Professional training is defined as a set of behaviors and acts with the purpose of increasing the employees’ professional skills to carry out a particular job in a better manner. Such a definition highlights three important features of professional training. First, its purpose is educational, which focuses on employee development (e.g., skill acquisition and knowledge growth) rather than performance improvement.
Augmented reality (AR) is defined as a technology-enhanced environment where virtual objects (augmented components) can be overlaid into the real world. Azuma (1997) identified three technical features of AR: a combination of the real and virtual world, real-time interaction, and accurate 3D registration of virtual and real objects.
1. Introduction
Professional training differs from K–16 education in its educational focus and pedagogy. While K–16 education focuses more on students’ learning outcomes and academic achievements, professional education is more career-oriented, concerning the cost-effectiveness of the training program. Consequently, K–16 education often relies on the student-centered pedagogy to promote higher-order thinking and meta-cognitive skills [
10], whereas professional training is more aligned with skill development featured by direct instruction and trial-and-error practice [
11]. The literature highlights the importance of professional training as it has a positive impact on employees’ working attitudes, job performance, and knowledge acquisition [
6,
12].
The aforementioned characteristics of professional training highlight the potential of AR as a proper instructional technology for this particular context. First, AR enables the natural integration of virtual instructional content into the actual working environment [
13], which can promote situational cognition and experiential learning. For example, Abhari et al. (2015) described an authentic AR-enhanced surgery environment where novice physicians can improve their neurosurgical skills through hands-on practice [
14]. Second, AR can provide a variety of visual cues in the digital forms of symbols, text, animation, or 3D objects, which are known to facilitate procedural learning in professional training [
15]. Third, AR can facilitate a shared learning experience in groups owing to increased visibility of virtual content [
16]. The ability to accommodate group learning can further improve the accessibility and feasibility of AR-supported professional training. Lastly, the digital artifacts afforded by AR allow for easy creation, modification, and duplication, which can greatly reduce the training cost for trial-and-error practice.
2. Computing Devices
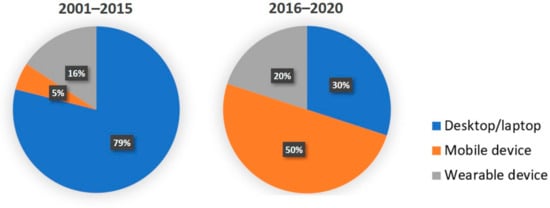
In professional training, data in AR systems were processed by three main types of devices: the desktop or laptop, mobile devices (including tablets, phones, and other handheld devices), and wearable devices.
Figure 5 shows a decreasing trend in desktop and an increase in mobile devices, consistent with technological advancements. In the first 15 years in the 21st century, the desktop/laptop had an overwhelming advantage over other computing devices, owing to the function of performing complex mathematical operations, satisfying the needs of simulation and calculation of AR systems. Meanwhile, in the last five years, portable devices, such as mobile or wearable devices, gradually replaced desktops and were used in some creative AR programs. For instance, Phan and Choo (2010) introduced an AR system in architectural education. For the convenience of virtual architecture representation, a set of wearable devices was designed for learners so that they could freely move in the scenario, which was combined with virtual images and real outdoor scenes, so as to help learners deeply understand the structure of the architecture and accept training [
34].
Figure 5. Computing devices of AR-supported instruction in the periods of 2001–2015 and 2016–2020.
3. Media Representation
In AR-supported instruction, the information carrier received by users had seven main forms, as shown in
Table 2. In terms of the total number, 3D object was the most common media representation, especially in health and medicine. For example, in anatomical education and dental morphology, AR was used to construct a 3D model of the skull or dental piece for students to learn about the structure and composition [
35,
36]. In addition, video and text were two other important information carriers. In surgical training, the real-time changes in the operating environment were represented in videos for monitoring, and trainees’ operating processes were also recorded by videos [
37,
38]. Furthermore, text was used as a scaffolding to assist students to complete training or learning in AR systems in engineering and other fields [
22,
30,
39]. Moreover, data occurred in health and medicine, recording the operating time, smoothness of the AR simulator, and the needle position [
25].
Table 2. Media presentation of AR-supported instruction in three disciplines.
| |
Symbol/
Indicator |
Text |
Data |
2D Image |
3D Object |
Video |
Animation |
Mixed |
Total |
| >Engineering |
1 |
4 |
0 |
3 |
8 |
5 |
4 |
4 |
29 |
| Health and medicine |
2 |
3 |
3 |
4 |
16 |
6 |
2 |
8 |
44 |
| Other |
1 |
4 |
0 |
2 |
3 |
1 |
0 |
4 |
15 |
| Total |
4 |
11 |
3 |
9 |
27 |
12 |
6 |
16 |
88 |
4. Instructional Design
4.1. Pedagogy
In order to ensure the effectiveness of AR technology in professional training, it is essential to understand the pedagogy in AR intervention [
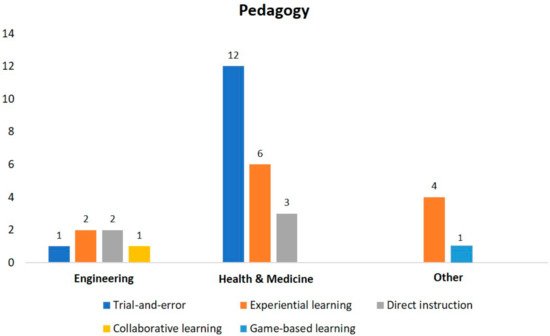
40]. Over the past two decades, four pedagogies were found to be used in three main disciplines of professional design; however, their frequency of applying was different owing to instructional contexts and teaching content. Much of the research was design case, not applicable to the pedagogy, thus the number of papers in each category was less than the total number, especially in the field of engineering.
As seen in
Figure 6, AR technology mainly served two pedagogies: trial-and-error (
n = 13) and experiential learning (
n = 12), which were consistent with the employment-oriented feature of professional training. Trial-and-error was defined as a process of repeated attempts with or without improvements by learning from failures [
41]. It was found to be the most used pedagogy in health and medicine and was in line with the features of medical education, which required repeated operation practice to improve behavioral and practical achievement. For example, in health and medicine, residents used the AR simulator to operate based on the checklist. In this process, the instructor assigned the tasks, observed students’ operating behaviors, and recorded their operating time and accuracy [
14,
42,
43].
Figure 6. Pedagogies guiding AR-supported instruction in three disciplines.
Another pedagogy that was used frequently, experiential learning, argued that knowledge is created and required through the transformation of experience, and knowledge results from the combination of grasping and transforming experience [
44]. Compared with trial-and-error, experiential learning focused on not only learners’ behavioral performance and skills, but the cognitive aspect of professional training, such as learning by doing, transfer learning, and reflection [
19]. In AR-supported professional training, learners interacted with the AR system, then completed a questionnaire about the acceptance and satisfaction of AR intervention, and even participated in an interview to reflect their learning experience [
22,
30,
45].
4.2. Types of Learning Outcomes
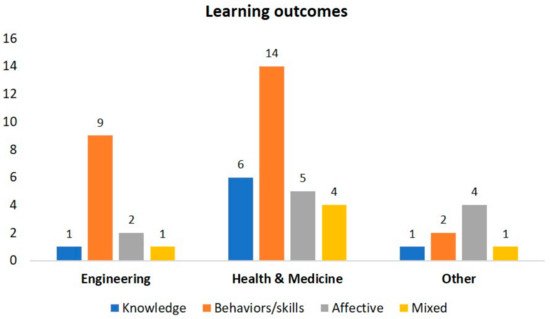
Figure 7 reveals learning outcomes by discipline in the perspectives of knowledge, behavior, and affection. In engineering and health and medicine, students’ behaviors/skills received the most attention (
n = 23), such as trainees’ operating time, accuracy, and proficiency in the workshop or simulated operating table [
33,
37,
46,
47,
48,
49]. In fact, this result depended on the characteristic of engineering and medical education, which emphasized practical operation skills. Moreover, some research focused on students’ knowledge level (
n = 8), which was measured by traditional exams before or after AR-supported instruction, to test the degree to which students had mastered new knowledge [
35,
50,
51,
52]. Another important finding is that affective outcomes (
n = 11) were also noted in selected papers, such as their learning experience, motivation, and attitude to the AR intervention [
30,
53,
54,
55]. These affective achievements were commonly measured by questionnaires, interviews, or scales. Moreover, some papers focused on multiple learning outcomes simultaneously (
n = 6), mixing their knowledge, behaviors, and affection, focusing on students’ comprehensive development [
36,
52,
56,
57,
58].
Figure 7. Learning outcomes in AR-supported instruction in three disciplines.
4.3. Instructional Function and Interactivity
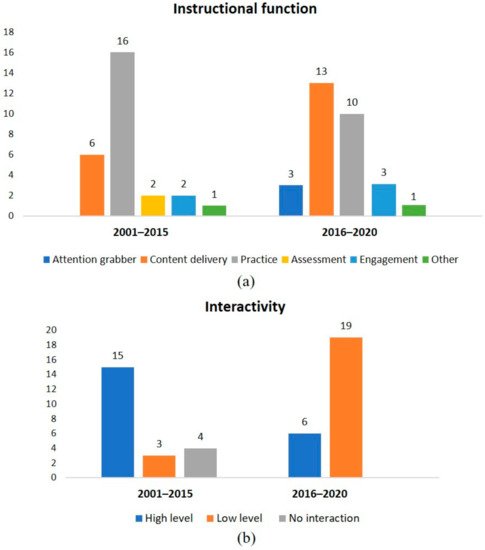
The instructional function of AR intervention was divided into six types, among which content delivery and practicing accounted for most percentages and indicated significant changes in the 20 years. As seen in
Figure 8a, the function of practice was far more than other functions in the first 15 years, consistent with the learning outcome of behaviors. Since 2016, practicing function decreased and the function of content delivery had a large growth and reached the top. In fact, the instructional function trend could be explained by the change in interactivity (
Figure 8b). In the first 15 years, the AR system was of a high level of interactivity, so it could support student training and practice. From 2016 to 2020, the AR system in professional training improved substantially in technological development and could realize more educational functions. For example, a complete AR system could be provided as a representation tool to present and simulate something invisible to assist content delivery [
35,
36,
52,
58]. In this case, the main function was not to promote practice, so the degree of interactivity was lower.
Figure 8. (a) Instructional function of AR-supported instruction in two periods of 2001–2015 and 2016–2020; (b) AR interventions by level of interactivity.
This entry is adapted from the peer-reviewed paper 10.3390/app12031024