The RAS plays a fundamental role in the regulation of fluid volume and blood pressure, but it also exerts a large spectrum of effects on several tissues, especially those that are microvasculature-rich, such as the lungs. Renin, a protease produced by renal juxtaglomerular cells in its active form, cleaves angiotensinogen, released mainly by the liver, to form Ang I. A pathophysiological mechanism underlying the cardio-metabolic conditions associated with a greater risk of morbidity and mortality in COVID-19 is the imbalance between ACE and its homologous ACE2, with a decreased activity of the latter and impairment of its protective effects. Similarly to ACE, ACE2 is a ubiquitous enzyme, particularly expressed in the lungs but also present on the enterocytes of the small intestine and on the endothelial cells of several organs and systems, such as the brain, cardiovascular system, and kidney [
10,
11]. ACE and ACE2 are key enzymes in the metabolism of Ang I: ACE, expressed widespread by endothelial cells, catalyzes the conversion of Ang I to the octapeptide Ang II [
12], which exerts its effects via Ang II type 1 and type 2 receptors (AT1R and AT2R, respectively). In particular, binding of Ang II to AT1R is the one most commonly expressed in normal adult tissues, stimulating vasoconstriction, sodium reabsorption, and blood pressure increase, promoting vascular damage, inflammation, and fibrosis [
13]. On the opposite side, ACE2 is a type I transmembrane metallocarboxypeptidase that cleaves Ang I into a nonapeptide [Ang (1-9)] that binds AT2R and Ang II into a heptapeptide [Ang (1-7)] that binds its specific receptor, initially identified as an “oncogene” (Mas receptor, MasR) [
14]. The two main effects of ACE2 are thereby the degradation of Ang II, the principal effector of the “classic” RAS arm through AT1R, and the production of Ang (1-7), which exerts opposite effects by inducing vasodilatation as well as anti-inflammatory and anti-fibrotic pathways through binding to the MasR [
15]. ACE2 also interacts with another sub-branch of RAS based on Ang peptides in which the aminoterminal aspartate is replaced by alanine (Alatensins), leading to the production of Ala-Ang (1-7) (Alamandine) that has been found to bind Mas-related G protein-coupled receptor D (MrgD) and may also protect against lung injury and fibrosis, improving vascular/endothelial dysfunction [
11]. The ACE2/Ang (1-7)/MasR axis has been found to attenuate inflammation and fibrosis in experimental models to prevent heart failure and coronary heart disease [
16], as well as lung injury [
17,
18]. Therefore, ACE2 plays a pivotal role in the modulation of the two main arms of RAS: the ACE/Ang II/AT1R axis (“classic RAS”) and the ACE2/Ang (1-7)/MasR axis (“anti-RAS”). Indeed, ACE2 antagonizes “classic RAS”, playing an essential counter-regulatory role in the activation of the “anti-RAS” [
19]. As SARS-CoV-2 uses ACE2 as a primary receptor to gain entry into human cells, causing its functional down-regulation through internalization and shedding [
20,
21], coronavirus infection leads to a RAS dysregulation, enhancing the ACE/Ang II/AT1R pathway up to vascular “toxicity”, causing microvascular damage and dysregulated vascular permeability. This results in capillary leakage of protein and fibrin-rich edema filling alveolar spaces, also promoting oxidative stress and inflammation, leading to acute respiratory distress syndrome (ARDS) [
9]. Moreover, the ACE/Ang II/AT1R axis is likely to promote the production of inflammatory cytokines, accelerate apoptosis in alveolar epithelial cells and promote extracellular matrix synthesis, resulting in lung fibrosis, a hallmark of tissue injury in SARS-CoV-2-related pneumonia [
22]. On the other hand, Ang (1-7) has been found to mitigate inflammation, counteract lung fibrosis, and improve oxygenation in acute lung injury, acting as a protective factor against ARDS [
17]. The main cardio-metabolic conditions associated with a worse outcome in COVID-19 are intertwined via RAS imbalance at baseline.
3. Overweight, Obesity, Visceral Adiposity and Metabolic Syndrome
Obesity and overweight with visceral adiposity promote increased circulating levels of Ang I, leading to an overproduction of Ang II and hyper-activation of “classic RAS” [
33,
34]. Adipocytes produce and release all the components of “classic RAS”, including angiotensinogen, ACE, and Ang II, with the only exception of renin, even if they express the renin receptor [
35,
36]. Thus, in the context of the aforementioned SARS-CoV-2-induced ACE2 downregulation, it is likely that the increased levels of both Ang I and Ang II coming from visceral adipose tissue lead to an ACE/Ang II/AT1R “storm” affecting the pulmonary microcirculation in obese COVID-19 patients [
37]. In addition, obese subjects show high circulating levels of microRNAs involved in the downregulation of ACE2, resulting in further basal dysfunction of ACE2 compared to healthy subjects [
38]. Adipose tissue is also involved in cytokine and adipokine secretion, contributing to a pro-inflammatory environment. Indeed, leptin, one of the main adipokines secreted by adipocytes, has been found to be related to increased Ang II levels and decreased ACE2 expression [
39]. Moreover, the deficiency of the natriuretic peptide (NP) system, found in obese subjects, mainly due to an increased expression of the clearance NP receptor C [
40], could further contribute to the RAS imbalance in this population. In fact, both A-type (ANP) and B-type (BNP) NPs counteract the typical features of the ACE/Ang II/AT1R axis hyper-activation (endothelial dysfunction and increased permeability, pro-inflammatory, pro-hypertrophic, and pro-fibrotic activity), while experimental studies found that ANP can prevent the reduction in ACE2 mediated by Ang II and, conversely, Ang (1-7) can increase ANP release [
34,
41]. These interactions with RAS, together with their natriuretic and cardio-protective effects against acute cardiac dysfunction that may develop during SARS-CoV-2 infection, give NPs an important role in COVID-19, especially if obesity and heart failure are present [
42].
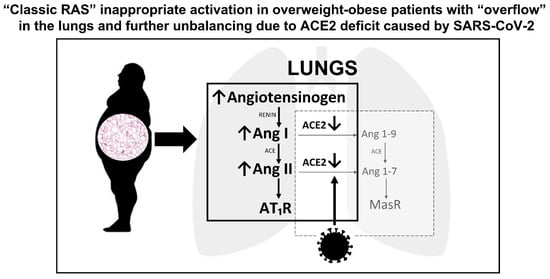
Overall, obesity and overweight can increase the risk for severe COVID-19 through several mechanistic, biochemical, and immunological pathways; among them, the dysregulation of RAS is likely to play a key role in increasing both disease severity and mortality (Figure 1).
Figure 1. Overweight/obesity, renin-angiotensin-system, and lung injury caused by SARS-CoV-2. ACE, angiotensin-converting-enzyme; Ang, angiotensin; AT1R, angiotensin II type 1 receptor; Mas R, Mas receptor.
4. Type 2 Diabetes Mellitus
New-onset hyperglycemia or acute decompensated diabetes mellitus have been frequently observed in COVID-19 patients [47,48]. Moreover, susceptibility to other overlapped secondary infections, together with the use of glucocorticoid therapy, can further precipitate acute hyperglycemia [49] with increased plasma osmolality, osmotic polyuria and dehydration, endothelial dysfunction, thrombophilia, and amplified pro-inflammatory cytokine secretion, all key factors in SARS-CoV-2-related multi-organ dysfunction. In addition, binding of SARS-CoV-2 to ACE2 in pancreatic cells can damage islets and reduce insulin release, leading to acute hyperglycemia and transient diabetes [50]. The evidence that diabetes mellitus causes a pro-inflammatory environment has been corroborated by serum levels of inflammation biomarkers, such as interleukin-6 (IL-6), C-reactive protein (CRP), and ferritin, and D-dimer that are markedly higher in COVID-19 patients with diabetes mellitus compared to controls without diabetes [51]. Generally, diabetes mellitus is associated with weakened immune response and enhanced susceptibility to infections, due to inherent neutrophil dysfunction, reduced T-cell responses, and disordered humoral immunity [52]. As other cardio-metabolic comorbidities, type 2 diabetes mellitus bears the fingerprint of RAS imbalance: indeed, chronic activation of “classic RAS” is typical in diabetes and insulin-resistance, despite high sodium intake and high blood pressure, and contributes to microvascular and macrovascular complications and is clearly involved in diabetic kidney disease [53]. Furthermore, chronic hyperglycemia also reduces the ACE2 expression, with a loss of its anti-inflammatory effects and protection of endothelial function, because of a decreased counter-regulation of Ang II [54,55].
In the context of ACE/Ang II/AT1R axis hyper-activation, the insulin receptor also uses mitogen-activated protein (MAP) kinase as a downstream mediator of its action [35], mediating growth-factor-like effects, such as vascular smooth muscle growth and cardiac hypertrophy [56]. Even AT1R can activate MAP kinase in its post-receptor cascade, so it can be postulated that these two receptors synergize to exacerbate and perpetuate inflammation, fibrosis, and tissue injury. These findings are in line with the hypothesis that RAS dysregulation could be the backbone in the pathogenesis of severe COVID-19 in patients with diabetes mellitus. This vulnerability may play a synergistic role with the underpinning inflammatory milieu and immune defects associated with diabetes, providing SARS-CoV-2 a pathway for causing prolonged lung injury.
5. Arterial Hypertension
Worldwide epidemiologic data provided evidence that hypertension is a pivotal comorbidity related to COVID-19 disease severity. In addition to the hypertensive condition, anti-hypertensive therapy is also likely to affect the course of COVID-19. A large meta-analysis enrolling 101,949 COVID-19 patients found a significant association between treatment with RAS inhibitors and mortality reduction among patients with hypertension [62].
The mechanisms by which hypertension leads to increased risk of worse outcome in COVID-19 are likely to be many. Hypertension is a major cardiovascular risk factor that promotes arteriosclerosis of large and small arteries and accelerates atherosclerosis, leading to cardiovascular disease and death. Left ventricular hypertrophy and myocardial fibrosis, with increased filling pressures and impaired coronary reserve, are key features that contribute to atrial fibrillation, myocardial ischemia, and heart failure with preserved ejection fraction [76]. Certainly, RAS hyper-activation or, at least, “inappropriately normal” renin activity and aldosterone levels are typical of overweight/obese hypertensive patients [33]. In these patients, normal or increased Ang II production results in a stimulation of the ACE/Ang II/AT1R pathway, leading to small arteries constriction, hypertrophy, fibrosis, and tissue injury [77]. It also leads to the activation of NADPH oxidases, with subsequent generation of reactive oxygen species, protein oxidation, and dysregulated cell signaling [78]. Moreover, animal models support a hypothetical link between hypertension and reduced ACE2 expression, corroborated by data showing lower expression of ACE2 mRNA and ACE2 protein expression in the kidneys of hypertensive rats [79].
6. Dyslipidemia
Another risk factor often associated with overweight/obesity and MetS is dyslipidemia. Although its influence may vary, according to age and the presence of other comorbidities, meta-analyses found that dyslipidemia was associated with higher mortality and disease severity [
85,
86]. Atherogenic dyslipidemia was more frequent in patients with critical COVID-19 and was significantly associated with intubation and death. High triglycerides levels were associated with high levels of inflammatory biomarkers and poor COVID-19 outcome during hospitalization [
87].
7. Male Sex
From the early phases of the pandemic, male sex has been found to be associated to a more severe course of COVID-19 and greater need for intensive care, compared with female sex [
102]. Studies found how men had a 59% increased risk for severe outcomes compared to women [
103]. Observational studies reported how the vast majority (82%) of patients that needed intensive care were males [
104] and how the main determinants of ICU admission were male sex and obesity [
105].
Several factors can explain this sex difference. Although the greatest evidence on RAS and sex comes from preclinical studies, both types of sex hormones, estrogens and androgens, likely affect the expression and activity of several RAS components, especially regarding the “classic RAS” pathway, while limited data are available on the interactions with the counter-regulatory RAS components [
108]. Estradiol is likely to cause a protective shift in ACE/ACE2 ratio, by both increasing ACE2 and inhibiting ACE expression [
109]. Estrogenic activity has been found to inhibit the hemodynamic effects of Ang II and promote the action of ACE2/Ang (1-7) axis in animal models [
110]. Estrogen has also been found to decrease tissue AT1R expression and aldosterone production, while testosterone conversely increases ACE activity and tissue AT1R expression [
108]. Furthermore, the gene for ACE2 is located in the X chromosome, which could make it susceptible to escaping X-inactivation in women [
111]. In an animal model of obesity-associated hypertension, the increase in blood pressure after high-fat diet is attenuated in females compared to males, and this different behavior appears to be mediated by ACE2 activity [
112]. In humans, men tend to have higher levels of aldosterone than females, regardless of other confounders, facilitated, at least in part, by higher levels of endogenous Ang II [
113].
8. Older Age
Several factors and age-related modifications are responsible for the increased risk of severe COVID-19 and death in older patients: the large spectrum of multiple cardio-metabolic morbidities, leading to a much higher cardiovascular risk, as well as immune-senescence, endothelial dysfunction, limited organ reserve (especially diminished cardiorespiratory function), and other psychosocial and nutritional factors [
118]. In this large variety of factors, age-related decline in ACE2 expression, as observed in the lungs of rats [
119], may play a non-negligible role. In older people, especially those with cardiovascular comorbidities, reduced ACE2 levels and increased Ang II signaling arrange a pro-inflammatory background. When these subjects are infected with SARS-CoV-2, that leads to a further reduction in ACE2 cell surface expression, there is a consequent overwhelmed amplification of the ACE/Ang II/AT1R pathway that perpetrates microvascular damage and inflammatory effects leading to severe lung injury [
120]. It must be recalled that aging has a major role in cardiovascular disease by substantially “giving time” to multiple risk factors, even “borderline” in severity, to produce vascular damage through decades of inappropriate control [
121]. When infections strike these older patients, the clinical scenario may often complicate with acute cardiovascular events, leading to more severe clinical course and worse outcome.