Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Oncology
Pediatric brain tumors represent the most common types of childhood cancer and novel diagnostic and therapeutic solutions are urgently needed. Nanoparticles have been increasingly and thoroughly investigated as they show great promises as diagnostic tools and vectors for gene/drug therapy for pediatric brain cancer due to their ability to cross the blood–brain barrier.
- Lipid
- Nanoparticles
- Pediatric Brain Tumors
- Nano-Systems
1. Introduction
Central nervous system (CNS) tumors represent the primary cause of cancer-related death in children [1][2][3]. Treatment modalities include surgery, radiotherapy, and chemotherapy with outcomes largely depending on the biological aggressiveness of the disease and marginal improvement in the last decade [4]. Delivering diagnostic and therapeutic agents to central nervous system represents a critical challenge due to the presence of the blood–brain barrier (BBB) that represents a dynamic, semi-permeable barrier whose function is to protect nervous system microenvironment from pathogens or toxins, separating blood from brain [5]. The tight junctions between endothelial cells along with the basal membrane, characterized by laminin, collagen, and fibronectin, in which contractile pericytes are located, limit the passage or transport of solutes. Additionally, in the BBB astrocytic end-feet are also involved in blocking the free diffusion of molecules. Moreover, some brain regions as the pons have a more restrictive BBB towards the entry of molecules compared with other brain areas, this may have significant consequences for preclinical drug penetration studies and for the treatment of CNS tumors, particularly in diffuse intrinsic pontine glioma (DIPG) [6]. Moreover, BBB allows the passive diffusion of small size molecules such as the indispensable gas oxygen, water, and some hydrophobic solute, as well as lipophilic molecules with a positive surface charge, the latter representing the majority of current diagnostic and therapeutic agents. Meanwhile, the passage of polar components is only permitted by the presence of specific carriers through an active transport (i.e., glucose and amino acids) [7]. Additional BBB crossing mechanisms such as receptor-mediated transcytosis and adsorptive transcytosis occur, and they are currently being explored in order to expand the repertoire of drugs able to pharmacologically penetrate BBB [8]. For example, the most common modification of water-soluble drugs take place through the addition of lipid for allowing passive diffusion into the brain [9]; also, the development of peptide–drug conjugates with a transportable peptide such as insulin, transferrin, etc., through a disulfide bond. In this way, the resultant chimeric peptide is internalized through receptor-mediated transcytosis and then subjected to the action of disulfide reductases into the brain, thus allowing the cleavage and the release of the conjugated drugs [10]. Another strategy involves to the development of pro-drugs able to cross the BBB, which could be (bio)converted into the active drug once reached CNS. All these efforts highlight the urgent need of alternative solutions in pediatric neuro-oncology, and nanoparticles (NPs) can pave the way to novel therapeutic and diagnostic agents. In particular, the development of innovative NPs for early cancer detection is of paramount importance for the possibility of enlarging the therapeutic window, thus improving the prognosis. Nowadays, the routinely employed radiological imaging technique for diagnosing brain tumors is magnetic resonance imaging (MRI) based on gadolinium (Gd) complexes as a contrast agent. This approach is also exploited for surgical planning and surgical navigation, as well as for the postoperative assessments [11]. The clarity of brain cancer areas in gadolinium-based MRI mainly relies on the accumulation of contrast agents in the target region for its ability to cross the BBB alterations and irregularities in the tumor region [12][13]. However, the extent of BBB defects and openings that are responsible for its increased permeability is not equally distributed to the entire cancer edges in several fast-growing type of CNS tumors [14]. Consequently, gadolinium-based MRI could provide suboptimal tumor images, thus resulting in partial surgical debulking, whereas an extra wide resection could certainly positively affect the prognosis [14][15]. In a comparable manner, low-grade primary brain cancers show a low degree of BBB alteration, thus hindering clear tumor limit delineation that is of fundamental importance for successful surgical treatments [16]. Efficient gadolinium-based scans require a significant amount contrast agent; however, concerns about the toxicity of gadolinium-based complexes resulted in restriction of the use of some linear gadolinium for MRI body scans, and authorizations for others were suspended by the European Medicines Agency (EMA) in 2017, similarly the Food and Drug Administration (FDA) has also limited the use of gadolinium-based contrast agents [17][18]. Therefore, contrast agent based on nanotechnology could offer novel opportunities for early and accurate diagnosis, as well as being at the frontier of non-invasive tumor grading. NPs are characterized for their targeting ability directly to the site of interest with a spatio-temporal control of the payload release, additionally NPs can improve stability, bioavailability, and bioactivity of poorly exploited compounds because of their unfavorable pharmacokinetic profiles. Recently, liposomes, polymeric micelles, dendrimers, polymeric, and inorganic NPs have been proven to be effective for brain tumor treatment due to their ability to cross the BBB [19][20][21][22][23][24][25][26], similarly, engineered solid metal NPs such as iron oxide NPs, quantum dots, dendrimers, and lipid NPs have demonstrated their potential as diagnostic tools for the detection of brain cancers [27]. Despite this enormous potential, several factors have to be carefully evaluated as, for example, cell toxicity, clearance, and BBB flow out. Additionally, some clinical trials are still subject to approval and their application in the pediatric population is largely based on results in adults [28]. Routes of nanocarriers delivery in brain tumors.
Impermeability of the BBB is one well-known mechanism of chemotherapy failure in patients with CNS tumors, leading to an urgent clinical need for alternative strategies [29]. One of these approaches involves the intracerebroventricular and intrathecal administration, which allows a much lower dose of therapeutics when compared with systemic administration. Although this delivery strategy has been applied in pediatric brain cancers [30], it is associated with several limitations, such as the ineffective volume of drug, and it also has limited practicality or effectiveness for the treatment of intraparenchymal tumors. These issues can be addressed by using the convection-enhanced delivery (CED) in which intracranial catheters, stereo-tactically positioned to target sites of interest in the brain, can deliver therapeutic drug by exploiting convection instead of diffusion, over a period of time ranging from a few hours to days (Figure 1).
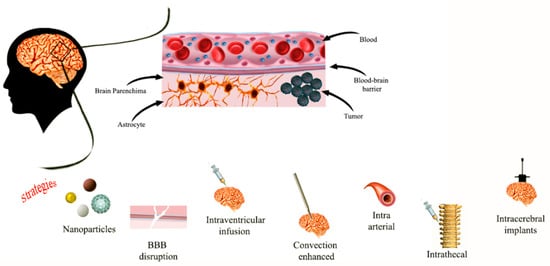
Figure 1. Representative images of different delivery routes to CNS.
2. Inorganic Nano-Systems for Pediatric Brain Cancer Diagnosis and Therapy
2.1. Gold Nanoparticles
Gold NPs (AuNPs) with a size < 10 nm are used in brain cancer diagnostic and treatments in order to deliver chemotherapeutic drugs, genes, or combined with radiotherapy [22][31]. AuNPs are FDA approved thanks to their small size, good biocompatibility, and the ability to cross BBB without causing damage [22]. Additionally, easy surface modification and controlled drug release make these NPs attractive [32]. AuNPs cross the BBB by passive diffusion (through ion channels such as Ca2+, Na+, and K+ channels), carrier-mediated and receptor-mediated transport (usually based on binding of transferrin modified AuNPs to transferrin receptor highly expressed on BBB epithelium cells) or adsorption mediated endocytosis [22]. Bredlau et al. reports the use of AuNPs conjugated with temozolomide as possible innovative treatment of recurring malignant glioma [33]. Another study [34] reports the efficiency of AuNPs for the delivery of doxorubicin (DOX) against human glioma cell lines, thanks to the employment of Agiopeptide-2 as targeting polymer and polyethylene glycol (PEG) to evade immune recognition (Figure 2).
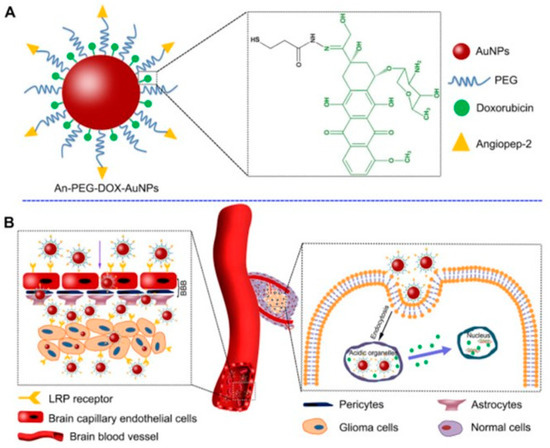
Figure 2. Scheme of the components of engineered AuNP functionalized with drug (green), targeting peptide (yellow) and components (A) and the delivery mechanism to glioma (B). Reprinted with permission from ref. [34]. Copyright 2014 Elsevier Ltd.
AuNPs are also exploited as adjuvant for radiotherapy since they increase DNA damage induced by ionizing radiation, as well as the blockage of angiogenesis. Joh et al. employed PEG-functionalized gold NPs coupled to the administration of ionizing radiation in human glioblastoma multiforme (GBM). The combination of these NPs and radiotherapy increased the survival of mice with orthotopic GBM tumors through a specific radio-sensitization [33][35][36]. For the possibility to finely control the physico-chemical properties of AuNPs (i.e., size, shape, and surface roughness), the resulting light absorption ability can be finely tuned, thus making AuNPs attractive for photothermal cancer therapy [37][38][39][40]. As, for example, photothermal therapy based on AuNPs-conjugated to RGD (arginine–glycine–aspartate) peptide were employed to target the integrins that are overexpressed in glioma cells in order to enhance the targeting [33][41]. In a similar manner, AuNPs functionalized with epidermal growth factor or transferrin receptors were loaded with the photosensitizer silicon phthalocyanine (Pc 4) and then employed in photodynamic therapy of glioblastoma. Through this strategy, cytotoxicity was reduced, and the efficacy of drug delivery was ameliorated [33][42]. In another study, AuNPs have been used to deliver short interfering RNA (siRNA) capable of crossing the BBB and to induce apoptosis; favorable outcomes were obtained, in particular a reduction in the tumor progression in xenografts models of GBM without side effects was clearly assessed. The biological target of this siRNA was the oncoprotein Bcl2Like12 (Bcl2L12), an effector caspase and p53 inhibitor overexpressed in GBM. This treatment caused tumor cells apoptosis by enhancing effector caspase and p53 activity [43][33]. Liu et al. have developed AuNPs coated by PEG, chitosan, and polyethyleneimine that were loaded with apurinic endonuclease 1 (Ape 1) siRNA for their successful delivery to pediatric ependymoma (EP) and medulloblastoma (MB) cells [44]. In another study, AuNPs were loaded with DOX and functionalized with PEG and the transactivator of transcription (TAT) in order to enhance the interaction between AuNPs and endothelial cell membranes. These NPs have shown accumulation in glioma cells and enhanced cytotoxicity in vitro and in vivo, when compared to DOX alone [22][45]. Different researches have also highlighted the potential of AuNPs as multifunctional tools for simultaneous brain cancer imaging and therapy. In particular, AuNPs could be used as diagnostic tool thanks their accumulation in the cancer brain tissue and, after irradiation, as therapeutic tools [35][46].
2.2. Silver Nanoparticles
Silver NPs (AgNPs) are colloidal metallic NPs widely employed in biomedicine [22][33]. The antibacterial and anticancer effects of AgNPs are mainly due to the release of Ag ions in tumor cells, thus leading to reactive oxygen species (ROS) generation and a subsequent oxidative damage to biological molecules that results in cell death [47][48]. More in details, AgNPs have a toxic effect on mitochondria with disruption of the respiratory chain, excessive oxidative stress, and inhibition of ATP synthesis, factors involved in the activation of apoptotic pathway. Furthermore, AgNPs with a diameter < 10 nm can cross the nuclear pores leading to ROS production and then, to cell cycle arrest and chromosomal aberration in glioblastoma cells [49], thus making attractive their application for increasing GBM cells apoptosis in vitro. In addition, AgNPs were used as sensitizers for radiotherapy [33]. Salazar-García et al. demonstrated the toxic effect of AgNPs and ZnCl2 in C6 rat glioma cells [50], showing a decrease in mitochondrial activity (about 13 and 21%, respectively) when used as single agents; on the other hand, combinatorial treatment with AgNPs and ZnCl2 decreased more significantly cell viability (around 30% administrating ZnCl2 as pre-treatment and 90% in concomitant administration) and led to an efficient apoptosis of C6 rat glioma cells [50].
2.3. Iron and Zinc Oxide NPs
Iron oxide (Fe3O4) NPs have extensive applications in cancer therapy as drug delivery agent or as magnetic guidance [33][51]. Fe3O4 NPs are biocompatible and biodegradable, and can be further functionalized in order to enhance biocompatibility, aqueous solubility, and to prolong their circulation time. Norouzi et al. [51], delivered DOX with bio magnetic Fe3O4 NPs (IONPs) for glioblastoma treatments (Figure 3).
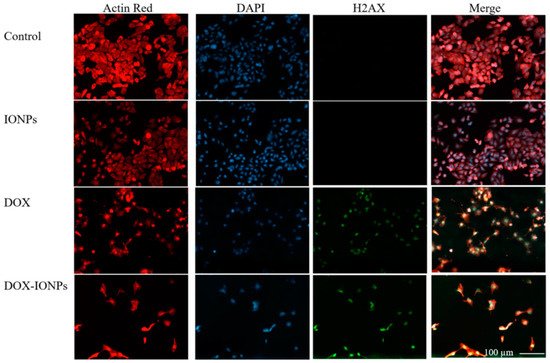
Figure 3. Fluorescent images of glioblastoma U251 cells after treatment with different formulations such as IONPs, DOX, and DOX loaded IONPs. Reprinted with permission from ref. [51]. Copyright 2020 Norouzi, M.; Yathindranath, V.; Thliveris, J.A.; Kopec, B.M.; Siahaan, T.J.; Miller, D.W.
Kievit et al. developed Fe3O4 NPs with a polymeric shell of chitosan, PEG, and polyethylenimine PEI that binded, protected, and delivered Ape 1 siRNA to perinuclear region of EP and MB cells, thus showing about 75% of down expression in pediatric tumor cells after radiation [52]. Duong et al. developed superparamagnetic Fe3O4 NPs (SPIONs) loaded with siRNA against MXD3 and observed cell apoptosis in neuroblastoma cell lines. In addition, Fe3O4 NPs loaded with MXD3 siRNA were combined with DOX, vincristine, cisplatin, or maphosphamide. Results showed an additive efficacy against neuroblastoma [53]. Iron oxide NPs have several advantages such as enhanced targeting, and delivering to diseased tissues via a magnetic field. Furthermore, once having been taken up by tumor cells, these NPs can be activated externally by alternating a magnetic field to destroy surrounding the target tissue through hyperthermia [54]. In this frame, SPION were coupled with an anti-EGFR antibody, which was expressed in human glioblastoma multiforme (GBM), and then used for MRI directed CED in cancer therapy [55]. Additionally, SPIONs represent a promising T2 MRI contrast agent that can persist for long time in the brain tissue, thus precisely defining the cancer edges with respect to gadolinium-based T1 MRI contrast agents [56][57]. Reddy et al. [58], developed a multifunctional SPION able to target glioma cells and to provide diagnostic images by using MRI and fluorescence. Their results showed the capability of this multifunctional SPION to penetrate the BBB and to mark brain cancer cells.
Another class of inorganic NPs is represented by zinc oxide (ZnO) NPs that are biocompatible and can be used for biomedical application [59][60]. The oral delivery of engineered ZnO NPs allows the brain to be reached and the BBB to be breached [47]. Wahab et al., showed that ZnO NPs present anticancer properties in the glioblastoma cell line [61]. The strong anticancer effect is due to induction of intracellular ROS generation and activation of apoptotic signaling pathway. Nonetheless, additional studies on ZnO NPs are required, including comparative analysis with other inorganic NPs, to better understand mechanism of potential toxicity in complex biological systems [59].
3. Lipid Based Nanoparticles in Pediatric Brain Tumors Treatment
Liposomes and micelles are organic NPs based on lipids that present different features: (i.) micelles are unilamellar NPs, smaller than liposomes, and are able to load hydrophobic therapeutics inside their structure or bound to their surface; (ii.) liposomes are composed by one or multiple lipid bilayers that form an internal aqueous compartment and a lipophilic external shell. Recently, liposomes have been exploited as drug delivery system against GBM [62], showing a good profile of biocompatibility and biodegradability, low toxicity, and the ability to load both hydrophilic and hydrophobic drugs [22][33][63]. There is evidence that highlights the ability of lipid NPs to accumulate in tumor tissue, due to the enhanced permeability and retention (EPR) effect [64]. The positively charged lipid-derived NPs are able to cross the BBB through adsorption-mediated transcytosis or endocytosis; liposomes conjugated with a specific BBB ligand, such as transferrin, insulin, or endothelial growth factor, can easily target the CNS by endocytosis mediated by a receptor [22][33][65]. Undoubtedly, one of the main drawbacks in the application of lipid NPs for pediatric brain cancers is represented by their rapid clearance. It has been demonstrated that liposomes conjugated with PEG evade opsonin recognition and the following clearance by the reticuloendothelial system (RES), thus prolonging their circulating time [33][47][66]. Many chemotherapeutic agents loaded into liposomes are involved in preclinical studies to treat brain cancers such as GBM, with respect to free drugs. These nanoformulations can accumulate in the tumor site, thus providing improved drug efficacy and lower toxicity [33][47]. Infante et al. developed amphiphilic self-assembling micelles to deliver Glabrescione B (Gla B), a hedgehog (Hh) inhibitor, which drastically inhibited tumor growth in both allograft and orthotopic models of Hh-dependent MB. It was demonstrated that micelles enhanced bioavailability of the poor water solubility of Gla B without the employment of organic solvents, thus obtaining favorable pharmacokinetics with negligible toxicity [67]. Bell et al. developed high density lipoprotein (HDL) NPs targeting the scavenger receptor class B type 1 (SCARB 1). Their results showed antineoplastic effects against the sonic hedgehog subtype of medulloblastoma (SHH-MB) (Figure 4), and potent inhibitor effects on the population of cancer stem cells, which is a result of the paramount importance in preventing tumor recurrence and therapeutic resistance [68].
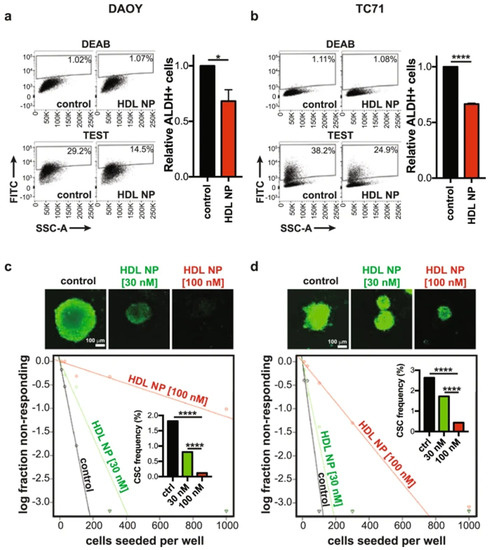
Figure 4. Flow-cytometry analysis of cancer stem cells reduction after treating DAOY cell line: (a) and TC71 cell line (b) with HDL NPs for 48 h. Spheroids obtained from DAOY (c) or TC71 (d) cells after dissociation were cultured with or without HDL NPs, in order to evaluate the formation of spheroids. Data are expressed as means ± SEM of 4 independent tests. * p ≤ 0.05, **** p ≤ 0.0001, and refer to unpaired, two-tailed t-test. Reprinted with permission from ref. [68]. Copyright 2018 Bell, J.B.; Rink, J.S.; Eckerdt, F.; Clymer, J.; Goldman, S.; Thaxton, C.S.; Platanias, L.C.
Additionally, Kim et al. developed biomimetic HDL NPs able to cross the BBB and deliver a SHH inhibitor (LDE 225) to cancer stem cell population of (SHH--MB) in vitro, ex vivo, and in vivo. These NPs were fabricated by incorporating with anti CD15 and apolipoprotein A1 to achieve a dual targeting delivery through binding of SCARB1 and CD15, both expressed by SHH MB cells. These NPs act as drug carriers and show a therapeutic effect due to efficient delivery of LDE 225, and for their intrinsic antineoplastic effect through SCARB1 intracellular cholesterol depletion in SHH MB cells [69][70]. Lipid-based NPs show many advantages like formulation simplicity, biocompatibility, and ability to load both lipophilic and hydrophilic drugs. However, despite these advantages, lipid NPs also show high uptake to the liver and spleen [71], which can induce a strong immune response. This limitation can be addressed via PEGylation of the nanoparticles [72] and, through modifications with cholesterol, it is possible to improve their stability and intracellular trafficking, and to reduce destabilization in the presence of serum [73][74].
Lipid-nanoparticles loaded with contrast agent can also represent an optimal strategy for the diagnosis of brain cancers thanks to their ability to promote the BBB passage of contrast complexes. Yang et al. [75] reported the synthesis of ultrasensitive magnetic resonance contrast agents for the imaging of brain cancers composed by a magnetic nanocrystals core and a coating of di-block of mPEG and dodecanoic acid. MRI investigation showed that these hybrid nanoparticles present good sensitivity against cancer cells with low toxicity in health cells.
This entry is adapted from the peer-reviewed paper 10.3390/diagnostics12010173
References
- Mueller, S.; Chang, S. Pediatric brain tumors: Current treatment strategies and future therapeutic approaches. Neurotherapeutics 2009, 6, 570–586.
- Fleming, A.J.; Chi, S.N. Brain tumors in children. Curr. Probl. Pediatr. Adolesc. Health Care 2012, 42, 80–103.
- Udaka, Y.T.; Packer, R.J. Pediatric Brain Tumors. Neurol. Clin. 2018, 36, 533–556.
- Pollack, I.F.; Jakacki, R.I. Childhood brain tumors: Epidemiology, current management and future directions. Nat. Rev. Neurol. 2011, 7, 495–506.
- Wu, L.; Li, X.; Janagam, D.R.; Lowe, T.L. Overcoming the blood-brain barrier in chemotherapy treatment of pediatric brain tumors. Pharm. Res. 2014, 31, 531–540.
- Warren, K.E. Beyond the Blood:Brain Barrier: The Importance of Central Nervous System (CNS) Pharmacokinetics for the Treatment of CNS Tumors, Including Diffuse Intrinsic Pontine Glioma. Front. Oncol. 2018, 8, 239.
- Zheng, W.; Aschner, M.; Ghersi-Egea, J.-F. Brain barrier systems: A new frontier in metal neurotoxicological research. Toxicol. Appl. Pharm. 2003, 192, 1–11.
- Bellettato, C.M.; Scarpa, M. Possible strategies to cross the blood-brain barrier. Ital. J. Pediatr. 2018, 44, 131.
- Sanchez-Covarrubias, L.; Slosky, L.M.; Thompson, B.J.; Davis, T.P.; Ronaldson, P.T. Transporters at CNS barrier sites: Obstacles or opportunities for drug delivery? Curr. Pharm. Des. 2014, 20, 1422–1449.
- Pardridge, W.M. Brain Drug Targeting and Gene Technologies. Jpn. J. Pharmacol. 2001, 87, 97–103.
- Kiviniemi, A.; Gardberg, M.; Ek, P.; Frantzén, J.; Bobacka, J.; Minn, H. Gadolinium retention in gliomas and adjacent normal brain tissue: Association with tumor contrast enhancement and linear/macrocyclic agents. Neuroradiology 2019, 61, 535–544.
- Castillo, M. History and Evolution of Brain Tumor Imaging: Insights through Radiology. Radiology 2014, 273, S111–S125.
- Cha, S. Update on brain tumor imaging: From anatomy to physiology. AJNR Am. J. Neuroradiol. 2006, 27, 475–487.
- Karschnia, P.; Vogelbaum, M.A.; van den Bent, M.; Cahill, D.P.; Bello, L.; Narita, Y.; Berger, M.S.; Weller, M.; Tonn, J.-C. Evidence-based recommendations on categories for extent of resection in diffuse glioma. Eur. J. Cancer 2021, 149, 23–33.
- Hirono, S.; Ozaki, K.; Kobayashi, M.; Hara, A.; Yamaki, T.; Matsutani, T.; Iwadate, Y. Oncological and functional outcomes of supratotal resection of IDH1 wild-type glioblastoma based on 11C-methionine PET: A retrospective, single-center study. Sci. Rep. 2021, 11, 14554.
- Goryaynov, S.A.; Widhalm, G.; Goldberg, M.F.; Chelushkin, D.; Spallone, A.; Chernyshov, K.A.; Ryzhova, M.; Pavlova, G.; Revischin, A.; Shishkina, L.; et al. The Role of 5-ALA in Low-Grade Gliomas and the Influence of Antiepileptic Drugs on Intraoperative Fluorescence. Front. Oncol. 2019, 9, 423.
- Center for Drug Evaluation and Research. FDA Evaluating the Risk of Brain Deposits with Repeated Use of Gadolinium-Based Contrast Agents for Magnetic Resonance Imaging (MRI); Center for Drug Evaluation and Research: Beltsville, MD, USA, 2017.
- EMA. EMA’s Final Opinion Confirms Restrictions on Use of Linear Gadolinium Agents in Body Scans; EMA: Amsterdam, The Netherlands, 2017.
- Grabrucker, A.M.; Chhabra, R.; Belletti, D.; Forni, F.; Vandelli, M.A.; Ruozi, B.; Tosi, G. Nanoparticles as Blood–Brain Barrier Permeable CNS Targeted Drug Delivery Systems; Springer: Berlin, Germany, 2013; Volume 10.
- Zhang, T.T.; Li, W.; Meng, G.; Wang, P.; Liao, W. Strategies for transporting nanoparticles across the blood-brain barrier. Biomater. Sci. 2016, 4, 219–229.
- Patel, T.; Zhou, J.; Piepmeier, J.M.; Saltzman, W.M. Polymeric nanoparticles for drug delivery to the central nervous system. Adv. Drug Deliv. Rev. 2012, 64, 701–705.
- Zhou, Y.; Peng, Z.; Seven, E.S.; Leblanc, R.M. Crossing the blood-brain barrier with nanoparticles. J. Control Release 2018, 270, 290–303.
- Johnsen, K.B.; Burkhart, A.; Melander, F.; Kempen, P.J.; Vejlebo, J.B.; Siupka, P.; Nielsen, M.S.; Andresen, T.L.; Moos, T. Targeting transferrin receptors at the blood-brain barrier improves the uptake of immunoliposomes and subsequent cargo transport into the brain parenchyma. Sci. Rep. 2017, 7, 10396.
- Johnsen, K.B.; Burkhart, A.; Thomsen, L.B.; Andresen, T.L.; Moos, T. Targeting the transferrin receptor for brain drug delivery. Prog. Neurobiol. 2019, 181, 101665.
- Wang, X.; Zhao, Y.; Dong, S.; Lee, R.J.; Yang, D.; Zhang, H.; Teng, L. Cell-Penetrating Peptide and Transferrin Co-Modified Liposomes for Targeted Therapy of Glioma. Molecules 2019, 24, 3540.
- Kulkarni, P.V.; Roney, C.A.; Antich, P.P.; Bonte, F.J.; Raghu, A.V.; Aminabhavi, T.M. Quinoline-n-butylcyanoacrylate-based nanoparticles for brain targeting for the diagnosis of Alzheimer’s disease. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2010, 2, 35–47.
- Posadas, I.; Monteagudo, S.; Ceña, V. Nanoparticles for brain-specific drug and genetic material delivery, imaging and diagnosis. Nanomedicine 2016, 11, 833–849.
- Li, C.; Wallace, S. Polymer-drug conjugates: Recent development in clinical oncology. Adv. Drug Deliv. Rev. 2008, 60, 886–898.
- Liu, C.; Zhao, Z.; Gao, H.; Rostami, I.; You, Q.; Jia, X.; Wang, C.; Zhu, L.; Yang, Y. Enhanced blood-brain-barrier penetrability and tumor-targeting efficiency by peptide-functionalized poly(amidoamine) dendrimer for the therapy of gliomas. Nanotheranostics 2019, 3, 311–330.
- Albertazzi, L.; Gherardini, L.; Brondi, M.; Sulis Sato, S.; Bifone, A.; Pizzorusso, T.; Ratto, G.M.; Bardi, G. In vivo distribution and toxicity of PAMAM dendrimers in the central nervous system depend on their surface chemistry. Mol. Pharm. 2013, 10, 249–260.
- Pendiuk Gonçalves, J.; Fraga da Cruz, A.; Ribeiro de Barros, H.; Santana Borges, B.; Almeida Soares de Medeiros, L.C.; Soares, M.J.; Padovan Dos Santos, M.; Grassi, M.T.; Chandra, A.; Del Mercato, L.L.; et al. Beyond gold nanoparticles cytotoxicity: Potential to impair metastasis hallmarks. Eur. J. Pharm. Biopharm. 2020, 157, 221–232.
- Podsiadlo, P.; Sinani, V.A.; Bahng, J.H.; Kam, N.W.; Lee, J.; Kotov, N.A. Gold nanoparticles enhance the anti-leukemia action of a 6-mercaptopurine chemotherapeutic agent. Langmuir 2008, 24, 568–574.
- Bredlau, A.L.; Dixit, S.; Chen, C.; Broome, A.-M. Nanotechnology Applications for Diffuse Intrinsic Pontine Glioma. Curr. Neuropharmacol. 2017, 15, 104–115.
- Ruan, S.; Yuan, M.; Zhang, L.; Hu, G.; Chen, J.; Cun, X.; Zhang, Q.; Yang, Y.; He, Q.; Gao, H. Tumor microenvironment sensitive doxorubicin delivery and release to glioma using angiopep-2 decorated gold nanoparticles. Biomaterials 2015, 37, 425–435.
- Joh, D.Y.; Sun, L.; Stangl, M.; Al Zaki, A.; Murty, S.; Santoiemma, P.P.; Davis, J.J.; Baumann, B.C.; Alonso-Basanta, M.; Bhang, D.; et al. Selective Targeting of Brain Tumors with Gold Nanoparticle-Induced Radiosensitization. PLoS ONE 2013, 8, e62425.
- Cheng, X.; Murphy, W.; Recek, N.; Yan, D.; Cvelbar, U.; Vesel, A.; Mozetic, M.; Canady, M.D.J.; Keidar, M.; Sherman, J. Synergistic effect of gold nanoparticles and cold plasma on glioblastoma cancer therapy. J. Phys. D Appl. Phys. 2014, 47, 335402.
- Luly, K.M.; Choi, J.; Rui, Y.; Green, J.J.; Jackson, E.M. Safety considerations for nanoparticle gene delivery in pediatric brain tumors. Nanomedicine 2020, 15, 1805–1815.
- Paciotti, G.F.; Myer, L.; Weinreich, D.; Goia, D.; Pavel, N.; McLaughlin, R.E.; Tamarkin, L. Colloidal gold: A novel nanoparticle vector for tumor directed drug delivery. Drug Deliv. 2004, 11, 169–183.
- Huang, X.; Jain, P.K.; El-Sayed, I.H.; El-Sayed, M.A. Plasmonic photothermal therapy (PPTT) using gold nanoparticles. Lasers Med. Sci. 2008, 23, 217–228.
- Ding, Y.; Jiang, Z.; Saha, K.; Kim, C.S.; Kim, S.T.; Landis, R.F.; Rotello, V.M. Gold nanoparticles for nucleic acid delivery. Mol. Ther. 2014, 22, 1075–1083.
- Setua, S.; Ouberai, M.; Piccirillo, S.G.; Watts, C.; Welland, M. Cisplatin-tethered gold nanospheres for multimodal chemo-radiotherapy of glioblastoma. Nanoscale 2014, 6, 10865–10873.
- Cheng, Y.; Meyers, J.D.; Agnes, R.S.; Doane, T.L.; Kenney, M.E.; Broome, A.M.; Burda, C.; Basilion, J.P. Addressing brain tumors with targeted gold nanoparticles: A new gold standard for hydrophobic drug delivery? Small 2011, 7, 2301–2306.
- Jensen, S.A.; Day, E.S.; Ko, C.H.; Hurley, L.A.; Luciano, J.P.; Kouri, F.M.; Merkel, T.J.; Luthi, A.J.; Patel, P.C.; Cutler, J.I.; et al. Spherical nucleic acid nanoparticle conjugates as an RNAi-based therapy for glioblastoma. Sci. Transl. Med. 2013, 5, 209ra152.
- Liu, Z.; Yan, H.; Li, H. Silencing of DNA repair sensitizes pediatric brain tumor cells to γ-irradiation using gold nanoparticles. Environ. Toxicol. Pharm. 2017, 53, 40–45.
- Cheng, Y.; Dai, Q.; Morshed, R.A.; Fan, X.; Wegscheid, M.L.; Wainwright, D.A.; Han, Y.; Zhang, L.; Auffinger, B.; Tobias, A.L.; et al. Blood-brain barrier permeable gold nanoparticles: An efficient delivery platform for enhanced malignant glioma therapy and imaging. Small 2014, 10, 5137–5150.
- Vajrala, G.; Maricar, S.; Thammineni, P.R.; Raya, C.N.; Vidiyala, S.K.; Madigubba, S.; Panigrahi, M.K. The Effect of Gold Nanoparticles on Chemo and Radiotherapy of Brain Tumor Cells. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, e530.
- Mukhtar, M.; Bilal, M.; Rahdar, A.; Barani, M.; Arshad, R.; Behl, T.; Brisc, C.; Banica, F.; Bungau, S. Nanomaterials for Diagnosis and Treatment of Brain Cancer: Recent Updates. Chemosensors 2020, 8, 117.
- Cortese, B.; D’Amone, S.; Testini, M.; Ratano, P.; Palamà, I.E. Hybrid Clustered Nanoparticles for Chemo-Antibacterial Combinatorial Cancer Therapy. Cancers 2019, 11, 1338.
- Panzarini, E.; Mariano, S.; Carata, E.; Mura, F.; Rossi, M.; Dini, L. Intracellular Transport of Silver and Gold Nanoparticles and Biological Responses: An Update. Int. J. Mol. Sci. 2018, 19, 1305.
- Salazar-García, S.; García Rodrigo, J.F.; Martínez-Castañon, G.-A.; Ruiz-Rodríguez, V.; Portales-Pérez, D.; González, C. Silver nanoparticles (AgNPs) and zinc chloride (ZnCl2) exposure order determines the toxicity in C6 rat glioma cells. J. Nanoparticle Res. 2020, 22, 253.
- Norouzi, M.; Yathindranath, V.; Thliveris, J.A.; Kopec, B.M.; Siahaan, T.J.; Miller, D.W. Doxorubicin-loaded iron oxide nanoparticles for glioblastoma therapy: A combinational approach for enhanced delivery of nanoparticles. Sci. Rep. 2020, 10, 11292.
- Kievit, F.M.; Stephen, Z.R.; Wang, K.; Dayringer, C.J.; Sham, J.G.; Ellenbogen, R.G.; Silber, J.R.; Zhang, M. Nanoparticle mediated silencing of DNA repair sensitizes pediatric brain tumor cells to γ-irradiation. Mol. Oncol 2015, 9, 1071–1080.
- Duong, C.; Yoshida, S.; Chen, C.; Barisone, G.; Diaz, E.; Li, Y.; Beckett, L.; Chung, J.; Antony, R.; Nolta, J.; et al. Novel targeted therapy for neuroblastoma: Silencing the MXD3 gene using siRNA. Pediatr Res. 2017, 82, 527–535.
- Anselmo, A.C.; Mitragotri, S. A Review of Clinical Translation of Inorganic Nanoparticles. Aaps. J. 2015, 17, 1041–1054.
- Hadjipanayis, C.G.; Machaidze, R.; Kaluzova, M.; Wang, L.; Schuette, A.J.; Chen, H.; Wu, X.; Mao, H. EGFRvIII antibody-conjugated iron oxide nanoparticles for magnetic resonance imaging-guided convection-enhanced delivery and targeted therapy of glioblastoma. Cancer Res. 2010, 70, 6303–6312.
- Orringer, D.A.; Koo, Y.E.; Chen, T.; Kopelman, R.; Sagher, O.; Philbert, M.A. Small solutions for big problems: The application of nanoparticles to brain tumor diagnosis and therapy. Clin. Pharm. 2009, 85, 531–534.
- Lee, N.; Yoo, D.; Ling, D.; Cho, M.H.; Hyeon, T.; Cheon, J. Iron Oxide Based Nanoparticles for Multimodal Imaging and Magnetoresponsive Therapy. Chem. Rev. 2015, 115, 10637–10689.
- Reddy, G.R.; Bhojani, M.S.; McConville, P.; Moody, J.; Moffat, B.A.; Hall, D.E.; Kim, G.; Koo, Y.E.; Woolliscroft, M.J.; Sugai, J.V.; et al. Vascular targeted nanoparticles for imaging and treatment of brain tumors. Clin. Cancer Res. 2006, 12, 6677–6686.
- Jiang, J.; Pi, J.; Cai, J. The Advancing of Zinc Oxide Nanoparticles for Biomedical Applications. Bioinorg. Chem. Appl. 2018, 2018, 1062562.
- Palamà, I.E.; D’Amone, S.; Arcadio, V.; Biasiucci, M.; Mezzi, A.; Cortese, B. Cell mechanotactic and cytotoxic response to zinc oxide nanorods depends on substrate stiffness. Toxicol. Res. 2016, 5, 1699–1710.
- Wahab, R.; Kaushik, N.K.; Verma, A.K.; Mishra, A.; Hwang, I.H.; Yang, Y.B.; Shin, H.S.; Kim, Y.S. Fabrication and growth mechanism of ZnO nanostructures and their cytotoxic effect on human brain tumor U87, cervical cancer HeLa, and normal HEK cells. J. Biol. Inorg. Chem. 2011, 16, 431–442.
- Kemper, E.M.; Boogerd, W.; Thuis, I.; Beijnen, J.H.; van Tellingen, O. Modulation of the blood-brain barrier in oncology: Therapeutic opportunities for the treatment of brain tumours? Cancer Treat. Rev. 2004, 30, 415–423.
- Brasnjevic, I.; Steinbusch, H.W.; Schmitz, C.; Martinez-Martinez, P. Delivery of peptide and protein drugs over the blood-brain barrier. Prog. Neurobiol. 2009, 87, 212–251.
- Juillerat-Jeanneret, L. The targeted delivery of cancer drugs across the blood–brain barrier: Chemical modifications of drugs or drug-nanoparticles? Drug Discov. Today 2008, 13, 1099–1106.
- Smith, M.W.; Gumbleton, M. Endocytosis at the blood-brain barrier: From basic understanding to drug delivery strategies. J. Drug Target. 2006, 14, 191–214.
- Bae, Y.H.; Park, K. Targeted drug delivery to tumors: Myths, reality and possibility. J. Control. Release Off. J. Control. Release Soc. 2011, 153, 198–205.
- Infante, P.; Malfanti, A.; Quaglio, D.; Balducci, S.; De Martin, S.; Bufalieri, F.; Mastrotto, F.; Basili, I.; Garofalo, M.; Lospinoso Severini, L.; et al. Glabrescione B delivery by self-assembling micelles efficiently inhibits tumor growth in preclinical models of Hedgehog-dependent medulloblastoma. Cancer Lett 2021, 499, 220–231.
- Bell, J.B.; Rink, J.S.; Eckerdt, F.; Clymer, J.; Goldman, S.; Thaxton, C.S.; Platanias, L.C. HDL nanoparticles targeting sonic hedgehog subtype medulloblastoma. Sci. Rep. 2018, 8, 1211.
- Kim, J.; Dey, A.; Malhotra, A.; Liu, J.; Ahn, S.I.; Sei, Y.J.; Kenney, A.M.; MacDonald, T.J.; Kim, Y. Engineered biomimetic nanoparticle for dual targeting of the cancer stem-like cell population in sonic hedgehog medulloblastoma. Proc. Natl. Acad. Sci. USA 2020, 117, 24205–24212.
- Rodríguez-Nogales, C.; Noguera, R.; Couvreur, P.; Blanco-Prieto, M.J. Therapeutic Opportunities in Neuroblastoma Using Nanotechnology. J. Pharm. Exp. 2019, 370, 625–635.
- Fenton, O.S.; Olafson, K.N.; Pillai, P.S.; Mitchell, M.J.; Langer, R. Advances in Biomaterials for Drug Delivery. Adv. Mater. 2018, 30, 1705328.
- Huang, J.Y.; Lu, Y.M.; Wang, H.; Liu, J.; Liao, M.H.; Hong, L.J.; Tao, R.R.; Ahmed, M.M.; Liu, P.; Liu, S.S.; et al. The effect of lipid nanoparticle PEGylation on neuroinflammatory response in mouse brain. Biomaterials 2013, 34, 7960–7970.
- Buck, J.; Grossen, P.; Cullis, P.R.; Huwyler, J.; Witzigmann, D. Lipid-Based DNA Therapeutics: Hallmarks of Non-Viral Gene Delivery. ACS Nano 2019, 13, 3754–3782.
- da Cruz, M.T.; Simões, S.; de Lima, M.C. Improving lipoplex-mediated gene transfer into C6 glioma cells and primary neurons. Exp. Neurol. 2004, 187, 65–75.
- Yang, J.; Lee, T.-I.; Lee, J.; Lim, E.-K.; Hyung, W.; Lee, C.-H.; Song, Y.J.; Suh, J.-S.; Yoon, H.-G.; Huh, Y.-M.; et al. Synthesis of Ultrasensitive Magnetic Resonance Contrast Agents for Cancer Imaging Using PEG-Fatty Acid. Chem. Mater. 2007, 19, 3870–3876.
This entry is offline, you can click here to edit this entry!