Restless legs syndrome (RLS) is a sleep-related movement disorder characterized by an unpleasant urge to move the lower limbs. The prevalence of RLS varies by region, ethnicity, sex, and age, ranging from 5–15% . Its pathophysiology remains unclear. Criteria for the diagnosis of RLS include the International Restless Legs Syndrome Study Group (IRLSSG) and International Classification of Sleep Disorders, Third Edition (ICSD-3). The ICSD-3 criteria require distress and associated sleep disturbance, which is different from the IRLSSG consensus [2]. As for the measurement of disease severity for RLS, the IRLSSG rating scale (IRLS) was proposed. It assesses a range of RLS related symptoms and their impact on patients’ mood and daily life, and it has been proved reliable, valid, and responsive in clinical trials.
1. Introduction
Restless legs syndrome (RLS) is a sleep-related movement disorder characterized by an unpleasant urge to move the lower limbs. The prevalence of RLS varies by region, ethnicity, sex, and age, ranging from 5–15% [
1]. Its pathophysiology remains unclear. Criteria for the diagnosis of RLS include the International Restless Legs Syndrome Study Group (IRLSSG) and International Classification of Sleep Disorders, Third Edition (ICSD-3) [
2,
3]. The ICSD-3 criteria require distress and associated sleep disturbance, which is different from the IRLSSG consensus [
2]. As for the measurement of disease severity for RLS, the IRLSSG rating scale (IRLS) was proposed. It assesses a range of RLS related symptoms and their impact on patients’ mood and daily life, and it has been proved reliable, valid, and responsive in clinical trials [
4].
Pharmacologic therapies for RLS include dopamine agonists, alpha-2-delta calcium channel ligands, and iron supplements [
5]. Several non-pharmacological interventions have been proposed to treat RLS, such as repetitive transcranial magnetic stimulation, exercise, compression devices, counter-strain manipulation, infrared therapy, and acupuncture; however, they have relatively low quality of evidence [
6]. Despite the treatments mentioned above, about 45% of patients remain unchanged or are worse [
7,
8]. Therefore, finding alternative therapies that complement the conventional treatments would be beneficial.
In patients with RLS, hyperalgesia in the leg was revealed in previous studies [
9,
10,
11]. Besides, 21.4% to 61% of RLS patients have described their symptoms as painful [
12]. Additionally, botulinum neurotoxins (BoNT) may relieve hyperalgesia and pain probably through blocking the release of pain mediators in the peripheral terminals, dorsal root ganglia and spinal cord neurons [
13,
14,
15,
16]. Hence, we may expect improvements in patients with RLS after BoNT treatment. However, controversies exist in the effect of BoNT in RLS [
17,
18,
19,
20,
21,
22,
23], and no articles have evaluated this topic systemically.
2. Results of Quantitative Synthesis
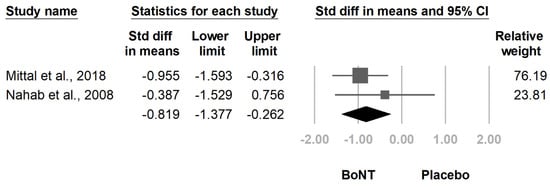
The meta-analysis included two randomized controlled trials [
19,
23]. Compared with placebo, botulinum toxin injection significantly reduced IRLS score at four weeks after injection (SMD, −0.819, 95% CI, −1.377 to −0.262,
I2 = 0.0%,
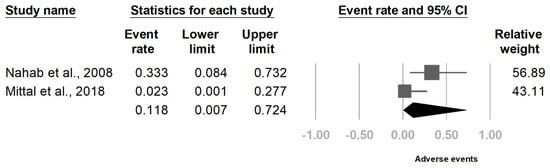
Figure 3). The rate of adverse events after botulinum toxin injection was 11.8% (95% CI, 0.7–72.4%,
I2 = 70.3%,
Figure 4). The primary and secondary outcomes showed low and moderate between-study heterogeneity, respectively. Publication bias was not assessed due to the low number of studies.
Figure 3. Forest plot of standardized mean differences in International Restless Legs Scale (IRLS) score. Squares indicate effect of individual studies, lines indicate 95% CI, and the diamond indicates the summarized effect size.
Figure 4. Forrest plot of adverse event rate in the intervention groups after botulinum toxin administration. Squares indicate the rate of individual studies, lines indicate 95% CI, and the diamond indicates the summarized result.
3. Current Insights
Our systemic review and meta-analysis suggested that intramuscular botulinum toxin injection decreased the IRLS score in patients with RLS. Although a few patients complained about adverse events after injection, no serious adverse events were recorded in the articles enrolled in our review.
The results of our meta-analysis corresponded to our initial hypothesis. Our meta-analysis only included randomized controlled trials, which decreased the possible bias caused by placebo effect [
30] and ensured the robustness at the evidence level. Furthermore, the low statistical heterogeneity suggested that there might be a correlation between botulinum toxin and an improvement of symptoms in RLS. The fact that no adverse events recorded after BoNT injection may further assure future studies to apply BoNT in patients with RLS. However, these results should be interpreted with caution due to low number of articles included.
Differences between the results of the included studies may be caused by low statistical power, the dose of BoNT, or the muscles injected. The trial conducted by Nahab et al. [
23] had a small sample size of six participants, which might cause a type II error. As for the dose of BoNT and the target muscle of injection, we proposed a hypothesis by comparing the studies included in our review. Although no evidence has revealed a conversion factor between incobotulinumtoxinA and onabotulinumtoxinA in patients with RLS, a 1:1 conversion rate is usually accepted in clinical practice [
31]. Under this assumption, Mittal et al. [
19] and Agarwal et al. [
18] had at least two times the dose of BoNT in the tibialis anterior compared with Nahab et al. [
23]. Meanwhile, both Mittal et al. and Agarwal et al. but not Nahab et al. reported a significant decrease in IRLS score after BoNT treatment. This may imply that higher doses of BoNT per muscle especially to the tibialis anterior may be necessary to create positive effects in treatment of patients with RLS, while the total dose may not be the critical factor. This hypothesis may also explain the negative results of Ghorayeb et al. [
22], which applied BoNT intradermally. Additionally, a research poster in 2007 concluded that patients with RLS might benefit from 40 to 50 units of onabotulinumtoxinA applied to each tibialis anterior, which corresponded to our hypothesis [
20].
This entry is adapted from the peer-reviewed paper 10.3390/healthcare9111538