Many phase III trials failed to demonstrate a survival benefit from the addition of molecular therapy to conventional chemotherapy for advanced and metastatic gastric cancer, and only three agents were approved by the FDA. Despite recent advances in surgical techniques and in anticancer drugs, and the adoption of perioperative treatments mostly based on conventional chemotherapy, the prognosis of advanced and metastatic gastric cancer remains poor. In the last decade, the addition of molecular therapy did not show any significant survival advantage, and the first reports available documented an increase of the rate of severe adverse effects and related mortality. The survival benefits of molecular therapies available to date for advanced and metastatic gastric cancer are rather unclear, mostly due to inaccurate patient selection, particularly concerning oncogene amplification and copy number.
1. Introduction
Gastric cancer is one of the most frequent malignancies. It represents the fifth most frequent cancer worldwide (5.6%) and the fourth leading cause of cancer-related death (7.7%) with 768,793 deaths per year in 2020 [
1].
Surgical resection with optimal lymphadenectomy is the only curative treatment in cases of AGC [
2,
3,
4,
5,
6]. In recent decades, several perioperative and postoperative regimens of conventional CT have been investigated, and neoadjuvant treatment has been recommended as mandatory in several national guidelines, but the prognosis of stage III and IV GC remains poor [
7,
8,
9,
10]. In 2014, Cancer Genome Atlas Research Network paved the way for a new molecular classification of GC and documented the existence of four subtypes: EBV (9%), MSI (22%), CIN (50%), and GS (20%) [
11]. The identification of these subtypes and the related signaling pathways provided a roadmap for GC patient stratification and promising strategies for targeted therapies. Trastuzumab was the first MT approved by the FDA and European Union for AGC; it was subsequently introduced as the standard of care for patients with locally or fAGC displaying HER2 overexpression/amplification [
12]. In 2014, the FDA also approved the use of ramucirumab as monotherapy or in combination with paclitaxel for advanced and metastatic GC [
13]. To date, only these two MTs (in addition to the antibody–drug conjugate trastuzumab deruxtecan) have been approved, although many other molecular targets have been identified in recent years. Indeed, the majority of phase III trials investigating novel molecular agents failed to demonstrate their efficacy, mostly due to inaccurate patient selection (particularly concerning driver gene amplification and copy number) and the lack of preclinical models supporting proof of concepts followed by structured trials. PDXs are helpful in validating and predicting the response to novel MTs, even though these models are unable to reproduce the same conditions and environmental characteristics of the donor tumor and very rarely allow metastatic dissemination [
14]. For this purpose, PDOXs were recently introduced in GC preclinical research to better recapitulate the original cancer background [
15].
In 2016, the Cochrane Collaborative Group published a systematic review with the aim of assessing the efficacy and safety of MTs available for the treatment of advanced and metastatic gastric cancer [
16]. The authors identified 11 RCTs enrolling a total of 4014 patients with AGC who underwent conventional CT and MT or conventional CT alone. They concluded that the benefit of MTs on survival was unclear and pointed out a significant increase in side effects.
2. Molecular Targets and Target Agents
2.1. Epidermal Growth Factor Receptor
2.1.1. Anti-HER1
Many authors have demonstrated that approximately 30% of GCs show HER1 overexpression [
17,
18]. Two main monoclonal antibodies (cetuximab and panitumumab) that reduce HER1 activity by binding its extracellular domain have been identified. Moreover, cetuximab can stimulate the activity of the immune system against tumor cells [
19]. Unfortunately, the heterogeneity of GC seems to affect the efficacy of cetuximab in most of these patients [
20].
Gefitinib and erlotinib, two tyrosine kinase inhibitors, can also inactivate HER1 by binding its intracellular domain and blocking its kinase activity [
21]. Unfortunately, phase II trials have shown that these therapies have limited efficacy [
22,
23]. Recently, Maron et al. and Corso et al. identified a subpopulation of GC patients presenting a high level of EGFR amplification, which is responsive to anti-EGFR drugs [
24,
25]. They also identified mechanisms of resistance to EGFR-targeted drugs, such as TKR activation, KRAS mutation/amplification, and TSC2 inactivation [
25].
2.1.2. Anti HER2
Several authors have shown a direct relationship between HER2 amplification (and the consequent overexpression of its receptor) and many types of tumors [
26]. The HER2 gene is a proto-oncogene located on chromosome 17q21. The first drug binding HER2 was trastuzumab. In 2010, the ToGa trial documented the superiority of trastuzumab in combination with conventional chemotherapy compared with chemotherapy alone in terms of OS and DFS for patients with AGC [
12]. Nevertheless, only a few patients with GC (less than 20%) gain a real advantage from trastuzumab.
In the past decade, several other anti-HER2 agents have been tested for GC treatment. Lapatinib is a dual kinase inhibitor that acts on EGFR (ErbB1) and HER2 (ErbB2) with the consequent downregulation of HER2 signaling [
27].
Pertuzumab is an anti-HER2 monoclonal antibody that prevents heterodimerization between HER2 and other HER family members [
28].
2.2. Vascular Endothelial Growth Factor
VEGFs are proteins promoting blood vessel formation. Four types of VEGF (VEGF-A, VEGF-B, VEGF-C, and VEGF-D) have been identified, with three types of corresponding receptors (VEGFR-1, VEGFR-2, and VEGFR-3). Several studies have reported the fundamental role of these signaling proteins in new blood vessel formation and cancer cell proliferation [
34]. Furthermore, VEGF expression has been found in approximately 40% of GC [
35]. Bevacizumab is an anti-VEGF-A monoclonal antibody that inhibits circulating VEGF-A activity [
36]. The efficacy of this monoclonal antibody has been widely documented in several solid tumor treatments [
37,
38,
39] but bevacizumab is still under investigation for its benefit in GC. Some phase II/III trials proved its efficacy in association with conventional chemotherapy in AGC, while others did not report any clear benefits [
40,
41].
2.3. Mammalian Target of Rapamycin
mTOR is a serine/threonine protein kinase identified in mammalian cells with a leading role in controlling mechanisms of cell growth and proliferation. Human cancers can be characterized by hyperactivity or inactivity of the mTOR pathway, which plays a crucial role in maintaining tumor-modified phenotypes [
48].
.4. Hepatocyte Growth Factor Receptor
HGFR, also known as c-MET, is a proto-oncogenic receptor tyrosine kinase that, after binding to hepatocyte growth factor, induces cell migration and proliferation, promotes mitosis, and inhibits apoptosis. C-MET overexpression and gene amplification are related to a poor prognosis [
50,
51].
Crizotinib (PF-02341066) is a tyrosine kinase inhibitor of the c-MET receptor and of the TKR anaplastic lymphoma kinase; it has been approved by the FDA for treatment of ALK-positive NSCLC patients.
Another promising agent targeting the HGF-cMET complex is rilotumumab. This human monoclonal antibody impairs the c-MET signaling pathway by binding to and inactivating its ligand HGF [
53]. Clinical trials of this drug in GC (including two phase III trials) were halted due to a significant increase in mortality in the experimental arm (rilotumumab in combination with conventional chemotherapy) in one of these trials, but new investigations have begun.
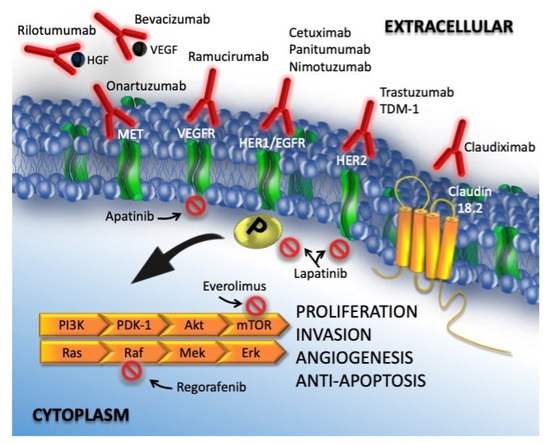
In Figure 1, targeted therapies and oncogenic pathways in gastric cancer are detailed.
Figure 1. Targeted therapy and oncogenic pathways in gastric cancer. Activation of ERK-AMP KINASE: ligand binding to a growth factor receptor activates the small GTP-binding RAS protein, which interacts with RAF protein kinase. RAF phosphorylates and activates MEK (MAP kinase or ERK kinase), which then activates ERK (extracellular signal-regulated kinase) by phosphorylation of tyrosine and threonine residues. Activated ERK translocates into the nucleus where it phosphorylates the Elk-1 transcription. PI3K/AKT/MTOR Pathway: PI3K/AKT/MTOR signaling constitutes an important pathway that consists of two steps: phosphatidylinositol 3-kinase (PI3K) and its downstream molecule serine/threonine protein kinase B (PKB; also known as AKT). The PI3/AKT/mTOR pathway is stimulated by RTK and cytokine receptor activation. Tyrosine residues are then phosphorylated and provide anchor sites for PI3K translocation to the membrane, thus participating in the transduction of various extracellular matrix molecules and cytokines, including mTOR, a serine/threonine protein kinase and a member of the PI3K-associated kinase protein family.
2.5. Preclinical Trials
Preclinical trials have proved to be valuable tools to derive molecular information to better target GC for innovative MTs and stratify patients for clinical trials. The use of organoids, PDXs, and PDOXs in GC research showed interesting patient related tumor characteristics and cancer escape mechanisms. Several authors reported a strong relationship between higher levels of HER2 amplification/copy number and increased benefit of Trastuzumab in AGC [
30,
62].
3. Molecularly Targeted Therapies for Gastric Cancer
GC is still characterized by a poor prognosis, particularly in cases of metastatic or recurrent disease and in locally advanced stages. The identification and introduction of effective and safe molecular therapies in clinical practice lag behind other malignancies, such as lung and breast cancers.
Unfortunately, findings showed that molecular therapies do not provide a clear survival benefit compared to conventional CT in the case of advanced or metastatic GC.
In 2016, the Cochrane group published the largest systematic review and meta-analysis investigating the survival benefit of MTs for GC patients, with or without conventional treatment. The Cochrane authors identified 11 RCTs (phase II and III studies), and the conclusion was “Adding molecular-targeted treatment to chemotherapy may have a small effect on survival and on stopping further development of the disease, compared with chemotherapy alone, but the evidence is of low quality”.
In the past five years, only eight new phase III RCTs have been conducted.
Most of these studies failed to demonstrate the superiority of MT with or without conventional CT compared with conventional treatment alone or with placebo in terms of survival outcomes. Moreover, two of these eight trials were terminated prematurely. The METGastric Phase III trial was stopped early because of negative results reported in a concomitant Phase II study that concluded: “The addition of onartuzumab to mFOLFOX6 in gastric cancer did not improve efficacy in an unselected population or in a MET immunohistochemistry-positive population” [
74,
75]. The RILOMET-1 was interrupted prematurely because a safety control committee found more deaths in the experimental arm than in the control arm during a planned interim analysis of safety and survival outcomes [
70].
The RCT published by Li was the only positive study; it reported a clear survival benefit in patients with GC treated with apatinib (a VEGFR2 inhibitor) compared with those receiving a placebo in terms of both OS (7.6 vs. 5.0 months,
p = 0.0027) and PFS (2.8 vs. 1.9 months,
p < 0.001), with an acceptable SAE rate [
69]. Accordingly, in 2014, the China Food and Drug Administration approved the use of apatinib as a third-line treatment for metastatic GC.
Despite this positive report, the overall meta-analysis did not show any significant differences in OS and PFS between the experimental (MT) and control arms.
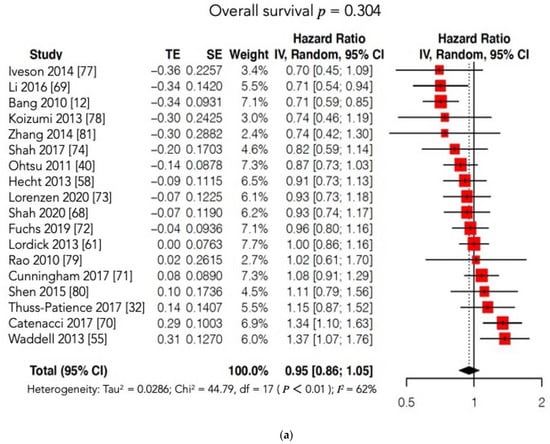
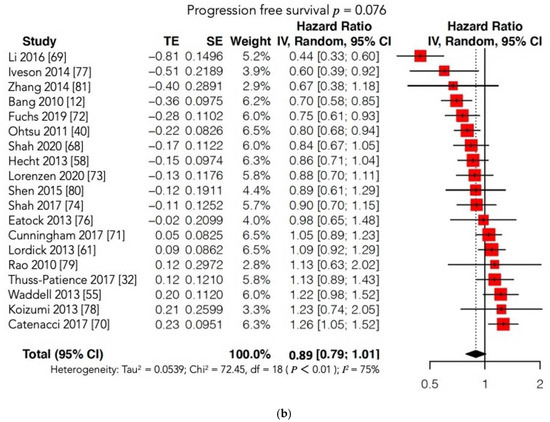
Furthermore, the subgroup analysis according to the type of MT administered (VEGFR or c-MET inhibitors) failed to show a significant prolongation of OS and/or PFS in the experimental arm. Notably, our results may have been unable to identify significant differences between the two arms due to the high heterogeneity found among the included studies. On account of this statistical bias, we conducted two further meta-analyses matching our OS and PFS findings with those reported in the Cochrane review [
76,
77,
78,
79,
80,
81] (
Figure 7a,b;
Table S1). Regrettably, these new cumulative analyses maintained high heterogeneity and could not document any survival advantage when MT was added to conventional treatment or administered alone compared to conventional CT or to a placebo.
Figure 7. (a) Forest plot of comparison: molecular-targeted therapy alone/plus chemotherapy versus chemotherapy alone/placebo. Main analyses; outcome: overall survival (data from Cochrane and present review pooled). (b) Forest plot of comparison: molecular-targeted therapy alone/plus chemotherapy versus chemotherapy alone/placebo. Main analyses; outcome: progression free survival (data from Cochrane and present review pooled).
Quality of life was mentioned only in the study by Li et al. [
69] and in the RAINFALL study [
72] without any significant differences between the two groups.
Finally, the number of serious adverse effects and SAE-related deaths did not increase in the experimental arm. Additionally, the analysis of secondary outcomes confirmed that, to date, the supposed advantage of the administration of MT vs. conventional CT alone is unclear.
In addition, most of the investigated targeted therapies available to date are very expensive; therefore, it is mandatory to evaluate the cost-effectiveness as well. In 2017, Chen et al. [
82] evaluated the relationship between the efficacy and the costs of apatinib as a third-line treatment in metastatic GC and concluded that this type of treatment is not cost-effective at all, while another author stated that apatinib is likely to be cost-effective only for patients with solid insurance [
83]. Other authors analyzed the cost-effectiveness ratio of ramucirumab + paclitaxel as a second line treatment in AGC as proposed by Wilke et al. [
47], concluding that this regimen was cost-ineffective and suggesting that its indirect charges to society be considered [
84,
85].
Finally, although three MTs have been approved by the FDA (trastuzumab, trastuzumab–deruxtecan, and ramucirumab) and a fourth one by the China Food and Drug Administration (apatinib), most phase III RCTs assessing novel molecular agents failed to demonstrate a survival advantage over conventional treatments. Consistent with the literature, we found four possible reasons for these negative results.
First, only in recent times has GC undergone wide investigational programs from a molecular perspective, which has highlighted the importance of patient selection because of the high number of molecular mutations found in GC [
86]. Indeed, several molecular alterations characterizing GC subtypes have been identified and analyzed in the past decade, as in the case of CIN tumors, which manifest the most frequent TKR amplifications, and in the case of 80% of EBV tumors, which display
PIK3CA mutations [
87].
Second, GC is often characterized by a high grade of heterogeneity, both inside the primary tumor and in distant metastases. Several studies clearly demonstrated the intratumoral heterogeneous pattern of HER2 and c-MET expression [
88,
89]. Some authors have suggested inactivating alterations to the phylogenetic tree trunk because they promote cancer growth and are present in every tumor cell [
90]. Unfortunately, no trunk mutations have been discovered in GC.
Third, several preclinical trials have recently documented a strict relationship between c-MET amplification and copy number and the response grade to anti-MET therapies [
91,
92] and that c-MET expression alterations are found in only 2% of GCs. However, in clinical trials investigating anti-MET agents, no patient selection was done. This could be one of the reasons for RILOMET-1 and METGastric trial failure.
Finally, many studies have shown different escape mechanisms of cancer cells that could shorten the duration of or even nullify the response to targeted therapies [
93,
94]. For example, c-MET-addicted GC could overcome c-MET blockade through HER family receptor expression activation. Recently, Apicella et al. showed that combined molecular therapy with anti-MET/EGFR leads to a complete and durable response [
91]. For this reason, PDX and PDOX are valuable preclinical tools in validating new targeted therapies tailored to patients’ cancer molecular expression [
14,
15,
95].
4. Conclusions
The results showed that despite their newly documented safety, the molecular therapies available to date for advanced and metastatic gastric cancer do not present clear survival benefits. These unfavorable results are mostly related to inadequate patient selection. Targeted therapies are promising treatments for patients with locally advanced, metastatic, or recurrent gastric cancer as they are for other types of tumors. However, their clinical validation requires accurate patient selection, particularly related to driver oncogene amplification and copy number, and it should take into account preclinical models investigating cancer heterogeneity and escape mechanisms.
This entry is adapted from the peer-reviewed paper 10.3390/cancers13164094