Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Oncology
Pancreatic acinar cell carcinoma (PACC) is a distinct type of pancreatic cancer with low prevalence. We aimed to analyze prognostic factors and survival outcome for PACC in comparison to pancreatic ductal adenocarcinoma (PDAC), based on data from the German Cancer Registry Group.
- pancreatic acinar cell carcinoma
- pancreatic cancer
- German Cancer Registry Group
1. Introduction
Pancreatic acinar cell carcinoma (PACC) is a distinct type of exocrine pancreatic cancer that arises from the acinic cells. It presents microscopically as a solid, cellular neoplasm with minimal stroma [1], (Figure 1). The prevalence of PACC has been estimated to be below 1% of all pancreatic malignancies [2]. Compared to patients with the most common pancreatic cancer, pancreatic ductal adenocarcinoma (PDAC), patients with PACC are on average younger and have a better overall prognosis [2][3]. Clinical evidence on PACC is based on case reports and small institutional series as well as a few registry-based studies that analyzed larger cohorts of patients with PACC [2][3][4][5][6][7]. Many of these studies point out surgical resection as the most effective therapeutic strategy [2][3][4][5][7]. The survival benefit of systemic therapy is more controversial [3][8][9].
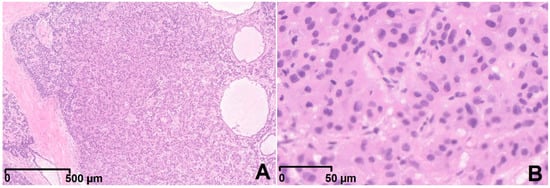
Figure 1. Overview of an acinar cell carcinoma with typical high cellularity and scant fibrous stroma (A, 2.5-fold magnification). In higher magnification (B, 20-fold magnification), tumor cells are presenting a granular eosinophilic cytoplasm and uniform nuclei (hematoxylin and eosin staining).
Because of the low prevalence of PACC, clinical practices well studied in PDAC are often applied also to PACC. However, PACC has distinct clinical, histologic, and molecular features that make a differential approach necessary [1][2][4][10]. Especially relevant are the questions of long-term survival after resection of locally advanced tumors, resection of synchronous or metachronous distant metastases, as well as the benefit of different perioperative and palliative therapies. To expand our knowledge on a rare malignancy such as PACC, registry-based studies are the most feasible.
2. Basic Characteristics of the PACC Cohort
There were 233 (0.44%) patients with PACC out of 52,518 patients with pancreatic malignancy in the whole dataset. The median age at time of diagnosis was 66 years. There were 154 (66.1%) male and 79 (33.9%) female patients. Distant metastases were present in 79 (33.9%) patients. Resection was performed in 131 (56.2%) cases. Of those resected, 80 (61%) received operation alone, 49 (37.4%) operation and adjuvant therapy (47 chemotherapy, 2 radiochemotherapy), 2 (1.5%) neoadjuvant chemotherapy and operation (one of them received neoadjuvant and adjuvant chemotherapy). Distant metastases M1 were present in 18 (13.7%), and lymph node metastases N1 in 56 (42.7%) of resected patients.
3. Survival Analysis of PACC Patients
Survival data were available for 218 (93.6%) patients. Of those, 157 (72%) were dead at last follow-up. Median follow-up was 92 (56 to 158) months. Median overall survival was 22 (15 to 27) months (Figure 2A), 5-year overall survival rate was 21.5% (16.1 to 28.8%). Median survival of resected patients was 34 (27 to 45) months, 5-year survival rate 33.1% (24.8 to 44.3%). Non-resected patients had a median overall survival of 6 (4 to 10) months. (Figure 2E)
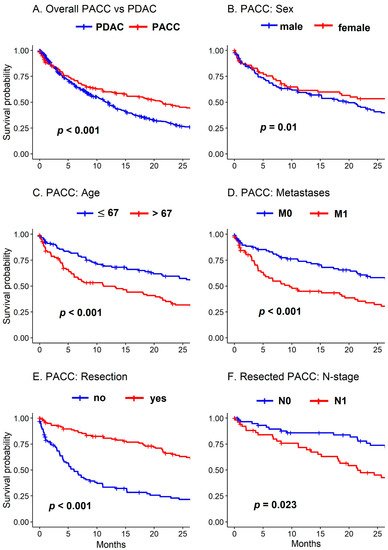
Figure 2. Survival of PACC and matched PDAC cohorts. (A) Overall survival of PACC versus PDAC. (B) Survival of PACC patients according to sex. (C) Survival of PACC patients according to age (67 years or younger versus older than 67 years). (D) Survival of PACC patients according to distant metastases. (E) Survival of PACC patients according to resection versus no resection. (F) Survival of PACC patients according to lymph node metastases.
In the univariable survival analysis, females had better overall prognosis than males (31 versus 20 months, respectively, p = 0.01) (Figure 2B). Age > 67 years (11 versus 29 months, p < 0.001) (Figure 2C) as well as distant metastases (10 versus 28 months, p < 0.001) were negative prognostic factors (Figure 2D).
In the multivariable Cox regression, female sex (hazard ratio (HR) 0.6 (0.43 to 0.87), p = 0.006) and resection were positive prognostic factors (HR 0.34 (0.22 to 0.51), p < 0.001), while age > 67 was a negative prognostic factor (HR 2.1 (1.51 to 2.91), p <
In the subgroup of patients with upfront surgery, lymph node metastases (22 versus 45 months, p = 0.023)nd lymph vessel invasion (21 versus 45 months, p = 0.003) were associated with worse prognosis in the univariable survival analysis.
4. Comparison PACC and PDAC
PACC patients were compared to a cohort of 37,940 patients with PDAC (72.2% of all 52,518 patients). The median age at time of diagnosis of PDAC patients was 70 years compared to 66 years of PACC patients (p < 0.001). The proportion of male patients was higher in the PACC cohort (66.1% versus 53.3%, p < 0.001). More patients were resected in the PACC cohort (56.2% versus 38.9%, p < 0.001). Of those resected, more patients received adjuvant chemotherapy in the PACC cohort (38.2% versus 30.1%, p = 0.045). PACC patients underwent distal pancreatectomy more often than PDAC patients (29 versus 8.2%, respectively, p < 0.001). The estimated overall survival after diagnosis for PACC patients was 22 (15 to 27) months, and for all PDAC patients, this was 8.1 (8.07 to 8.13) months (p < 0.001).
The 218 PACC patients with available survival data were matched to 654 patients with PDAC. The estimated overall survival of the matched PDAC cohort was 12 (10 to 13) months (Figure 2A). Females had better prognosis in PACC (31 versus 20 months, respectively, p = 0.01) compared to males but not in PDAC (13 versus 11 months, respectively, p = 0.163). There were several differences between PACC and the matched PDAC in the subgroup of patients with upfront surgery: there was no statistically significant difference in the estimated survival of resected patients without (M0) and with distant metastases (M1) in PACC (29 versus 32 months, respectively, p = 0.709) but significantly shorter survival for M1 in PDAC (24 versus 9 months, respectively, p < 0.001); no significant difference in resection margin status in PACC R0 versus R+ (34 versus 23 months, respectively, p = 0.208) but significant difference in PDAC (29 versus 12 months, respectively, p < 0.001); no significant difference with adjuvant therapy versus no adjuvant therapy in PACC (36 versus 34 months, respectively, p = 0.48) but survival benefit for PDAC patients with adjuvant therapy (30 versus 16 months, respectively, p < 0.001).
This entry is adapted from the peer-reviewed paper 10.3390/cancers13236121
References
- Thompson, E.D.; Wood, L.D. Pancreatic Neoplasms with Acinar Differentiation: A Review of Pathologic and Molecular Features. Arch. Pathol. Lab. Med. 2020, 144, 808–815.
- Schmidt, C.M.; Matos, J.M.; Bentrem, D.J.; Talamonti, M.S.; Lillemoe, K.D.; Bilimoria, K.Y. Acinar Cell Carcinoma of the Pancreas in the United States: Prognostic Factors and Comparison to Ductal Adenocarcinoma. J. Gastrointest. Surg. 2008, 12, 2078–2086.
- Wisnoski, N.C.; Townsend, C.M.; Nealon, W.H.; Freeman, J.L.; Riall, T.S. 672 Patients with Acinar Cell Carcinoma of the Pancreas: A Population-Based Comparison to Pancreatic Adenocarcinoma. Surgery 2008, 144, 141–148.
- Kruger, S.; Haas, M.; Burger, P.J.; Ormanns, S.; Modest, D.P.; Westphalen, C.B.; Kleespies, A.; Angele, M.K.; Hartwig, W.; Bruns, C.J.; et al. Acinar Cell Carcinoma of the Pancreas: A Rare Disease with Different Diagnostic and Therapeutic Implications than Ductal Adenocarcinoma. J. Cancer Res. Clin. Oncol. 2016, 142, 2585–2591.
- Landa, K.; Freischlag, K.; Nussbaum, D.P.; Youngwirth, L.M.; Blazer, D.G. Underutilization of Surgical Resection in Patients with Pancreatic Acinar Cell Carcinoma. HPB 2019, 21, 687–694.
- Seth, A.K.; Argani, P.; Campbell, K.A.; Cameron, J.L.; Pawlik, T.M.; Schulick, R.D.; Choti, M.A.; Wolfgang, C.L. Acinar Cell Carcinoma of the Pancreas: An Institutional Series of Resected Patients and Review of the Current Literature. J. Gastrointest. Surg. 2008, 12, 1061–1067.
- Wang, Y.; Wang, S.; Zhou, X.; Zhou, H.; Cui, Y.; Li, Q.; Zhang, L. Acinar Cell Carcinoma: A Report of 19 Cases with a Brief Review of the Literature. World J. Surg. Oncol. 2016, 14, 172.
- Patel, D.J.; Lutfi, W.; Sweigert, P.; Eguia, E.; Abood, G.; Knab, L.; Kuo, P.C.; Baker, M.S. Clinically Resectable Acinar Cell Carcinoma of the Pancreas: Is There a Benefit to Adjuvant Systemic Therapy? Am. J. Surg. 2020, 219, 522–526.
- Takahashi, H.; Ikeda, M.; Shiba, S.; Imaoka, H.; Todaka, A.; Shioji, K.; Yane, K.; Kojima, Y.; Kobayashi, S.; Asagi, A.; et al. Multicenter Retrospective Analysis of Chemotherapy for Advanced Pancreatic Acinar Cell Carcinoma: Potential Efficacy of Platinum- and Irinotecan-Containing Regimens. Pancreas 2021, 50, 77–82.
- Jäkel, C.; Bergmann, F.; Toth, R.; Assenov, Y.; van der Duin, D.; Strobel, O.; Hank, T.; Klöppel, G.; Dorrell, C.; Grompe, M.; et al. Genome-Wide Genetic and Epigenetic Analyses of Pancreatic Acinar Cell Carcinomas Reveal Aberrations in Genome Stability. Nat. Commun. 2017, 8, 1323.
This entry is offline, you can click here to edit this entry!