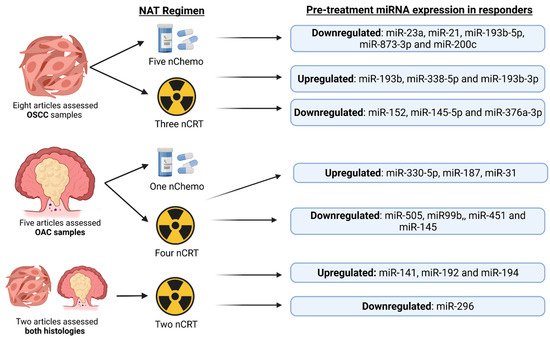
Oesophageal cancer (OC) is the ninth most common cancer worldwide. Patients receive neoadjuvant therapy (NAT) as standard of care, but less than 20% of patients with oesophageal adenocarcinoma (OAC) or a third of oesophageal squamous cell carcinoma (OSCC) patients, obtain a clinically meaningful response. Developing a method of determining a patient’s response to NAT before treatment will allow rational treatment decisions to be made, thus improving patient outcome and quality of life. MicroRNAs are valuable biomarkers of response to NAT in OC. Research is needed to understand the effects different types of chemotherapy and chemoradiotherapy have on the predictive value of microRNAs; studies also require greater standardization in how response is defined.
- oesophageal adenocarcinoma
- oesophageal squamous cell carcinoma
- predicting response
- chemotherapy
- chemoradiotherapy
- neoadjuvant therapy
- microRNAs
1. Introduction
1.1. Oesophageal Cancer Epidemiology
1.2. Pathophysiology of OAC and OSCC
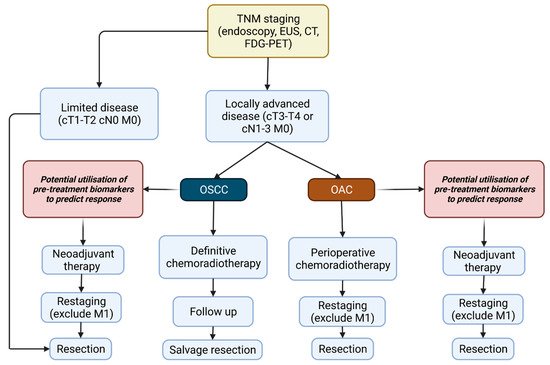
1.3. Current Pathways of Screening
1.4. Treatment of Oesophageal Cancer
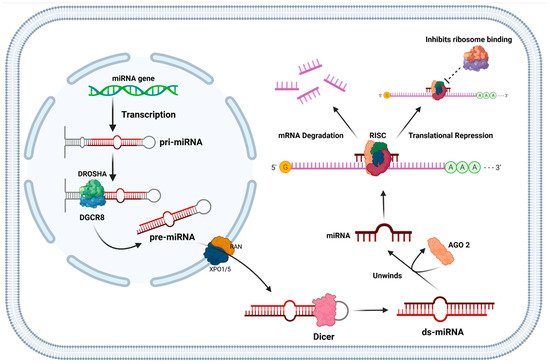
1.5. Function of miRNAs and Their Role in Cancer
2. Current Insights
Current Use of miR-21, miR-193b and miR-200c in Cancers and Their Functional Roles
This entry is adapted from the peer-reviewed paper 10.3390/cancers14051171