Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Orthopedics
Osteoarthritis (OA) can be defined as the result of pathological processes of various etiologies leading to damage to the articular structures. Although the mechanism of degenerative changes has become better understood due to the plethora of biochemical and genetic studies, the drug that could stop the degenerative cascade is still unknown. All available forms of OA therapy are based on symptomatic treatment.
- osteoarthritis (OA)
- pharmacotherapies
- disease-modifying drugs for osteoarthritis (DMOADs)
Arthritis is classified into various types, including osteoarthritis, rheumatoid arthritis (RA, ICD-10-CM code: M06 [1]), gouty arthritis, septic arthritis (SA), and psoriatic arthritis (PsA). Among them, RA and OA are the most common types of arthritis in the human population affecting about 302 million people [2]. Hallmarks of RA include inflammatory changes in the synovial membranes and articular structures, widespread fibrinoid degeneration of the collagen fibers in mesenchymal tissues as well as atrophy and rarefaction of bony structures. RA can also affect body parts other than joints, such as the eyes, mouth, and lungs. The etiology of RA is unknown, but most commonly autoimmune mechanisms have been implicated. In autoimmune diseases, the body’s immune cells attack the body’s tissues [3]. On the other hand, OA (ICD-10-CM code: M15-M19 [4]) is a complex, multifactorial disease. It can occur in any joint, mainly targeting the major joints (knee, hip, and back); nevertheless, it commonly affects hands, elbows, and ankles [5]. It is characterized by degeneration of the articular cartilage that ultimately leads to joint destruction [6]. The pathological changes of OA involve the entire joint, which is composed of multiple types of tissues and cells, exemplified by cartilage degradation, subchondral bone thickening, osteophyte formation, synovium inflammation, and hypertrophy, as well as ligament degeneration [7,8]. Both RA and OA commonly cause chronic pain, reduce motion in joints, and will become more prevalent given the aging population [9]. They have several underlying causes, including biochemical and mechanical factors [10,11]. In general, these diseases are progressive and no widely applied effective therapy is available [12].
Arthritis is managed pharmacologically and non-pharmacologically, including common pharmacotherapies, surgery, and lifestyle changes. Initially, the therapy should be based on non-pharmacological methods, such as weight reduction, improvement of special exercises, and orthoses. This first step is often overlooked or insufficiently emphasized, to the detriment of patients [13]. Pain medications, including the most popular NSAIDs, are the first-line treatment [14]. However local treatment has been used more widely, which in the hierarchy of proceedings takes place between rehabilitation and pharmacological treatment. Surgery should be considered only in the case of insufficient improvement and the presence of advanced lesions visible in imaging tests.
3. The First-Line Therapy of Osteoarthritis
Nonpharmacological interventions, in parallel to the pharmacological treatment modalities, have been recommended for the management of OA and associated comorbidities [26]. The American Academy of Orthopaedic Surgeons (AAOS) published the guidelines to assist in making evidence-based decisions in the conservative management of hip and knee OA [27,28]. Moreover, other scientific societies, such as The European League Against Rheumatism (EULAR), the OsteoArthritis Research Society International (OARSI), and the American College of Rheumatology (ACR), have developed various recommendations for treating OA, depending on its location [2,29,30]. The pharmacological approach in symptomatic OA management mainly focuses on improvement or control of symptoms, pain, and underlying inflammation resulting in a reduced need for rescue analgesia and joint replacement surgery.
Before starting therapy, each patient should be assessed for medical conditions, such as hypertension, cardiovascular disease, heart failure, risk of gastrointestinal bleeding, chronic kidney disease, or other comorbidities, as well as trauma, disease severity, and surgical history that may affect the risk of side effects of certain pharmacological agents [2].
Drugs available for the treatment of OA (ATC code: M01-M09 [31]) include topical products for joint and muscular pain (ATC code: M02A [32]). The most frequently used preparations are the ATC subgroup M02AA [33], which includes anti-inflammatory, non-steroidal drugs (NSAIDs), e.g., those listed in Figure 1. Recently, pharmacological therapy is broadened by so called disease-modifying drugs for osteoarthritis (DMOADs) and symptomatic slow-acting drugs for osteoarthritis (SYSADOA) [34]. The initial oral medication of choice in the treatment of OA involves oral NSAIDs. Regardless, the anatomic location of pain must come before patients are recommended the available oral medications [2].
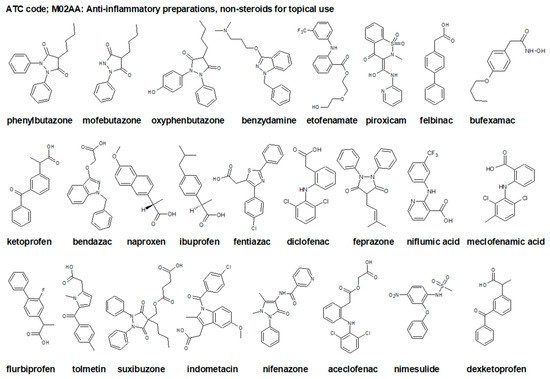
Figure 1. Chemical structures of selected non-steroidal anti-inflammatory drugs (NSAIDs), topical drugs for joint and muscle pain ATC code: M02AA [33].
The ultimate goal for the OA treatment would be to halt the disease progression and repair the cartilage damage and relieve pain. However, effective cures are not currently available and recommendations for treatment vary. OA has multiple etiologies and interconnecting pathways; therefore, targeting only one molecule does not seem to become the effective treatment [5]. Due to this, it is highly unlikely to use a single medication effectively treating these diseases. OARSI and EULAR guidelines recommend that if patients do not respond to oral analgesics, they should receive intra-articular injections of either corticosteroids or hyaluronate followed by the use of opioids and narcotics only when all other pharmacological options have been considered [2,29,30,35].
. Platelet-Rich Plasma (PRP)/Platelet-Rich Fibrin (PRF) as Second Line Treatment
Platelets (PLT), also known as thrombocytes, are small cytoplasmic fragments (2 to 3 μm in diameter, volume between 5 and 10 fL (10−15 L (femtoliters) and the normal counts in peripheral blood (approximately 150–450 × 109 per liter volume of plasma)) [110]). They are derived from bone marrow megakaryocytes. Numerous studies have established that they consist of more than 800 proteins and other molecules. These components are GFs (also known as the osteoinductive proteins), cytokines, chemokines, membrane proteins, metabolites, messenger molecules, and numerous soluble proteins [111].
PRP is defined as a volume of plasma with a platelet concentration (1 × 106 PLT/μL) in small volume of plasma (approximately 5 mL) higher than the average in peripheral blood [111]. According to this definition, PRP contains 2–9 folds more PLT per unit volume than normal blood. PRP is developed from autologous blood, it is inherently safe, and is free from transmissible diseases. It has been used successfully on tissue regeneration, due to the high concentration of GF contained in platelets [112]. GFs, which are being released from platelets α-granules enhance the regeneration of injured tissue. The α-granules are approximately 200 to 500 nm in diameter and contain over 30 bioactive proteins [113].
A review of the literature shows that the history of various PRP-based therapies is at least 70 years old. For this reason, it is widely accepted that the method is sufficiently well-established to allow widespread use in medicine, particularly in sports medicine, and orthopedics [114]. The use of PRP in the process of plasmapheresis in enhancing bone regeneration was described in 1999 by Anitua [115,116]. A recent meta-analysis of randomized controlled trials (RCT) evaluating the effects of PRP or intra-articular hyaluronic acid (IA HA) injections in patients with knee OA documented that PRP is an effective treatment that reduced pain and improved functional status [117,118].
In sum, PRP is an autologous orthobiologic treatment option for musculoskeletal conditions with favorable results in a limited number of high-quality clinical trials. PRP therapy is currently used to treat degenerative disorders and promote the healing of tendons, ligaments, muscles, and cartilage [114].
This entry is adapted from the peer-reviewed paper 10.3390/ijms23031566
This entry is offline, you can click here to edit this entry!