The identification of homogeneous subgroups of patients with chronic low back pain (CLBP), based on distinct patterns of motor control, could support the tailoring of therapy and improve the effectiveness of rehabilitation. Differences in the patterns of motor control can be identified using outcome measures based on muscle activation or kinematic movement patterns, representing the outcomes of neural structures and processes. The purpose of this review was (1) to assess if there are differences in motor variability between patients with CLBP and pain-free controls, as well as inter-individually among patients with CLBP, during the performance of functional tasks; and (2) to examine the relationship between motor variability and CLBP across time.
1. Introduction
Chronic low back pain (CLBP) is a highly disabling condition, which calls for effective interventions that target pain, disability, and functioning [
1,
2,
3]. Although improvements for guidelines of CLBP clinical practice have been achieved over the years [
4], the effectiveness of therapies, including rehabilitation, remains modest at best [
5,
6]. Variations in treatment outcomes could be driven by the heterogeneity of the CLBP population [
7,
8,
9,
10,
11]. In CLBP, central and peripheral nociceptive processes are influenced by multidimensional factors [
12,
13,
14]. The identification of homogeneous subgroups of patients with CLBP, based on distinct patterns of motor control, could support the tailoring of therapy and improve the effectiveness of rehabilitation [
15,
16].
Differences in the patterns of motor control can be identified using outcome measures based on muscle activation or kinematic movement patterns, representing the outcomes of neural structures and processes [
17]. Studies have shown aberrant alterations in trunk-pelvis coordination and in muscle recruitment during functional tasks in patients with CLBP compared to pain-free controls, such as during walking [
18]. While there is a long tradition of studying movements based on mean values and ensemble averages of movement patterns in CLBP over the last decades, the concept of motor variability has received considerable attention in recent years [
19,
20,
21]. From a motor-control perspective, features of motor variability provide insight into stable and adaptive motor control [
22,
23,
24]. One of the origins of motor variability is ‘motor redundancy’, defined as having more degrees of freedom (DOFs) than necessary to execute a motor task [
25]. Therefore, each repetition of a movement is based on variations in neural and motor patterns, while leading to the same goal. Hence, movement variability is inherent across multiple executions of the same task, in kinematic, kinetic, and muscle activation patterns, and can therefore be regarded as a natural phenomenon.
The interpretation of systematic differences in motor variability is challenging because it is unknown whether these reflect the adaptability of the neuromotor system and should therefore be considered beneficial, or reflect changes in physiology as a result of pathological processes [
26]. For instance, trunk stiffness reduces movement variability and could lead to increased spinal loading while moving [
27] but could also reflect an attempt to stabilize the spine [
21]. High movement variability could be a sign of reduced neuromuscular control but might be beneficial for the re-distribution of joint loads, muscle activity, and ligament stress [
28]. Thus, differences in motor variability may be both a cause and effect of pain and might also contribute to the chronicity of CLBP [
29].
2. Current Insights
There are differences in motor variability between patients with CLBP and pain-free controls during the performance of functional tasks, albeit with some discrepant results between tasks and among studies. Temporal relationships between changes in movement variability and pain and functional capacity were not evident in the longitudinal studies.
Studying isolated movements is required to test biomechanical models and gain insight into mechanically related processes that contribute to the development and course of CLBP, such as intervertebral movements [
59]. When interested in motor variability, however, functional tasks are considered where the DOFs within a task are minimally restricted, because task demands will influence the motor strategies used to complete the task [
60]. Among functional tasks there were differences in motor variability between patients with CLBP and pain-free individuals, but these differences were not consistent.
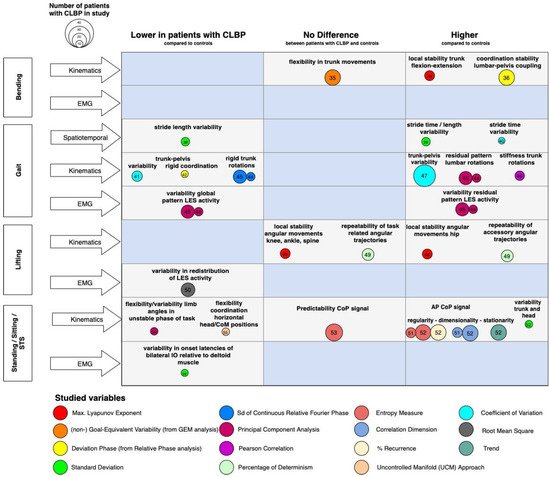
Figure 1 shows that, overall, there were studies that reported high and low variabilities in motor control parameters. To interpret the heterogeneity of the results, it is important to take into account the theoretical framework and associated metrics adopted by the included studies.
Figure 1. Findings and literature gap map of the cross-sectional studies. Legend: Differences in motor variability between patients with CLBP and controls (x-axis) across various functional tasks and levels of measurement (y-axis). The bubbles represent the methodology (in terms of used metrics) and their size represents the number of included patients with CLBP in the study. The numbers in the bubbles represent the references. Knowledge gaps are marked as blue fields. Abbreviations: LES: lumbar erector spinae; CoM: Center of Mass; CoP: Center of Pressure; AP: anterior-posterior; IO: internal oblique.
3. Metrics of Motor Variability
Several studies addressed variability with metrics that provide information about the magnitude of the variability such as RMS, CV, or SD (e.g., of step length, range of motion, EMG) neglecting time-dependent fluctuations and structure in these fluctuations. These conventional metrics fit into a conceptual framework in which motor variability is considered ‘noise’, and low trial-to-trial variability with a low SD reflects consistent behavior, whereas a higher SD might point towards a lack of control [
61]. Over the last years, however, there is a growing interest in within-person and/or intraindividual variability from a dynamical systems perspective, which regards variability as an inherent property of human movement and provides a window to study the coordination of system components as well as its stable and adaptive features. From this perspective, human motor behavior is considered intrinsically variable both within and between individuals, and an in-depth analysis of variability, including both its temporal as well as spatial characteristics, may provide insight into the underlying control structures and mechanisms related to movement impairments [
21,
62,
63,
64].
Most included studies examined motor variability using concepts and tools derived from dynamical systems theory, using numerous computational forms to characterize properties of motor variability such as correlation-based measures (PCA, detrended fluctuations analysis), pattern stability methods (PCA and RP analysis), and predictability-related measures (Recurrence Analysis, λmax, sample entropy, and UCM approach) (
Figure 1). Although all of them address movement dynamics and recognize the importance of movement variability, they are conceptually different. For instance, the λmax quantifies the system’s ability to resist ‘natural’ local perturbations, and weak fluctuations are suggested to indicate local stability that can be steadily maintained. The rate of decay of small perturbations is referred to as local stability [
65]; a system might be locally stable but globally cannot resist larger disturbances. Coordination dynamics describe and predict changes in patterns of oscillating body segments. In patients with CLBP, the variability of trunk-pelvis RP is considered an index of pattern stability [
21]. Similarly, a PCA was used to extract the (in-)variant patterns of segment coordination from the more variable components, as an index of flexibility in kinematics and EMG [
45]. The UCM theorem examines multi-joint coordination in relation to multi-DOF for task performance. It partitions variability as essential and invariant to the task and the variability that affects it [
66]. The UCM provides information about the flexibility of task performance, which was reported to be lower in patients with CLBP [
55]. The λmax, coordination stability, and UMC might thus reflect different motor control characteristics. For instance, fatigue during a lifting task is associated with a higher λmax, while higher pattern stability (expressed by a lower mean and SD of RP) in patients with CLBP in gait is reported.
4. Heterogeneity in Motor Variability
When focusing on the discrepant results among studies and between tasks, the variety in functional tasks and task-specificity, per se, does provide different behavioral repertoires for the human body as a complex system to solve the motor tasks, quantifying a range of movement options inherent to motor variability. Moreover, differences in task constraints may lead to different motor variabilities; during dual-tasking, patients with CLBP might choose different priorities, for instance, maintaining cognitive performance at the expense of the motor task during gait [
43] or vice versa [
38]. The motor solutions available for a given task might serve various goals, such as the stabilization of the spine, maintaining the CoM within the base of support, end-point accuracy, or mitigating fear-avoidance beliefs [
53]. Hence, it is crucial to consider the main goal of the task when analyzing motor variability.
The substantial between-subject variance in motor variability in CLBP could also be driven by the heterogeneity of the CLBP population phenotyping [
7,
8,
9,
10,
11]. Biopsychosocial models suggest that the fear of pain keeps a tight rein on motor behavior in patients with CLBP [
67]. Specific movement adaptations, aimed at minimizing pain or the fear of pain, could be founded through reinforcement learning [
20]. Some functional tasks might not have been threatening enough by individual participants to evoke a protective motor strategy, or motor strategies could be influenced by depressive symptoms, catastrophizing, and somatic anxiety [
68]. A substantial amount of patients with CLBP present increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input, a phenomenon known as central sensitization [
69]. Because central sensitization affects the central nervous system, it is assumed that functioning is related to central sensitization and pain. Nonetheless, the relationship between central sensitization and motor functioning—or, more specifically, motor variability—has not been extensively investigated.
It is widely recognized that CLBP presents as a multidimensional problem [
70]. Remarkably, the researchers found that the studies that addressed motor control and variability scarcely reported the clinical and demographic characteristics of the study sample. Multifactorial models are needed that include clinical and demographic factors to better understand differences in motor variability.
5. Pain Intensity and Patterns of Motor Variability
Proposed contrasts in motor variability between acute and chronic pain suggest that motor adaptations vary across time and might change when the pain is relieved [
71]. Longitudinal studies [
56,
57,
58] observed lower pain intensity and improved functional capacity in patients with CLBP after interventions. In studies with relatively high pain intensity at baseline (VAS 5.55 ± 1.7 [
56], VAS > 4 [
57]), motor variability shifted towards the levels of controls in the follow-up phase; contrastingly, no changes in motor variability (the predictability of the CoP sway) were evident in the intervention group with relatively low pain intensity at baseline (VAS 2.5 ± 0.7) [
58]. A plausible reason for the reduced pain intensity and conflicting results regarding motor variability might be that specific muscles are responsible for pain alleviation and improved neuromuscular coordination, and that there might be a relationship between motor variability, muscle de-conditioning, movement direction, and the type of exercise performed [
72].
6. Changes in Motor Variability in Patients with CLBP: Pathology or Genius Adaptation?
Optimal adaptive variability could possibly have two ends of the spectrum: variability beyond the upper limit, implying an unstable system that is sensitive to perturbations, and variability below the lower limit, implying a stereotypical system without exploratory behavior, which is, therefore, less capable of adapting to perturbations [
71]. This paradigm is manifested in a recently published theory, which proposed the existence of two phenotypes in LBP: ‘tight’ control and ‘loose’ control over trunk movements [
73]. However, the generalization of patients with CLBP during functional tasks and targeting treatments to these phenotypes requires caution. The results of this work indicate that the theory should be elaborated given considerations to the whole range of multidimensional CLBP conditions. The individual-specific motor behaviors attributed to beliefs and attitudes towards pain and the multidimensional clinical representation of CLBP should be covered. Furthermore, the context- and task-specificity of movements might give rise to specific intraindividual motor strategies, shifting the control strategies across the spectrum.
7. Clinical implications
The results of the present review show that it is not viable to identify homogeneous subgroups of patients with CLBP based on motor variability alone. Longitudinal studies, however, indicate that there is the potential for interventions targeting motor variability. Clinically, the results emphasize the need for the development and study of personalized approaches, and single-subject-like designs, to examine interventions.
This entry is adapted from the peer-reviewed paper 10.3390/biomechanics1030030