IgG antibodies can cross and do cross the placenta during pregnancy from the mother to the fetus. The passage starts by the end of the first trimester and continues throughout pregnancy. This is a manner by which the fetus gets passive humoral immunity from the mother. In the early neonatal period, these transferred maternal antibodies will act as a defense and help the developing immunity of the baby. While they are short-lived and cleared from the neonatal circulation within several months, they may be very helpful.
A down-side is that in certain maternal autoimmune conditions auto-antibodies seem to have the capacity to hijack the transfer mechanism. It is the case for anti-Ro antibodies. These antibodies are frequent in women with systemic lupus erythematosus and/or Sjogren syndrome. They can lead to fetal atrioventricular block.
1. Introduction
Immunological adaptative changes occurring during pregnancy allow maternal tolerance towards the fetus and placenta, which practically constitute semi-allografts as 50% of their antigens have a paternal provenience [
1]. This complex process mediated by maternal hormone levels and the placenta represents the fundament of a normally evolving pregnancy. Any breakdowns in this process may lead to maternal anti-fetal rejection and consequently to serious complications such as preterm birth, premature rupture of membranes, placental abruption or stillbirth [
2]. During normal pregnancy, there is a physiological transfer of immunoglobulins from the mother to the fetus, with the aim of providing essential protection during the first few months of life when neonatal humoral response is inefficient.
The placenta has an extremely important function throughout gestation. It is a histological barrier formed by three layers: (1) multinucleated syncytiotrophoblasts (STB) with a cytotrophoblast layer directly beneath, (2) stroma containing fibroblasts and Hofbauer cells and (3) endothelial cells of the fetal capillaries [
3]. There are active and passive mechanisms that allow transfer of low molecular weight substances from the mother to the fetus. Immunoglobulin G (IgG), although it has a high molecular weight, is the only class of immunoglobulins able to cross the placenta and to reach the fetal circulation.
IgG is a large protein with a tetrameric structure, containing two heavy and two light chains disposed in a Y-like shape. In its structure, there is an antigen binding site (Fab region) and a constant region, the crystallizable fragment (Fc), which binds to Fc receptors found on the surface of different cells in the immune system, most importantly on phagocytes. There are four types of IgG (1–4), and all of them are transferred across the placenta via syncytiotrophoblast cells that express receptors for the Fc domain, called neonatal Fc receptors (FcRn) [
4,
5,
6].
Active transplacental transfer starts early in the course of pregnancy, at about 13 weeks of gestation, and fetal levels of IgG increase with advancing gestational age, being relatively low between 17 and 22 weeks at about 5–10% of maternal levels, then by 32 weeks reaching 50% of maternal levels, and finally exceeding maternal plasma IgG levels at birth [
7].
Besides gestational age as an important factor in the transfer of antibodies, the process is influenced by several aspects such as maternal immunocompetence, concomitant infections, specific antibody levels acquired postimmunization, placental integrity, class of IgG and type of antigen [
7]. These variables represent the basis for strategies regarding maternal immunization, aiming to protect newborns against infectious diseases, and also for the development of special surveillance protocols in situations such as maternal autoimmune or alloimmune conditions where harmful antibodies transferred across the placenta may cause severe fetal complications.
2. Physiological Transfer of IgG
2.1. Role of FcRn
Neonatal Fc receptor is a major histocompatibility complex class I (MHC)-related molecule that plays a central role in the regulation of IgG homeostasis and transport across the placental barrier [
8]. Expression of FcRn on syncytiotrophoblast cells appears to be decisive for efficient IgG-mediated phagocytosis [
9], whereas expression on endothelial cells is important to prolong IgG half-life by recycling internalized IgG back to the surface [
10].
The interaction between the Fc domain of IgG and FcRn is influenced by pH changes, presenting high affinity at acidic pH level < 6.5 and low affinity at physiologic pH [
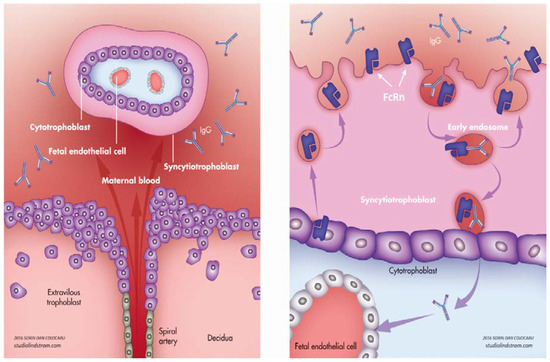
11]. During pregnancy, IgG is transferred from mother to fetus at the level of syncytiotrophoblasts through a process called transcytosis, which starts with internalization of maternal IgG into endosomes. At this level, the pH is acidified and it allows IgG to bind to FcRn present on the internal surface of the endosome [
12]. The complex is then carried towards the basal cell membrane of the syncytiotrophoblast, where the IgG is released upon exposure to normal pH (7.4) and it enters the fetal circulation (). It is not yet fully understood how maternal IgG is carried through villous stroma to the fetal endothelial cells as FcRn are not expressed on stromal cells [
13,
14]. Some evidence shows that Fc receptors type II and III are expressed in term placentas and could be involved in transplacental transfer of IgG [
15]. It remains controversial whether FcRn are expressed or not on fetal endothelial cells, but Fc receptors II could be identified at this level and are considered to be linked with IgG passage into the fetal circulation [
16,
17].
Figure 1. Transplacental passage of immunoglobulin G (IgG) and the neonatal Fc receptor. IgG from the maternal blood (left) is transferred by transcytosis at the level of syncytiotrophoblasts (STB); it is internalized within endosomes and binds to FcRn on the internal surface; the complex is then carried towards the basal cell membrane of STB and released into the fetal circulation (right). Purple arrows indicates IgG transport to the fetal blood.
In humans, FcRn are also expressed on both endothelial and bone marrow-derived cells, playing a role in prolonging the half-life of IgG and albumin [
18,
19] by preventing their catabolism. This finding might have a great impact in clinical practice: by modulating this IgG–FcRn interaction, one could improve the pharmacokinetics of therapeutic antibodies, or by inhibiting FcRn function in some autoimmune conditions, a reduced level of harmful antibodies could be achieved [
20,
21,
22].
2.2. Timing of IgG Transfer and Other Influencing Factors
The transplacental transfer of maternal antibodies to the fetus begins during the first trimester of pregnancy. Very little maternal IgG reaches the embryo and could be found in the coelomic fluid and villous stroma as early as 6 weeks [
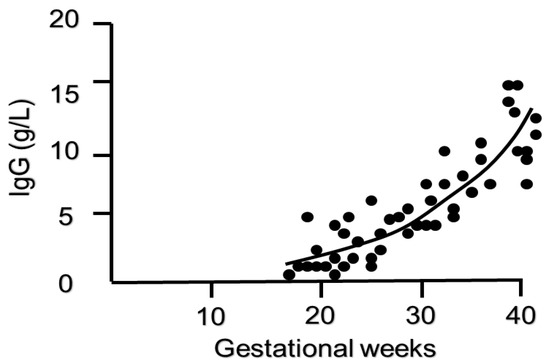
23]. Approximately 10% of maternal IgG concentrations are transferred to the fetus by 17–22 weeks’ gestation, and the levels show a continuous rise between 17 and 41 weeks, exceeding maternal levels by 37–40 weeks of gestation [
24] (). Due to this marked transfer of antibodies in the third trimester, closer to term, preterm neonates especially those born before 32 weeks have a considerably lower level of IgG compared to full term neonates and therefore higher susceptibility to infections [
25,
26,
27]. Preterm infants also show a more rapid and earlier decrease in IgG in the postpartum period than term infants [
28]. As passive immunization through transplacental maternal IgG transfer is not enough for preterm neonates, administration of intravenous immunoglobulin (iv IgG) after birth has been considered, although with limited benefits in reducing mortality or morbidity. A recent Cochrane meta-analysis tested the hypothesis that intravenous immunoglobulin supplementation in preterm or low birth weight neonates might reduce the risk of infections and any complications related to nosocomial infections. Data from more than 5000 infants enrolled showed that prophylactic use of iv IgG resulted in 3% reduction in sepsis and 4% reduction in severe infection, but without having a significant impact on neonatal mortality or other important neonatal outcomes such as length of hospital stay. Consequently, there is no general recommendation on prophylactic use of iv IgG in preterm neonates and there should be an individualized decision based on local resources. These results were consistent with previous data published in 2013 [
29].
Figure 2. Timing of IgG transfer across the placenta in pregnancy (adapted from Malek A et al., Evolution of maternofetal transport of immunoglobulins during human pregnancy, Am J Reprod Immunol, 1996) [
24].
The immunoglobulin rise in the fetal circulation is different between the four types of IgG. The fastest transfer was observed for IgG1 and the slowest for IgG2. At term, in the fetal circulation IgG1 level was seven times higher than IgG2 level. There are also differences between the two IgG types compared to maternal levels: fetal IgG1 level exceed the maternal concentration near term or after birth, while fetal IgG2 remain below maternal level [
24,
30]. These differences were considered to be due to a preferential transfer of natural killer (NK) cell-activating antibodies, which could be explained through different affinities of neonatal Fc receptors towards specific components (glycans) in the Fc region [
31].
Serum maternal immunoglobulin levels correlate to the placental transfer and neonatal IgG levels. Higher maternal IgG levels, above 15 g/L, have a negative influence on transplacental IgG passage and correlate to lower neonatal IgG levels, although in normal conditions fetal IgG levels in the third trimester surpass the maternal concentration. Paradoxically, when maternal level is too high, as is the case in maternal hypergammaglobulinemia, FcRn are oversaturated and unbound IgG molecules are destroyed [
7], leading to decreased fetal antibody transfer. A similar effect is observed in black women, who normally have a higher level of total IgG than white women; therefore, one could say that transplacental transfer is correlated to maternal race [
32].
On the other hand, in immunocompromised women secondary to HIV infection, reduced humoral immune response and reduced antibody production are linked with poor transfer of antibodies against specific pathogens such as group B streptoccocus, pertussis or Haemophilus influenzae [
33,
34]. In women with primary immunodeficiency with underlying specific gene mutation, exogenous IgG administration is essential to prevent severe maternal and fetal infections. It was observed that in these cases, immunoglobulin transfer across the placenta is similar to the transfer of endogenous antibodies [
35].
With an unclear mechanism of impairment, placental malaria has been associated with reduced IgG transplacental transfer [
34].
2.3. Maternal Immunization
2.3.1. Vaccination
Pregnancy is associated with a particular background as the maternal immunological response is inhibited in order to tolerate the fetus and placenta. Some infectious diseases may be more severe during pregnancy, thus the most effective way to provide protection for the mother and the newborn is vaccination. Current guidelines recommend administration of inactivated vaccines, while live vaccines are contraindicated at least 4 weeks before conception and definitely during pregnancy. Vaccines routinely administered during pregnancy include inactivated influenza vaccine and Tdap, with some others such as those against pneumococcus, meningococcus, hepatitis A and hepatitis B being justified under specific circumstances [
36].
Influenza vaccine in pregnancy was introduced in 2004 as part of a routine immunization program. It was observed that pregnant women are at greater risk of developing severe complications following influenza infection and that immunization in pregnancy, irrespective of trimester [
37], reduces this risk and additionally provides protection for their newborns in the first few months of life [
38].
A study on 112 mother–infant pairs highlights the strong correlation between maternal and neonatal antibody levels and the importance of passive immunity in newborns. As a consequence of low maternal immunity, only 30%, 42% and 82% of infants had protective antibody levels to pertussis, Haemophilus influenzae type b (Hib) and tetanus, respectively. Therefore, a high proportion of neonates are susceptible to those infections until active immunization is allowed [
39]. In this context, Tdap (tetanus and diphtheria toxoids and acellular pertussis antigens) vaccination in pregnancy has proven its safety and significantly increases the titers of antibodies against those antigens. It is recommended from the second trimester, with best results when administered between 27 and 36 weeks of gestation and repeated in each pregnancy [
40]. Administration in the third trimester provides the highest neonatal specific antibodies and prevents neonatal pertussis disease in the first 5–6 months of life until infants receive active immunization through vaccinations [
41]. Enhanced placental transfer is influenced by maternal IgG levels, type of IgG and time between vaccination and delivery. It was shown that IgG type 1 preferentially crosses the placenta, compared to other types; therefore, polysaccharide conjugated vaccines such as group B streptococcus or pneumococcus conjugated to Tdap are able to preferentially induce maternal IgG type 1 production and to have a better impact on neonatal IgG levels [
42].
It is important to mention that higher doses of passively acquired antibodies may suppress the immune response after vaccination in early infancy [
43]. Several studies reported that maternal antibodies transferred across the placenta during pregnancy can decrease infant immunologic response to measles, tetanus and whole cell pertussis vaccines, with consequent production of lower levels of antibodies postimmunization [
44,
45,
46]. Despite this disadvantage, the benefits for newborns in the first few months of life in terms of reducing hospitalization, decreasing the risk of mechanical ventilation and even decreasing the risk of death support the current recommendation of maternal Tdap immunization in the third trimester of pregnancy.
Due to general vaccination programs, most data showed high seropositivity for measles, mumps, rubella and varicella-zoster (VZV) in women of childbearing age. Maternal antibodies and transplacental passage protect newborns in the first few months of life against most vaccine-preventable diseases, and this protective level is maintained up to 6 months of age. In normal conditions, the rubella, measles or VZV antibody titer in the cord blood of neonates born at term exceeds maternal antibody levels. There is a high prevalence of anti-rubella and anti-VZV protective IgG titers, but there is a decreasing trend in anti-measles and anti-mumps immunity levels in pregnant women and neonates. Therefore, new preventive strategies have been proposed, such as measles-mumps-rubella (MMR) screening and vaccination of susceptible women of childbearing age or MMR vaccination of women who have no documentation of completed vaccination and no laboratory evidence of immunity [
47,
48,
49]. Live vaccines such as MMR and varicella vaccines are contraindicated during pregnancy, and maternal serologic status should be checked before conception in order to prevent any possible infections during pregnancy by appropriate preconceptional immunization [
50].
Passively acquired maternal antibodies with different antigen-specificities have been found to have different half-lives in infants. For example, although in normal pregnancy pertussis-specific IgG levels in cord blood achieve more than 100% of maternal levels, maternal pertussis-specific IgG has a half-life of 6 weeks in infants and decreases to undetectable levels as early as 4 months of life [
51]. In contrast, maternal passively acquired measles-specific IgG remains near protective levels at 6 months after birth and is still detectable at 1 year of life.
Ongoing efforts are being made to develop future vaccines for maternal immunization, the two most promising vaccines being respiratory syncytial virus vaccine, in phase III trial, and group B streptococcus vaccine to prevent late-onset neonatal infection, currently in the early stages of development. A vaccine against cytomegalovirus is also under development [
36,
52,
53,
54].
New emerging viruses with potential harm for the fetus, such as the Zika and Ebola viruses, have also been under investigation for the development of future vaccines [
55,
56].
2.3.2. Maternal Infection with COVID-19
The greatest challenge of our time is the COVID-19 pandemic, and special attention has been drawn to pregnant women and their infants in terms of vertical transmission, severity of the disease and immunologic response. Although there is no clear evidence of vertical transmission due to lack of angiotensin-converting enzyme 2 (ACE2) receptors for SARS-CoV-2 virus in the placenta [
57], the immunologic status at birth was investigated in 71 neonates born to mothers with confirmed infection. Immunoglobulin M (IgM) does not cross the placenta; it is a result of fetal immunologic response to pathogens, an ability that is acquired early in the first trimester of pregnancy. IgG in the fetal blood at birth is a result of maternal immunoglobulin transferred across the placenta. In 20% of the investigated cases, IgM was detectable after birth and in one case it was positive at 2 h postpartum, but the PCR remained negative after multiple determinations and we should take into account cross-reactivity and false positive rate of IgM results before making any assumptions [
58].
In a small cohort of six infants born to mothers with COVID-19 infection, IgG was present in all cases and the neonatal level was well correlated with maternal immunoglobulin levels. However, the study did not investigate whether the presence of antibodies in the neonates had a protective effect against infection as there was no long-term neonatal antibody level follow-up [
59]. One case report showed that IgG to SARS-CoV-2 in the neonate decreased in less than one and a half months after delivery, suggesting the potential risk for subsequent COVID-19 in neonates. The presence of IgG and immunoglobulin A (IgA) antibodies was confirmed in breast milk, indicating that breastfeeding might have an important immune protection for infants after birth [
60,
61]. Current recommendations state that for assessing future vaccine efficacy, maternal vaccination should be considered early in the design of these trials [
62].
3. Pathological Transfer of IgG—Autoimmune Disorders
Transplacental immunoglobulin transfer plays an important role in protecting the newborn in the first few months of life, when the immune system is immature and active immunization through vaccination is not yet recommended. Despite this clear benefit, there are situations in which transplacental transfer may be damaging to the fetus.
4. Pathological Transfer of IgG—Alloimmune Disorders
Around 50% of fetal antigens have a paternal origin, and maternal immunization to different fetal antigens inherited from the father, unrecognized as ″self″, determines an immune response with production of antibodies and placental transfer into fetal circulation leading to destruction of different fetal cells, mainly blood cells.
5. Pathological Transfer of IgG—Biological Therapy in Pregnancy
Numerous autoimmune disorders have been identified so far, and almost 80% are encountered in women of childbearing age [
122]. The evolution of autoimmune disorders is variable during pregnancy. In some situations, the disease is triggered by pregnancy or the postpartum period; some conditions relapse or are aggravated during gestation; some autoimmune disorders ameliorate under the immunosuppressive influence of pregnancy. For example, rheumatoid arthritis or systemic sclerosis might improve during pregnancy while systemic lupus erythematosus, myasthenia gravis or inflammatory bowel disease might present a worse evolution with gestation [
123,
124,
125,
126]. For a better outcome, it is recommended to plan conception when the disease is in remission or well controlled, and recent evidence indicates that treatment should be adapted and continued during pregnancy in order to minimize the risk for the mother and the fetus.
Anti-tumor necrosis factor alpha (anti-TNFα) antibodies are probably the most studied biological therapy used in pregnancy. Anti-TNFα antibodies such as infliximab and adalimumab are IgG1 antibodies that have a preferential transfer across the placenta starting at the end of the second trimester; therefore, neonatal drug levels may exceed maternal levels and may persist up to 12 months after birth [
127]. Etanercept, a fusion protein with a modified Fc portion that binds to TNFα, has a low capacity to cross the placenta, and minimal levels are found in the fetus at birth. Certolizumab, an anti-TNF therapy missing the Fc portion, does not cross the placenta and can be used throughout pregnancy.
The current data show that pregnancies exposed to anti-TNFα are not associated with an increased risk of fetal malformations, preterm delivery or pregnancy loss [
128,
129,
130]. One of the main concerns, when the fetus is exposed in utero to biological therapy, is the risk of neonatal infections, particularly in the first year of life [
131]. The observational data indicate that infants exposed to anti-TNF agents are not at greater risk of severe infections compared to the unexposed population, unless thiopurine therapy (azathioprine) is involved. In this case, the risk can be three times higher [
128]. Current recommendations regarding the use of biologics during pregnancy advise the discontinuation of medication at 20 weeks of gestation for infliximab and adalimumab and around 32 weeks for etanercept [
132]. If the medication is continued beyond 28 weeks, the drug levels in the fetus will exceed those in the mother, and precautions and close monitoring are required after birth. A large database of 1457 pregnant women with inflammatory bowel disease receiving anti-TNFα medication, mainly infliximab and adalimumab, showed that discontinuation of treatment before week 24 increased the risk of maternal disease flare. Almost 50% of the patients continued the medication during the third trimester of pregnancy and a third of them until the time of delivery, and there was no increased risk of neonatal infection or infections during the first year of life [
133]. Live vaccines are contraindicated in the first six months of life, especially BCG vaccine (Bacillus Calmette–Guérin) [
134].
Initially used to compensate for the deficient immune response in immunocompromised patients, iv IgG is now a widely used therapy in autoimmune and systemic inflammatory diseases [
135,
136]. Iv IgG is obtained from plasma of healthy blood donors and also has applicability in a wide range of pathologies associated with pregnancy. Its clinical utility comes from its ability to interfere with FcRn. Large quantities of exogenous IgG determine saturation of FcRn and as a result, the excess of pathological IgG that could not bind to FcRn will be destroyed. Consequently, there will be lower levels of pathological maternal antibodies transferred to the fetus [
12,
137].
Preventing harmful antibodies from reaching the fetal circulation, iv IgG is currently used in autoimmune thrombocytopenia, myasthenia gravis and systemic lupus erythematosus [
138]. Also, iv IgG represents the first line of therapy in preventing recurrence of neonatal alloimmune thrombocytopenia, initiated early in the first or second trimester of pregnancy [
139,
140]. Hyperimmune intravenous immunoglobulin is the subject of investigation for preventing congenital cytomegalovirus infection in women with primary infection in the first trimester of pregnancy. The results of the studies undertaken so far are conflicting, and at the moment there is no clear recommendation on routine iv IgG therapy for primary maternal cytomegalovirus infection [
141,
142].
6. Conclusions
The transplacental passage of maternal IgG antibodies is of great importance to the fetus and newborn, offering suitable protection until maturation of the immune system and until active immunization through vaccination is allowed. On the other hand, in some conditions such as maternal autoimmune disorders or maternal immune responses against paternally inherited fetal antigens, the physiological passage of immunoglobulin can have a deleterious effect upon the fetus to various degrees of severity and with potential long-term implications.
This entry is adapted from the peer-reviewed paper 10.3390/diagnostics10080583