Children and adolescents with intellectual disabilities (ID) have low levels of physical activity (PA). Understanding factors influencing the PA participation of this population is essential to the design of effective interventions. Continued exploration of factors influencing PA participation is required among children and adolescents with ID. Future interventions should involve families, schools, and wider support network in promoting their PA participation together.
1. Introduction
Physical activity (PA) is defined as any bodily movement produced by skeletal muscles that requires energy expenditure [
1] and is characterized by its modality, frequency, intensity, duration, and context of practice [
2]. PA promotes numerous physical and mental health benefits in children, including children and adolescents with disabilities [
3,
4,
5]. Regular and adequate levels of PA can improve children’s cardiorespiratory and muscular fitness, bone health, and cardiovascular and metabolic health biomarkers, reduce symptoms of anxiety and depression, and help to maintain a healthy weight [
6]. Despite the physiological and psychological health benefits associated with PA participation, previous studies reported that children with intellectual disabilities (ID) did not meet the PA guideline of at least 60 min of moderate-to-vigorous-intensity physical activity (MVPA) per day [
7,
8,
9]. In addition, children and adolescents with ID are less active than their counterparts without disabilities [
10,
11].
2. Current Insights
2.1. Searching Results
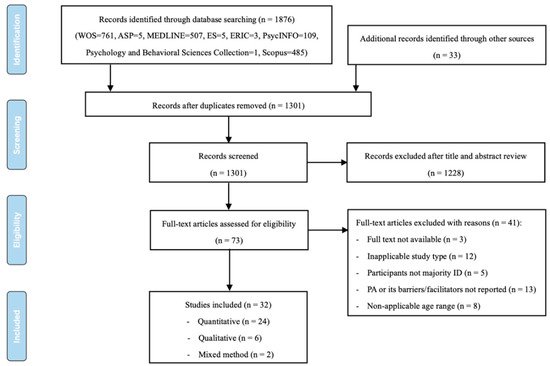
The initial search identified 1876 studies (WOS,
n = 761; ASP,
n = 5; MEDLINE,
n = 507; ES,
n = 5; ERIC,
n = 3; PsycINFO,
n = 109; Psychology and Behavioral Sciences Collection,
n = 1; Scopus,
n = 485). Thirty-three additional studies were identified through related reviews. After removing duplicates from the original sample (
n = 1909), title and abstract screening of 1301 articles was performed, from which 1228 studies were excluded. The researchers read the full text of the remaining 73 articles and excluded another 41. Finally, 32 studies were included in this review.
Figure 1, adapted from the PRISMA group [
32], displays the detailed search and study selection process.
Figure 1. Flowchart of search and study selection.
2.2. Study Characteristics
Table 1 summarizes the details of the studies that met the inclusion criteria. The final 32 articles selected for review were published between 1992 and 2020, 24 of which (75%) were published after 2010. These studies we conducted in the USA (12), UK (5), Canada (3), China (3), Australia (2), Iceland (1), Italy (1), the Netherlands (1), the Philippines (1), Saudi Arabia (1), Spain (1), and Trinidad and Tobago (1). A total of 24 studies employed quantitative methods of data collection, 6 used qualitative data collection methods, and the 2 remaining studies adopted mixed methods. Of the quantitative and mixed-method studies, 18 articles employed a cross-sectional design, 6 adopted intervention, one used a longitudinal design, and one utilized a case design. The six qualitative studies all employed a phenomenological design. Of the quantitative studies, 17 studies used objective measures including accelerometers (n = 11), pedometers (n = 3), heart rate monitors (n = 4), and quantitative observation (n = 6) to quantify PA. Nine studies used questionnaires as subjective measures. Two of the quantitative studies utilized more than one measurement tool. The intensity and duration of PA were presented as different ways due to different measurements. Among included quantitative studies, 17 studies used different PA dimensions including LPA, MPA, MVPA, and number of steps per day. Another 9 studies used regular PA, PA frequency, and PA perceptual characteristics based on subjective PA questionnaires. The qualitative studies used interviews (n = 4) and focus groups (n = 2) to explore the barriers and facilitators to PA among children and adolescents with ID. The mixed-method studies involved objective (e.g., accelerometers, quantitative observation, heart rate monitors) and subjective measurements (e.g., questionnaire, interviews). These two studies used different dimensions including MPA and MVPA. Of the 32 studies, 15 studies used a purposive sampling strategy, 10 studies used a convenience sampling strategy, and 7 studies did not provide an indication of the sampling strategy. The sample size ranged from 3 to 535, including one with more than 500 participants, 4 with 100 to 500 participants, 16 with 30 to 100 participants, and 11 with less than 30 participants. In all, 6 (19%) stated the use of theories, including social cognitive theory (n = 2), self-determination theory (n = 2), occupational perspective theory (n = 1), and dynamic systems theory (n = 1).
Table 1. Descriptive statistics of included studies.
2.3. Thematic Synthesis
The barriers and facilitators of PA participation among children and adolescents with ID are classified into three groups of studies using different research methods. Specifically, barriers and facilitators are presented under individual, interpersonal, and environmental levels of influence based on the social ecological model [
28] (
Table 2).
2.3.1. Barriers to Participating in PA
Qualitative Studies
The included qualitative studies identified barriers to PA participation among children and adolescents with ID based on the perceptions of parents, teachers, and adolescents with ID. Any dimension of PA was not available in these studies. At the individual level, the results of studies showed that conditions associated with ID, such as developmental delays [
57], ear problems [
49], and common characteristics associated with DS (including hypotonia, congenital heart defects, and communication impairments) [
51] were identified as physiological factors that inhibited PA participation in children and adolescents with ID. Low self-efficacy [
38] and lack of understanding on the importance of PA and its benefits for health [
48] were identified as cognitive and psychological barriers to PA participation. Interpersonal factors are related to interpersonal processes and primary groups, such as family and peers [
63], influencing PA participation among children and adolescents with ID. Lack of parental support (including lack of parents’ company [
46,
51], lack of family’s financial support [
46,
57], lack of transport support [
49], lack of information for parents on how to conduct home-based activities [
57]), and parent’s vigilance and overprotection [
46,
51] were identified as family barriers to PA participation among children and adolescents with ID. In addition, lack of social networks (e.g., lack of social connectedness with others) was also identified as an interpersonal barrier to PA participation among children and adolescents with ID [
38]. At the environmental level, inadequate or inaccessible facilities [
46] and lack of appropriate programs [
51,
57] were identified as social environmental barriers to PA participation among children and adolescents with ID. Poor weather, as one of the natural factors, prevented this population from participating in outdoor activity and thus decreased their PA [
38,
46].
Quantitative Studies
At the individual level, low motor development (e.g., low locomotor and object control skills) [
9,
33,
45] was identified as a barrier that influenced MVPA or the number of steps per day among children and adolescents with ID. Low self-efficacy [
43] and a preference for indoor activities [
62] were identified as cognitive and psychological barriers that influenced regular PA and rating perceived exertion of PA participation among children and adolescents with ID. At the interpersonal level, lack of a social network (e.g., have fewer friends) was identified as a barrier that influenced regular PA among children and adolescents with ID [
43]. At the environmental level, teacher and classroom-related factors were examined in previous studies. The results of the study found that lesson contexts organized by PE teachers (e.g., allocating the substantial amount of lesson time for management) and teaching behaviors (e.g., spending considerably more time transmitting physical education (PE) knowledge), which reduced opportunities for students to participate in MVPA, were identified as barriers [
56].
Mixed-Method Studies
Lack of parental support [
59] and lack of public transportation [
59] were, respectively, identified as barriers at the interpersonal and environmental levels that influence MPA among children and adolescents with ID in one study using mixed methods.
Table 2. Barriers and facilitators identified of PA participation among children and adolescents with ID.
2.3.2. Facilitators of Participating in PA
Qualitative Studies
Facilitators of PA participation among children and adolescents with ID reported by the included qualitative studies were also identified from perceptions of parents, teachers, and adolescents with ID. At the individual level, physical skills were identified as facilitators of participating in PA among children and adolescents with ID [
51]. Cognitive and psychological factors, such as high self-efficacy [
38], enjoyment of PA [
48,
49], and personality traits (e.g., enthusiastic and determined) [
51] were also facilitators. At the interpersonal level, sufficient parental support (e.g., parents’ positive role model, parental company and logistic supports) [
38,
48,
49,
51,
57], positive role of siblings [
51,
57], and positive social interactions with peers [
38,
49,
51,
57] were identified as facilitators of participating in PA among children and adolescents with ID. At the environmental level, PA programs available in the community adapted for children and adolescents with ID were identified as social environment facilitators of participating in PA among children and adolescents with ID [
51]. Attending PE classes [
38], teaching methods, and a strong home-school link [
48] were identified as school environment factors of participating in PA among children and adolescents with ID.
Quantitative Studies
At the individual level, physical skills (e.g., riding a bicycle) were identified as physical ability factors that influence MVPA among children and adolescents with ID [
53]. Wanting to lose weight [
40], high self-efficacy [
43], and enjoyment of PA [
43,
44] were identified as cognitive and psychological facilitators that influence PA frequency, regular PA, LPA, and MPA among children and adolescents with ID. In addition, caregiver’s higher educational level was another individual facilitator that influenced regular PA among children and adolescents with ID [
54]. At the interpersonal level, sufficient parental support (e.g., parents’ company) [
37] and positive parental beliefs of the benefits of PA for their child [
41] were identified as family factors that influence PA frequency among children and adolescents with ID. In addition, positive social interactions with peers [
11,
52] and positive relationships with the coach [
37] were identified as social network facilitators that influence PA frequency among children and adolescents with ID. At the environmental level, an exergaming context implemented at home or at school was identified as a facilitator that influenced MVPA among children and adolescents with ID [
34]. Adequacy and availability of environmental resources (e.g., access to transportation) were identified as social environment factors that influenced PA frequency among children and adolescents with ID [
37]. PA programs available in the community adapted for children and adolescents with ID were also identified as facilitators that influenced LPA and MVPA among children and adolescents with ID [
50,
53]. In terms of school factors, attending PE classes and participating in physical activities during school recess [
40,
42,
45,
47,
55,
58,
60,
61] were identified as key facilitators that influenced MVPA or number of steps per day among children and adolescents with ID. Inclusive PE programs (e.g., a peer-tutored PE program) [
35] were also identified as school facilitators that influenced the LPA and PA frequency of children and adolescents with ID. In addition, high autonomy-supportive instructional climates [
36] and PE lesson contexts focused on skill practice [
56] were identified as facilitators that influenced MVPA among children and adolescents with ID.
Mixed-Method Studies
An adapted PA program using group video conferencing for the promotion of PA [
39] was identified as a facilitator that influenced MVPA among children and adolescents with ID at the environmental level.
Qualitative studies help to explore and understand full-breadth issues in relation to the PA participation experienced by a specific population [
23]. Therefore, it would be best suited to the profound exploration of the specific barriers and facilitators of PA participation among children and adolescents with ID [
68]. However, only 19% (
n = 6) of the studies included in this review employed a qualitative research design. Qualitative studies are needed to address how children and adolescents with ID participate in PA and why their PA levels are lower than their peers without disabilities [
47,
69]. Theoretical frameworks were designed to help comprehensively understand the relationship between factors and the mechanisms by which they affect behavior [
22]. However, only 19% (
n = 6) of the research used a theoretical framework to guide their studies. Studies using the behavioral theoretical frameworks are urgently needed to better understand healthy behavioral patterns and guide the development of effective interventions to promote PA among children and adolescents with ID [
22,
66].
Based on the social ecological model, our synthesis of the studies identified 34 factors primarily related to individual, interpersonal, and environmental elements at several levels of influence.
3. Conclusion
Based on the social ecological model, our synthesis of the studies identified 34 factors primarily related to individual, interpersonal, and environmental elements at several levels of influence. Disability-specific factors, low self-efficacy, lack of parental support, inadequate or inac-cessible facilities, and lack of appropriate programs were the most commonly reported barriers. High self-efficacy, enjoyment of PA, sufficient parental support, social interaction with peers, attending school PE classes, and adapted PA programs were the most commonly reported facilitators. Given the findings from this scoping review, there is a need for continued exploration of the barriers and facilitators of PA participation among children and adolescents with ID by more qualitative, longitudinal, and interventional studies. By understanding the relationships between barriers and facilitators and the different dimensions of PA, interventions can be better designed and adapted to en-courage greater PA participation for children and adolescents. Such work may be vital to improve this population’s health and growth.
This entry is adapted from the peer-reviewed paper 10.3390/healthcare10020233