Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Oncology
Timely palliative care is a systematic process to identify patients with high supportive care needs and to refer these individuals to specialist palliative care in a timely manner based on standardized referral criteria.
- delivery of health care
- health care quality
- access and evaluation
- implementation
1. Introduction
Patients with cancer encounter significant supportive care needs throughout the disease trajectory, starting from the time of diagnosis [1]. These supportive care needs fluctuate with time and may include physical, psychological, social, spiritual, informational and financial concerns, often overlapping with each other, compromising patients’ quality of life. The demand for supportive care services increases with an aging patient population who often have multiple comorbid diagnoses. Moreover, there is a heightened need for supportive care in the era of novel cancer therapeutics, as patients are living longer while experiencing more chronic symptoms and adverse effects [2,3].
Over the past few decades, multiple supportive care programs have evolved to address these growing patient care needs [1]. In particular, there has been substantial development in specialist palliative care teams that provide interdisciplinary, holistic care for patients with cancer and their families [4,5,6]. Multiple randomized controlled trials have found that compared to primary palliative care provided by oncologists, early referral to specialist palliative care can improve patients’ quality of life, symptom control, mood, illness understanding, end-of-life care and survival [7,8,9,10,11,12,13]. Meta-analyses over the past 5 years have consistently reported the benefits associated with specialist palliative care [14,15,16,17,18] (Table 1). To date, the evidence on primary palliative care remains limited [19,20,21]. Thus, the focus of this article is on delivery of timely specialist palliative care.
Table 1. Meta-analyses on the outcomes of specialist palliative care for patients with cancer.
| Setting | No. of Studies | No. of Patients | Quality of Life SMD (95% CI) |
Symptoms SMD (95% CI) |
Mood SMD (95% CI) |
Survival HR (95% CI) |
|
|---|---|---|---|---|---|---|---|
| Kavalieratos et al. 2016 [16] | IP/OP | 11 | 1670 | 0.12 (−0.2, 0.27) |
−0.14 (−0.39, 0.10) |
0.82 (0.60, 1.13) | |
| Gartner et al. 2017 [14] | IP/OP | 5 | 828 | 0.20 (0.01, 0.38) |
−0.21 (−1.35, 0.94) |
||
| OP (early only) | 2 | 388 | 0.33 (0.05, 0.61) |
||||
| Haun et al. 2017 [15] | OP | 7 | 1614 | 0.27 (0.15, 0.38) |
−0.23 (−0.35, −0.10) |
−0.11 (−0.26, 0.03) |
0.85 (0.56, 1.28) |
| Heorger et al. 2019 [17] | OP | 8 | 2092 | 0.18 (0.09, 0.28) |
1y: 14.1% (6.5%, 21.7%) |
||
| Fulton et al. 2019 [18] | OP | 10 | 2385 | 0.24 (0.13, 0.35) |
−0.17 (−0.45, 0.11) |
−0.09 (−0.32, 0.13) |
0.84 (0.61, 1.18) |
Abbreviations: CI, confidence interval; HR, hazard ratio; IP, inpatient; OP, outpatient; SMD, standardized mean difference.
2. What Is Timely Palliative Care?
Timely palliative care is a systematic process to identify patients with high supportive care needs and to refer these individuals to specialist palliative care in a timely manner based on standardized referral criteria [23]. It requires four components: (1) routine screening of supportive care needs at the oncology clinics, (2) establishment of institution-specific consensual criteria for referral, (3) having a system in place to trigger a referral when patients meet criteria, and (4) availability of outpatient palliative care resources to provide timely access (Figure 1).
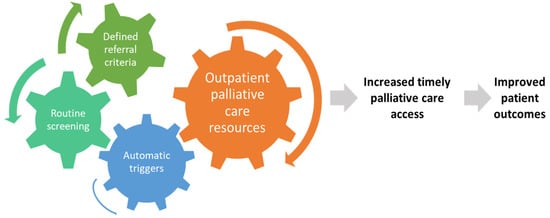
Figure 1. Conceptual model for timely palliative care. Timely palliative care has four key components: routine systematic screening, a defined set of referral criteria, a mechanism to trigger referral for appropriate patients, and an adequately staffed outpatient specialist palliative care clinic. The expected outcome is a greater number of patients receiving specialist palliative care and earlier timing of referral, which would lead to improved patient outcomes such as quality of life, quality of end-of-life care, and possibly survival.
3. How Is Timely Palliative Care Different from Early Palliative Care?
The concept of early palliative care is exemplified in the landmark Temel trial, in which patients with metastatic lung cancer were referred to palliative care within 2 months of diagnosis [24]. Although what constitutes “early” has not been established, randomized trials on early palliative care typically involved patients within 2–3 months of diagnosis of advanced diseases and had an ECOG performance status of 2 or less [7,9,10,11,25,26,27,28]. Patients referred within this timeframe are typically considered to have early palliative care involvement. Of note, patients did not need to have supportive care needs to qualify for a palliative care referral in these trials. However, a recent secondary analysis of the Zimmermann trial found that patients with higher symptom burden at baseline were more likely to derive a benefit from the palliative care intervention [29].
Due to the scarcity of palliative care resources, it is not possible to provide early palliative care for all patients with advanced disease from around the time of diagnosis [30]. Moreover, some patients may not require specialist palliative care initially due to low supportive care needs or their needs have been adequately addressed by the oncology team. In contrast to early palliative care, which initiates referral based on disease trajectory, timely palliative care is referral based on needs. Similar to early palliative care, timely palliative care is often initiated in the outpatient setting and provided to a majority of patients early in the disease trajectory.
Timely palliative care is early palliative care personalized around patients’ needs and delivered at the optimal time and setting [4]. Similar to the concept of targeted therapy, oncologists may only offer treatment for selected patients with “targetable mutations” instead of treating all patients. This approach provides a more rational use of resources, minimizes unnecessary exposure to those who may be less likely to benefit, and maximizes the impact on patients offered the intervention [29].
4. Rationale for Timely Palliative Care
Although specialist palliative care teams have significant expertise managing complex symptom crises that often occur in the last months of life, palliative care interventions are best provided proactively to prevent suffering [22,23]. Optimal timing is especially important as it allows specialist palliative care teams to more effectively introduce symptom management, provide psychological support and facilitate care planning. At MD Anderson Cancer Center, the median time from outpatient palliative care referral to death is over 12 months [31]. This allows the palliative care team to have multiple visits with patients and provide comprehensive care longitudinally.
Palliative care teams can provide a variety of non-pharmacologic and pharmacologic measures to alleviate symptoms such as pain, dyspnea and nausea when they first present. Subsequent visits can allow the palliative care team to optimize symptom control by providing therapeutic trials, active titration, proper education, longitudinal monitoring, and reinforcement of treatment adherence [32,33]. Successful symptom management not only improves quality of life, but also prevents escalation of symptoms leading to avoidable emergency room visits and hospitalizations [34,35]. Optimization of physical symptoms such as fatigue and anorexia–cachexia may also allow patients to better tolerate cancer treatments. Indeed, a higher baseline quality of life is associated with improved overall survival and progression-free survival for patients undergoing chemotherapy [36,37].
In addition to physical symptoms, timely palliative care referral allows for optimal psychological care to be delivered over time. It takes time for the palliative care team to establish trust, rapport, and explore the layers of emotional and existential concerns. Acute issues (e.g., severe pain, delirium) often need to be addressed first before chronic psychological issues can be managed. Moreover, many evidence-based interventions to treat depression and anxiety, such as counseling and exercises, require weeks and months to take effect [38,39]. In addition to patients, family caregivers benefit from building longitudinal relationships with the palliative care team so they can receive the proper education, psychologic care and resources to better support the patients throughout the disease trajectory [40,41].
Similar to symptom management and psychosocial care, serious illness conversations should start well before the last months of life because patients often require time to digest prognostic information and actively prepare for the future [42,43,44]. Palliative care teams have specialized training in communication skills to facilitate discussions around sensitive subjects such as prognostic disclosures, goals-of-care conversations and advance care planning. These discussions are longitudinal by nature and need to be timed carefully. Decisions regarding end-of-life care initiated by an oncology team are best followed by an interdisciplinary team to optimize goal-concordant care. Studies have found that early palliative care not only improves illness understanding, but also quality of end-of-life care by reducing chemotherapy use, emergency room visits, hospitalizations, intensive care units admissions in the last month of life [10,45].
This entry is adapted from the peer-reviewed paper 10.3390/cancers14041047
This entry is offline, you can click here to edit this entry!