Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Social Issues
Frailty is a complex state of objective and subjective vulnerability. It tends to increase with age, but the process is influenced by previous life course, especially previous disadvantages. Results show that while frailty increases with age, there is also evidence of an accumulation of risks: the longer the periods of adult life affected by unemployment, stress, financial hardship or, most importantly, bad health, the frailer individuals are in their late years. Furthermore, periods of coexisting disadvantages in adulthood translate into additional frailty in late life.
- aging
- life course
- frailty
1. Introduction
Health at older ages is subject to physiological decline [1], but it is also path-dependent: it reflects what happened in youth and adulthood [2]. Life trajectories begin in childhood [3] and evolve through the experiences made, among others, in the process of family formation (and dissolution), at reproduction [4,5], and at work [6,7]. Each stage affects the next and all are subject to several constraints, among which are the economic ones, and when these constraints are particularly binding the consequences on health in old age may be severe [8].
Health tends to deteriorate in later life, but this deterioration is not the same for everybody. It is particularly marked for those whose life trajectory was unfavorable, especially if adversities cumulated or lasted for long periods, or both [9,10]. The notion of accumulation of disadvantages relates to the number, duration, and severity of various types of exposure to risks. While each exposure exerts an independent effect on later life health, multiple exposures, not surprisingly, prove particularly harmful.
Two aspects may be distinguished: persistence and coexistence of disadvantages. The former refers to the length of periods of exposure to a single factor or a series of factors, even if these periods are not consecutive. Examples are spells of financial hardship or poverty [11,12,13], prolonged living in deprived neighborhoods [14], and long-term unemployment [15].
When disadvantages occur together, or coexist, researchers refer to multiple deprivation [9,11,14,15,16]. As biographies are made of interrelated trajectories—e.g., in terms of employment, education, and health—adverse events may reinforce one another [17].
2. Descriptive Results
Figure 1 shows the prevalence of the disadvantages considered in the analysis during the respondents’ adult years. Unemployment is the least frequently reported problem; financial hardship prevails initially, but stress is the main concern after age 30. Health problems affect about 3% of respondents at 25 years, and progressively more, up to 10% by 59 years. Overall, the share of respondents reporting coexisting disadvantages is low, but increases with age, from below 2% to about 5%.
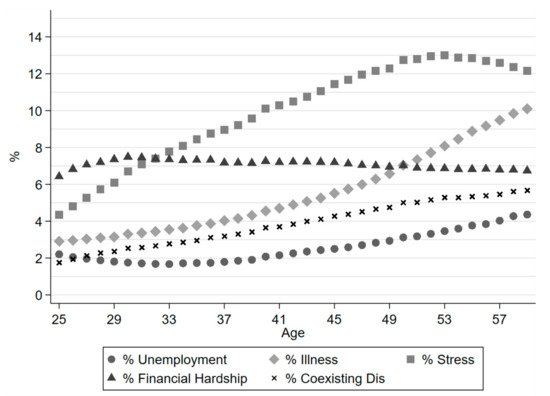
Figure 1. Prevalence of disadvantages, and coexisting disadvantages in adult years (19 SHARE countries, 2004–2017).
3. Lifelong Disadvantage: Persistence
The four panels of Figure 2 show the predicted frailty scores by age for selected levels of each specific disadvantage, under the assumption that no other disadvantage was experienced in adulthood.
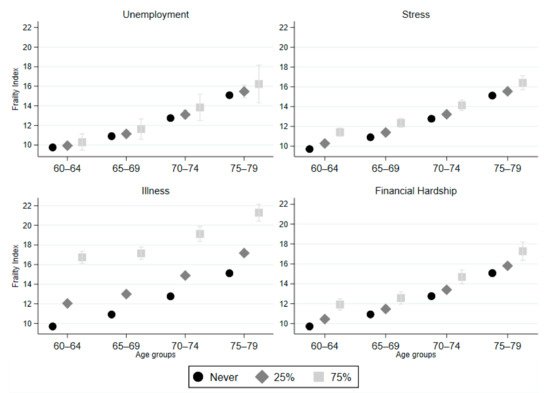
Figure 2. Predicted frailty scores by age, for various levels of past disadvantages, by type of disadvantage (19 SHARE countries, 2004–2017). 95% CI. Other covariates at their average level.
Although frailty increases with age for everybody, those who experienced adverse events in adulthood fare worse than others. As expected, the worst-case emerges in relation to poor past health (illness). As the frailty index itself may not be very telling, especially to those who are not familiar with it, we suggest an alternative point of view: to consider its equivalent in terms of years of life, that is referring to the x axis (age) rather than to the y axis (frailty). This probably gives a better sense of how past disadvantages trigger earlier biological aging and a corresponding increase in vulnerability.
4. A Breakdown by Welfare Regime
While everybody becomes frailer with age, the process is accelerated in Bismarckian, Southern, and Eastern Europe, while it is relatively modest in Scandinavian countries. Although in all groups of countries previous disadvantages exert an analogous frailty-increasing effect, final results differ markedly. Figure 4 suggests what the region-specific models (not reported here, but available upon request) indicate: in Scandinavia, those with very poor conditions in adulthood (e.g., with health problems 75% of the time) have frailty levels that are comparable to those of the healthiest in Eastern Europe—especially past 70 years of age.
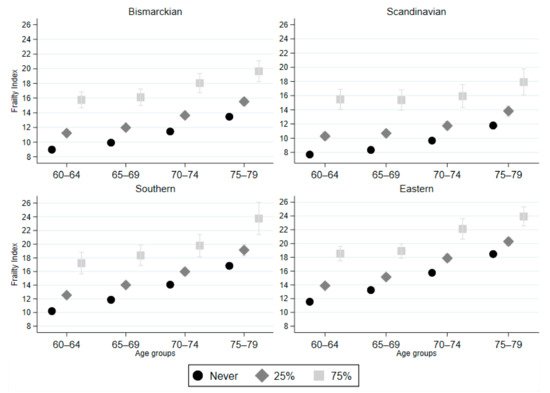
Figure 4. Predicted frailty scores by age, for various levels of past illness (in adult years), by welfare regime (19 SHARE countries, 2004–2017). 95% CI. Other covariates at their average level.
5. Research Findings
In line with previous research and with expectations, frailty, while increasing with age, reflects past experiences of stress and disadvantage. Apart from unemployment, the frailty effects of which are relatively minor, these long-term consequences may be relevant, especially when past episodes were prolonged (persistence) or simultaneous (coexistence). Multiple disadvantages occur rarely, but when they do, the consequences on frailty may be serious. Note that this finding has policy implications: problems, such as poor health and unemployment, for instance, which are typically targeted separately in most welfare systems, should instead be addressed simultaneously, because they tend to be particularly harmful when they occur together or persist in adult life.
Poor health in adulthood (and, additionally, during childhood) is the single disadvantage most closely associated with high frailty in late life, and these effects are strong already at relatively young ages (60–64 years) – a result that stands out more clearly if one transforms the worsening of the frailty index into an “individual aging” index. In short, it is as if affected respondents were N years older than non-affected respondents, despite having lived the same number of years. This aging effect, N, may be strong, frequently between 5 and 10 years, and it remains large throughout the observed age interval (60 to 79 years), although it shows signs of decline (health convergence) at older ages.
6. Conclusions
With population aging, the sustainability of welfare in Western societies has come into question. Both the WHO’s “healthy ageing” action [27] and the European Commission’s “healthy and active ageing” framework [30] underline the need to improve older people’s life and well-being, insisting on the notion of healthy lifestyles and subscribing to a life course approach. In this respect, the WHO encourages a prompt identification of people – especially the elderly – in the community with higher frailty profiles, as a fundamental instrument to make intervention to prevent, or at least delay, functional decline. Early action, the socio-economic background, and life-course experiences have been recognized as important determinants of later life health [2,3,8] and the results in this entry support this view, showing that frailty has life-course determinants: persistent and cumulative disadvantages during youth and adulthood tend to have long-lasting effects, clearly detectable already at relatively young ages (e.g., at 60–64 years). The early identification of frailty is crucial, as it can be stopped, and even reverted, with adequate prognosis and care [21].
This entry is adapted from the peer-reviewed paper 10.3390/jal2010002
This entry is offline, you can click here to edit this entry!