Obstetric and newborn outcomes of assisted reproductive technology (ART) pregnancies are associated with significative prevalence of maternal and neonatal adverse health conditions, such as cardiovascular and metabolic diseases. These data are interpreted as anomalies in placentation involving a dysregulation of several molecular factors and pathways. It is not clear which extent of the observed placental alterations are the result of ART and which originate from infertility itself. These two aspects probably act synergically for the final obstetric risk. Data show that mechanisms of inappropriate trophoblast invasion and consequent altered vascular remodeling sustain several clinical conditions, leading to obstetric and perinatal risks often found in ART pregnancies, such as preeclampsia, fetal growth restriction and placenta previa or accreta.
1. Introduction
There is a rapidly increasing interest in placentation in obstetric adverse outcome, neonatal and adult life health after infertility, and its related therapies. Abnormal placentation is a common finding in the infertile population, even among those couples conceiving spontaneously after a period of infertility. A higher risk of preterm birth (PTB) and low birth weight (LBW) has been found in these pregnancies [
1]. Moreover, abnormal placentation and obstetric complications such as PTB, preeclampsia (PE), and fetal growth restriction (FGR) have been associated with endometriosis, a common factor of infertility [
2]. Another maternal condition at risk for the development of placental anomalies, commonly associated with infertility, is polycystic ovary syndrome (PCOS), in which the prevalence of gestational diabetes mellitus (GDM) is significantly increased [
3]. Of note, GDM is an independent risk factor for the onset of placental disorders with altered structure, function and hypertrophic growth of the organ [
4].
ART is a group of in vitro techniques used to treat moderate and severe infertility, including in vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), frozen embryo transfer (FET), oocyte donation (OD), blastocyst culture, intrauterine insemination, and preimplantation genetic testing for aneuploidy (PGT-A). Unfortunately, each of these techniques may represent a possible confounding factor to the identification of a precise relationship between ART procedures and obstetric or neonatal outcomes, including children and their adulthood health. Many studies report an evident increase of obstetrical risk and perinatal complications with ART, especially for hypertensive disorders of pregnancy (HDP), from gestational hypertension to eclampsia [
6,
7,
8,
9,
10,
11,
12,
13].
The role of the placenta in these conditions has been demonstrated in several studies. It is well documented that ART can be associated with changes in placental morphology and structure, growth dynamics, imprinted and non-imprinted genes, and other aspects regulating placentation [
15].
2. Abnormal Placentation and ART: Molecular Factors and Involved Signaling
Abnormal placentation may present in a variety of phenotypes, severity, clinical conditions and consequences as the result of several types of infertility treatments and techniques used in ART. For these reasons, it becomes difficult to linearly relate placental influence to obstetrical and perinatal (or neonatal) outcomes after ART.
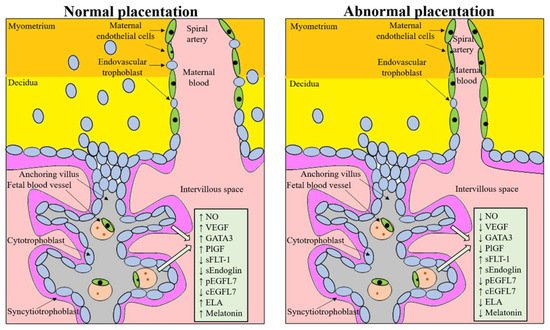
An altered expression of factors and molecules involved in proper placental development, leading to impaired trophoblast invasion and subsequent reduced vascular remodeling and placenta hypoperfusion, sustain several clinical conditions leading to obstetric and perinatal risks often found in ART pregnancies, such as PE, FGR and placenta previa or accrete (
Figure 1) [
24,
25,
26,
27,
28]. Syncytiotrophoblast stress has been associated with a dysregulated expression of placental growth factor (PlGF) and soluble fms-like tyrosine kinase 1 (sFLT-1) [
29,
30]. Circulating levels of the anti-angiogenic factor sFLT-1 are increased, and those of PlGF are decreased even before the onset of the clinical symptoms of PE and FGR [
31,
32,
33,
34,
35]. The increased ratio sFLT-1:PlGF is thought to contribute to the systemic endothelial response and correlate with the severity of FGR and PE.
Figure 1. Molecules regulating proper placental development, whose dysregulation is involved in an abnormal placental development. NO, nitric oxide; VEGF, vascular endothelial growth factor; GATA3, GATA binding protein 3; PlGF, placental growth factor; sFLT-1, soluble fms-like tyrosine kinase 1; sEndoglin, soluble endoglin; pEGFL7, placental epidermal growth factor-like domain 7; cEGFL7, circulating epidermal growth factor-like domain 7; ELA, elabela.
Over the last decades, several other factors have been demonstrated to be altered in pregnancy disorders associated with abnormal placentation (e.g., soluble endoglin (sEndoglin), PlGF and epidermal growth factor-like domain 7 (EGFL7)), with the aim to create a panel of markers to allow an earlier and more precise diagnosis of PE. sEndoglin has been shown to be upregulated in abnormal placenta, typical of FGR and PE, and released into the maternal blood, where it acts as antiangiogenic factor by inhibiting transforming growth factor-beta (TGF-β) signaling in the vasculature. sEndoglin markedly increased, beginning 2 to 3 months before clinical manifestations of PE [
38,
39]. EGFL7, originally discovered as a largely endothelial restricted gene, has been recently demonstrated to be expressed in the placenta and involved in placental angiogenesis and trophoblast migration [
40,
41,
42]. Altered EGFL7 expression is associated with abnormal placentation and systemic maternal endothelial dysfunction, observed in PE [
40,
43,
44]. Maternal treatment with nitric oxide (NO) donors increases placental EGFL7 levels and improves maternal hemodynamic state and perinatal outcome [
45,
46]. In the maternal circulation, endothelial dysfunction and abnormal hemodynamic state are associated with increased levels of EGFL7, which return to control levels after NO treatment [
44]. Moreover, EGFL7 dosage in maternal circulation allows to discriminate between PE and FGR [
43]. Although there are no data correlating EGFL7 with ART, dosage of its circulating levels could help identify ART-associated abnormal placentation.
In FGR and placental insufficiency, the levels of the hormone melatonin are significantly reduced, and this decrease is correlated with proinflammatory activities of tumor necrosis factor alpha (TNF-α), interleukine-1beta (IL-1β), and IL-6 [
47]. Melatonin is an antioxidant factor and an anti-inflammatory agent [
48,
49]. Several studies support the production of this hormone in the ovary as a whole [
50,
51], the granulosa cells, including those making up the cumulus oophorus [
52,
53], and the oocyte [
54]. In women undergoing ART, melatonin significantly increased the implantation rate [
55]; a similar result was obtained in women affected by PCOS undergoing intrauterine insemination [
56]. Melatonin crosses the cell membrane, thus interacting with intracellular molecules via different signaling pathways and displaying scavenger functions [
57]. Melatonin upregulates the primary implantation receptors, ErbB1 and ErbB4, and significantly reduces intracellular ROS in mouse blastocysts (increasing the embryo total antioxidant capacity) and promotes mitosis of the inner cell mass and trophectoderm cells [
58]. Recently, it has been demonstrated that the supplementation of culture medium with melatonin (10
−9 mol/L) improves the growth of mouse parthenogenetic embryo potentially by promoting cell cycle progression [
59]. Despite all these functions, melatonin is not present in culture media used in ART. We could speculate that the addition of melatonin to the ART media may be beneficial.
3. Pathophysiology of the Placenta in Pregnancy Complications and ART Pregnancies
3.1. Altered Hormonal Milieu Effect on Placental Development
Several common infertility conditions, such as endometriosis and PCOS, often treated with ART, are characterized by a hormonal dysregulation that affects proper placentation. In endometriosis, a defective deep placentation may derive from functional abnormalities of the eutopic endometrium, as well as an imbalance in endocrine and inflammatory markers [72]. PTB, placenta previa, placental abruption, gestational hypertension, PE, LBW, SGA, cesarean delivery, postpartum hemorrhage, and stillbirth have been significantly associated with endometriosis in a systematic review and meta-analyses, including in 39 studies [73]. PCOS is another condition leading to infertility, in which the defective trophoblast invasion and placentation may be caused by mother’s hyperandrogenism [74,75]. Testosterone can act directly on trophoblast invasion, with modifications of placenta morphology and function [76,77]. PCOS is a chronic low-grade inflammation associated with metabolic dysfunction that is enhanced in pregnancy by the induction of an endothelial dysfunction [78]. This condition might in turn prevent normal remodeling of spiral vessels and the physiologic decrease of uterine artery impedance, thus reducing the depth of endovascular trophoblast invasion. As a consequence of these patterns, in patients with PCOS the placental weight, thickness, density and volume was found significantly reduced [76].
3.2. Epigenetic Changes after ART Techniques Are Associated with Altered Gene Expression in the Placenta and Congenital Imprinting Disorders
Epigenetic regulatory mechanisms can originate from several sources: direct DNA methylation, non-coding RNA, imprinting, and post-translational modification of histone proteins and chromatin remodeling [
80]. According to some clinical studies, it was speculated that prolonged exposure to extracorporeal environment might predispose human embryos to disorders of genomic imprinting and to epigenetic modification [
81]. Each stage of embryo development, from fertilization to blastocyst formation, also in humans, can undergo to epigenetic changes and consequent differential gene expression in the placenta [
82,
83]. In the pre-implantation period, the embryonic epigenome is entirely reprogrammed by specific methylations [
84], leading to an increase in the risk of gene expression alterations under specific circumstances. For example, there is evidence that aberrant fetal DNA methylation might cause abnormal development of the placenta and recurrent spontaneous abortion [
85].
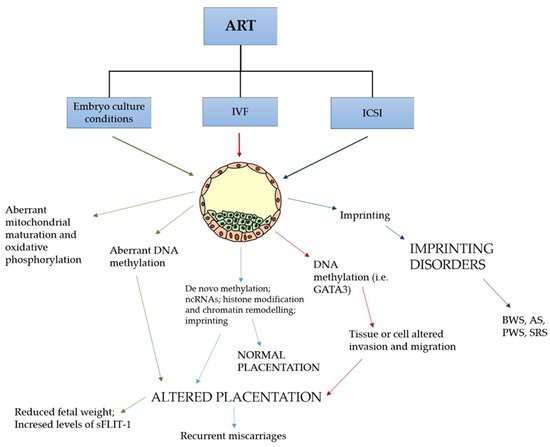
We must consider that ART procedures occur simultaneously to this extensive epigenetic reprogramming and we cannot rule out that the stress involved in ART might affect the establishment and/or maintenance of genomic imprinting (
Figure 2). Actually, more than 100 imprinted genes have been found to be strictly involved in the growth and development of embryos [
15]. In placentas from IVF pregnancies, a different methylation pattern was observed in comparison to non-IVF gestations and environmental conditions were considered responsible for these findings (
Figure 2) [
82,
83]. IVF disturbs the DNA methylation of the imprinting control region of
H19/Igf2,
Snrpn,
Peg3, and
Kcnq1ot1 genes, inducing morphological alterations in the placenta and an increased risk of adult metabolic syndrome [
86]. Studies using animal models have demonstrated a dysregulation of several maternally and paternally expressed imprinted genes (e.g.,
Kcnq1ot1 involved in placental growth,
Peg10 that is required for the differentiation of placental spongiotrophoblast and labyrinth,
Peg11/Rtl1 involved the development of placental labyrinth and nutrient passive transport,
Sfmbt2 playing a key role in the maintenance of trophoblast cell types) in the IVF group as compared to the control group [
87,
88,
89]. Most of these genes play an important role in the proper placental morphology and function. Moreover, specific transcription factors, such as GATA binding protein 3 (GATA3), produced by trophectoderm at blastocyst stage, may be responsible for tissue or cell altered invasion and migration under the influence of the local environment [
90].
Figure 2. ART techniques affecting epigenetics in the pre-implantation embryo. Epigenetic dysregulation is involved in an abnormal placentation and genetic imprinting disorders. sFLT-1 denotes soluble fms-like tyrosine kinase 1, GATA3 GATA binding protein 3, BWS Beckwith–Wiedemann syndrome, AS Angelman syndrome, PWS Prader–Willi syndrome, SRS Silver–Russell syndrome.
3.3. Immune Dysregulation at the Maternal-Fetal Interface
Increased immune activity at the maternal–fetal interface and significant histological and immunohistochemical differences were observed in placentas from pregnancies obtained by IVF of heterologous oocytes, compared to those obtained using homologous oocytes [
112], and may be the consequence of a host versus graft rejection-like condition. This aspect was further investigated using 3D ultrasound analysis. This technique demonstrated a more marked reduction of first-trimester placental volume in pregnancies obtained using donor oocytes [
113].
3.4. Mechanical Stress on Embryo and Placental Development (the Case of PGT-A)
PGT-A is an ART technique that is increasingly performed, considering that it represents 40% of all IVF cycles in the USA [115]. Its aim is to discover if produced embryos are aneuploid and, in this case, they should not be transferred into the uterus, in order to prevent implantation failure and miscarriages. PGT-A preliminarily requires the in vitro development of embryos up to the blastocyst stage, in order to collect 5 to 10 trophoblast cells. Embryos are then frozen while waiting for the genetic analysis results. Embryos with no or few aneuploidies are thawed and transferred (FET) in the uterine cavity after endometrial hormonal preparation using estrogen and progesterone. In this condition, natural ovulation and formation of the corpus luteum are suppressed. Similar to PGT-A, preimplantation genetic test for monogenic diseases (PGT-M) allows to screen for embryos affected by monogenic diseases.
4. Metabolic and Cardiovascular Consequences of Placental Dysregulation in Mothers Following ART
Studies demonstrated that vascular dysfunctions in IVF pregnancies were similar to those identified when babies were conceived naturally from mothers affected by PE [
132,
133]. Sundheimer and Pisarska explain that the size of the placental bed and successful trophoblast invasion and spiral artery remodeling determine maternal blood flow. With these premises, abnormal placentation associated with infertility can represent a consequent marker of overall health for both the mother and her offspring [
134]. It has been well known for a long time that inadequate trophoblast invasion and poor spiral artery remodeling may cause reduced vascular perfusion in pregnancy [
135].
Women of advanced maternal age are generally at increased risk of GDM, HDP, operative and cesarean deliveries [
136,
137]; however, those who conceive with the use of IVF are at increased risk of retained placenta, suggesting that placentation abnormalities may contribute to maternal morbidity, and this may be more pronounced in women with infertility [
138].
In summary, cardiovascular and metabolic diseases derived from impaired placentation following infertility treatments may have long-term consequences on both the mother and the newborn.
5. Health Risk in Infancy as a Consequence of Placental Dysfunction Following ART
According to the “developmental origins of health and disease theory” [143] and the Barker hypothesis of the developmental origins of chronic adult disease [144], placental dysfunction and abnormal fetal development may have long-term consequences on the neonate and his development, from childhood to adult life. A higher risk of diabetes mellitus and CVD were found in children whose mothers had PE and HDP, by long-term follow up observations [145,146]. A track of this condition is represented by the finding of reduced endothelial function in mothers and children after PE [147].
Additionally, there is increasing evidence that offspring conceived by IVF displays a level of vascular dysfunction similar to that seen in children spontaneously conceived by mothers with PE [132,133]. Of note, in 2015 in a randomized case-control trial, antioxidant administration to IVF children was able to improve NO bioavailability and responsiveness of both systemic and pulmonary circulation [149], thus indicating that vascular dysfunctions induced by ART are reversible in young people.
6. Simultaneous Action of Factors Dysregulating Normal Placentation
Infertility and its treatments, including ART and its various procedures (ICSI, blastocyst culture + FET + PGT-A with ovarian stimulation or hormonal preparation), may individually or synergistically participate in the dysregulation of embryo and placenta development. Consequently, it is probably impossible to separate the relative contribution of the many factors influencing embryo, placental, and newborn health when an infertile woman is treated with the many types of ART techniques. These techniques may represent confounding factors for a full understanding of previous studies and future ones to be designed.
Each technique may lead to important epigenetic changes and differential gene expression in the placenta [
82,
83] or damage the developing embryos with thermal, oxidative and mechanical stressing actions [
82,
98,
158].
Pivotal reproductive hormones, such as human chorionic gonadotropin, progesterone and estradiol, are found at high concentrations at the maternal–fetal interface during vessel remodeling. This observation allows to hypothesize that such relevant vascular transformation may be under the influence of these hormones, which may control trophoblast migration [
90,
159]. A potential role in placental function dysregulation has been proposed for estrogens. In this respect, elevated estrogen exposure (as in controlled ovarian hyperstimulation) has been associated with higher rates of LBW and FGR [
160].
Are perinatal adverse outcomes in infertile patients the consequence of ART or are they the consequence of the underlying infertility? A possible answer to this basic question may come from infertile couples conceiving spontaneously with no ART treatments; in these couples, a higher risk of PTB and LBW has been reported [
1]. However, an increasing number of observations show vascular dysfunctions similar to those observed in PE in IVF offspring [
132,
133], and a common mechanism of action could be postulated.
The induction of defective methylation and consequent alteration of gene expression, which may impair placentation [
85], can be caused by oxidative stress [
161,
162], as in endometriosis and by the altered hormonal milieu, i.e., supraphysiologic estradiol levels due to ovarian hyperstimulation [
97]. Particular negative effects on embryo development may occur in PGT-A procedures, in which the epigenetic risk for long in vitro culture may be added to the trophectoderm mechanical stress. If the patient is also affected by PCOS, this adverse metabolic condition for the placenta would considerably increase the overall obstetric, perinatal and postnatal final risk [
76,
77]. All these factors could exert additive effects, leading to the pathologic condition.
This entry is adapted from the peer-reviewed paper 10.3390/ijms23020659