TTS(Takotsubo syndrome) was first officially reported in 1991 as a reversible cardiomyopathy that appeared to be precipitated by acute emotional stress. The majority of TTS patients were postmenopausal females and usually developed symptoms similar to those of an acute coronary syndrome. A strong emotional stressor was thought to cause a transient abnormality of LV wall motion in the apical and mid-ventricular portion without obstructive coronary artery disease with ECG changes . TTS was initially called “Takotsubo cardiomyopathy”. Although most TTS cases were described as having been caused by negative emotions, there are cases in which positive emotions, such as joy, triggered TTS. In addition, 10% of TTS patients are male.
1. Pathophysiology of Takotsubo Syndrome
Sympathetic autonomic nervous system overactivity is one possible pathophysiology underlying TTS. Elevated concentrations of plasma norepinephrine have been reported in acute stroke [
85,
86], and ECG changes in TTS were also observed after an intravenous [
87,
88] or intracoronary [
89] injection of catecholamine. Increased sympathetic nervous system activity is an apparent link in the relationship between cerebrovascular disease and TTS specifically in postmenopausal women.
Recent research has described a pathophysiology linking the relationship between cerebral infarction and TTS with poor outcome, and damage to the integrity of the blood–brain barrier (BBB) was suggested to explain the underlying pathophysiology. In addition to increased levels of catecholamine, post-cerebral infarction patients with TTS showed elevated blood levels of inflammatory mediators that are known to cause vascular conditions such as thromboembolism and stroke [
90]. These stressors concomitant with hypoxia were shown to deteriorate BBB integrity, which could be the mechanism underlying the poor outcomes of Ic-involved stroke, as Ic neurons were also shown to encode and retrieve specific immune responses [
91,
92].
Using an in vitro model of the BBB consisting of an immortalized murine microvascular endothelial cell (cEND) line, Förster et al. (2005) [
93] analyzed the molecular effects of exposure to catecholamines (dopamine, norepinephrine, and epinephrine), pro-inflammation cytokines (interleukin [IL]-6 and tumor necrosis factor-alpha [TNF-α]). They simultaneously subjected the cell system to oxygen glucose deprivation (OGD; which had been established as an in vitro cerebral infarction model) with and without subsequent reoxygenation [
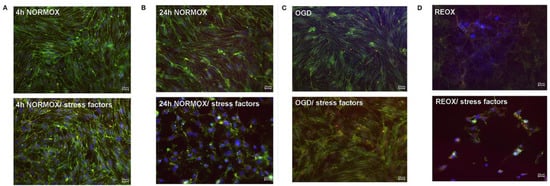
94]. Their results demonstrated that the BBB’s integrity and the cells’ morphology and viability were clearly affected by catecholamine and inflammation under the conditions of OGD. Most proteins of the established BBB model were downregulated (
Figure 5). The structures affected could form the basis of the molecular pathophysiology of the cerebral vasculature and comprise a potential therapeutic target for cerebral infarction concomitant with TTS [
95].
Figure 5. Loss of morphological integrity of cEND cells exposed to elevated catecholamine levels and inflammatory mediators. Immunofluorescence staining of tight junction proteins claudin-5 (green) and ZO-1 (red) as markers of morphological changes of the endothelial cell monolayer. DAPI (blue) was used to stain nuclei. Cells were grown on cover slips to confluence. After differentiation, cEND cells were treated with a combination of catecholamines and inflammatory mediators (stress factors). Stress factors were administered under different incubation conditions. Magnification 400×, scale bar 20 μm. (
A) Stress factor application for 4 h under normoxia conditions (4 h NORMOX). (
B) Stress factor application for 24 h under normoxia conditions (24 h NORMOX). (
C). Stress factor application for 4 h under oxygen glucose deprivation (OGD) conditions. (
D) Stress factor application for 4 h under OGD conditions with 20 h of subsequent reoxygenation under normoxia conditions (REOX). (
E) Cell number in treatments shown in panels (
A–
D) normalized to control. ***
p < 0.001, ****
p < 0.0001. From [
95].
2. Case Report
We reported the TTS case of a 79-year-old female with LV asynergy in the mid-ventricle after a right Ic infarction (
Figure 6). Twelve hours after her hospitalization, the patient suddenly collapsed. After rapid cardiopulmonary resuscitation, spontaneous circulation returned. Coronary angiography was then performed and showed no obstructive arterial disease (
Figure 7). In left ventriculography, akinesis was observed in the mid-portion with hyperkinesis in the basal and apex portions of the LV (
Figure 8). After two weeks of hospitalization, the LV contraction in the mid-portion was improved as shown by cardiac ultrasound. This patient’s right Ic infarction might have been associated with CAN dysregulation that was linked to an increase in sympathetic nervous system activity that triggered TTS [
96].
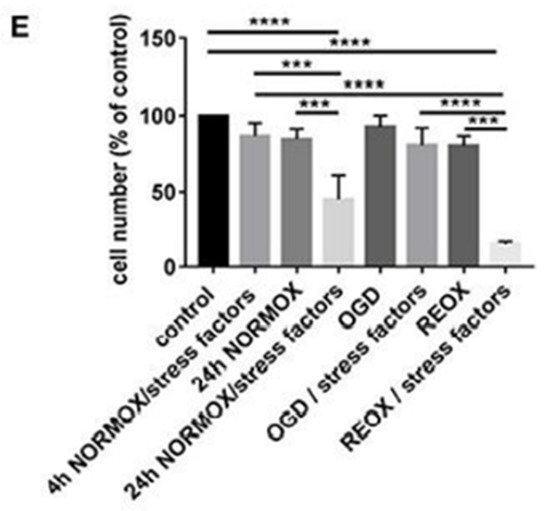
Figure 6. Axial brain MRI in a patient with TTS. Acute cerebral lesions including the right Ic were observed in the diffusion-weighted (
A) and FLAIR (
B) images. From [
96].
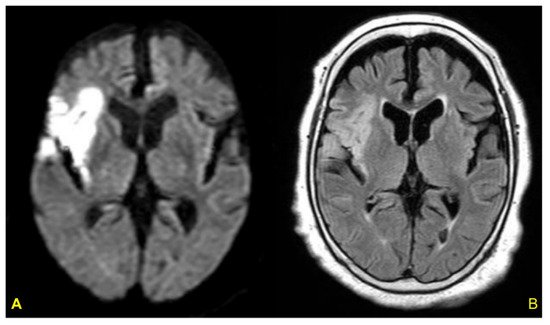
Figure 7. Coronary artery angiography. No stenosis was observed in the right coronary artery (
A), left anterior descending artery, or circumflex artery (
B). From [
96].
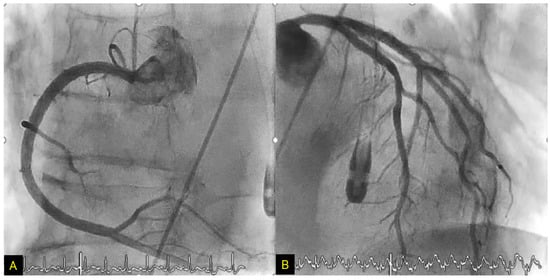
Figure 8. Left ventriculography. End-diastolic-phase left ventriculogram (
A) and end-systolic-phase left ventriculogram (
B). The extensive area around the mid-portion shows akinesis (arrows), and the basal and apex portions display hypercontraction, especially in the end-systolic phase (
B). From [
96].
In a study of 1750 TTS patients, the apical pattern of TTS was shown to be the most common type (81.7%), and the mid-ventricular pattern was the second most common type (14.6%) [
97]. Although Ic lesion is considered to play a pivotal role as a trigger of TTS [
4], a TTS patient with the mid-ventricular pattern had never been reported in relation to Ic damage until our above-described patient [
96].
In the apical pattern of TTS, the effect of increased catecholamine levels on the myocardium determined by the beta-adrenoceptor (βAR) gradient is thought to be associated with subsequent acute apical ballooning [
98]. βAR gradients in the LV might be different between the apical pattern and the mid-ventricular pattern of TTS. The murine cardiac β1AR function was shown to be suppressed by β2AR overexpression [
99]; there was a bell-shaped dose-response relationship between the doses of epinephrine and myocardial contraction, and at the highest epinephrine doses, a negative inotropic effect was confirmed in relation to the β2AR. In our TTS patient’s case, the highest β2AR distribution might have been in the mid-portion of the LV.
3. Ic Stroke and Takotsubo Syndrome
Data from the Japanese National Cardiovascular Center [
100] revealed that among 569 consecutive patients with acute cerebral infarction, seven patients developed TTS. All seven of these patients were female, and six were ≥75 years old. In these six patients, the culprit infarcts included the Ic or were identified close to the Ic. Elderly females with an Ic lesion were thus suggested as predominant features for the development of TTS among patients with acute ischemic stroke [
100]. In a Korean hospital-based registry, the patients with both ischemic stroke and TTS also had a higher inflammatory marker level and a higher prevalence of lesions in the Ic and peri-Ic areas [
101].
In a review of patients with acute stroke concomitant with the development of TTS [
102], the female proportion was 77%, and the average age of the patients was 72.5 years. Stroke involving the Ic was found in 38.4% of the patients. The patients’ mean score on the U.S. National Institutes of Health Stroke Scale (NIHSS) was 12.6 at admission and 10.8 at discharge. ST-segment elevations and T-wave inversions were observed in 69.2% and 84.6% of the cases, respectively, whereas the average TnT was 0.64 mcg/dL. The average LV ejection fraction (LVEF) was 34.4% at the time of onset; LVEF was significantly improved in 84.6% of the patients at approximately four weeks after onset [
102]. In addition, the majority of the patients presented with an apex-involved pattern [
103].
This entry is adapted from the peer-reviewed paper 10.3390/biom12010110