The prostate is partially enveloped by a capsule, consisting of a layer of smooth muscle bundles mainly arranged in a transverse plane, and collagen fibers, usually concentrated as a thin line at the external border [10,11]. The smooth muscle cells of the internal border of the capsule blend with the prostatic stroma [11]. The thickness of the capsule, the relative proportions of collagen and smooth muscle and the distance of the prostatic acini to the surface of the prostate vary significantly, even within different areas of the same gland [10]. Additionally, the capsule is missing in the anterior and anterolateral surfaces of the gland, even though its outer collagen region is consistently identified in most parts of the gland. [11] Thus, the prostatic capsule cannot be regarded as a well-defined anatomic structure, and the terms extracapsular extension, invasion of the capsule and capsule penetration are no longer accepted in prostatectomy reports, being replaced by the term extraprostatic extension [12,13].
To ensure precise assessment of the margins, at the Pathology Department, the whole surface of the prostate is inked with one or multiple colors depending on the pathologist preference and the department’s protocol (Figure 1a) [14]. Special considerations should be given to the grossing of the apex and the base. To reduce overestimation of positive margins, the cone method or a parallel/parasagittal sectioning is preferred for both anatomical areas over the trimming of a save block (Figure 1b) [14].
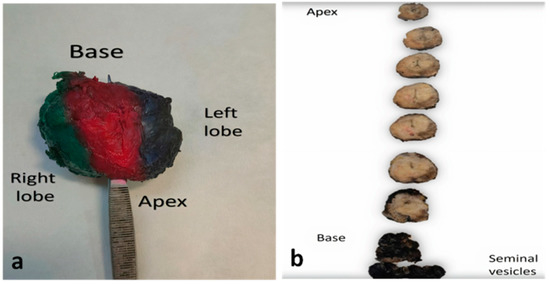
Figure 1. Gross handling of prostatectomy specimens (a) Prostate specimen, colored with different colors in each surface to help orientation. (b) Serial sectioning through the transverse axis from apex to base (margins colored with blank ink). Apex and base will be subsequently sectioned in a parallel (parasagittal) way (not shown).
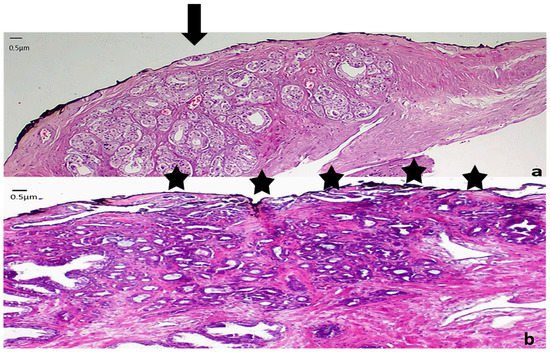
A positive margin of resection (MOR) is defined as malignant glands in contact with the ink (Figure 2) [14], which means that the neoplasm extends to the area where the surgeon has dissected the tissue [15]. The presence of neoplastic cells close but not in contact with the surface of the prostate is not considered as a positive margin (Figure 2) no matter how close the cells are to the ink [16], as studies have shown that this has no prognostic significance [17,18].
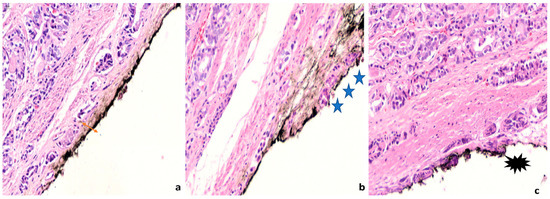
Figure 2. Definition of margin positivity (a) Neoplastic cells are close but not in contact with the ink. The distance between the inked margin and the neoplastic cells is pointed with a double-sided arrow. (b) Neoplastic cells are in contact with the ink. This is considered a positive margin. Three asterisks indicate the area of margin infiltration. (c) Cautery artifact in neoplastic cells in contact with the ink. An asterisk highlights the area of cautery effect. (400× magnification).
Practical issues regarding what is considered a positive margin are common. In the anterior surface of the prostate, the gland is surrounded by a fibromuscular stroma and its capsule is incomplete, thus, there is increased difficulty in recognizing the presence of extraprostatic extension and positive MOR [19]. In addition, cautery artifacts are frequent at the MORs (Figure 2) and may rarely pose difficulty in determining the nature of the cells that are present at the ink.