Ceramic composites based on alumina and zirconia have found a wide field of application in the present century in orthopedic joint replacements, and their use in dentistry is spreading. The development of this class of bioceramic composites was started in the 1980s, but the first clinical applications of the total hip replacement joint were introduced in the market only in the early 2000s. Since then, several composite systems were introduced in joint replacements. These materials are classified as Zirconia-Toughened Alumina if alumina is the main component or as Alumina-Toughened Zirconia when zirconia is the main component. In addition, some of them may contain a third phase based on strontium exa-aluminate. The flexibility in device design due to the excellent mechanical behavior of this class of bioceramics results in a number of innovative devices for joint replacements in the hip, the knee, and the shoulder, as well in dental implants.
1. Introduction
Oxides are among the most stable inorganic materials since no further oxidative processes (e.g., corrosion, ion release) can take place. This is a major reason for the use of oxides as ideal bioceramic materials since the 1960s because their chemical inertness was considered as the basis for biocompatibility. The first ceramic oxide used in orthopedics was alumina (Al
2O
3), while ceramic composite oxides, prevalently made of alumina-zirconia (Al
2O
3-ZrO
2) were subsequently developed, seeking improved mechanical performance [
1].
The first use of alumina as a biomaterial is due to Dr. Sami Sandhaus, a Swiss dentist, who in 1962 developed a screw-shaped dental implant named Crystalline Bone Screw—CBS
® and used it in a significant number of cases [
2]. In 1963, L.W. Smith and J.F. Estes (Haeger Potteries, Dundee, IL, USA) developed Cerosium
TM as a bone substitute in case of large bone defects, i.e., a silica aluminate matrix where pores (about 50% in volume) were filled with epoxy resin [
3].
At that time, hip arthroplasty was taking its first steps. Although keenly interested by the potential of such a procedure, orthopedic surgeons were very concerned about the failures of implants due to the wear of bearings. The cooperation between Dr. Boutin—an orthopedic surgeon working in Pau, a town in Southern France—and one of his patients, the manager of a factory sited nearby manufacturing high alumina electric insulator, led to the first total hip replacement (THR) with an alumina-on-bearing in 1970 [
4]. Such an implant had a stainless-steel stem and a Ultra-High Molecular Weight Polyethylene (UHMWPE) socket—soon replaced by a socket made of alumina—both cemented into bone.
In the same years, several scientists in Germany (i.e., G. Langer in Keramed, G. Heimke in Friedrichfeld, H. Dörre in Feldmüle, M. Saltzer in Rosenthal) gave a decisive contribution to the development of alumina for orthopedic components and overall for alumina as a biomaterial. This resulted in the development of a number of ceramic orthopedic devices, among which it is worthwhile to mention the BIOLOX
® alumina developed by H. Dörre in Feldmüle (now CeramTec GmbH), which became “
the ceramic” in orthopedics until this attribute was overtaken by the higher-performing BIOLOX
® delta alumina–zirconia ceramic composite [
5].
Indeed, alumina showed critical issues particularly related to failure of THR implants [
6], leading some manufacturers to withdraw from the market of implantable ceramics. Alumina exhibits low fracture strength and toughness and is very sensitive to microstructural flaws that lead to a poor resistance to stress concentration or mechanical impact. As the presence of intergranular pores and large grain size are the main microstructural features that affect the mechanical strength of alumina, the efforts of ceramists were focused on decreasing the porosity and the grain size in alumina ceramics. This was obtained by the selection of proper precursors (e.g., alkoxide-derived powders) and by the optimization of the overall manufacturing process, from batch preparation to final densification by hot isostatic pressing (HIP). Such improvements resulted in the so-called “third generation alumina” based on high-purity precursors and characterized by finer grain size and density near the theoretical one, as illustrated in
Table 1.
Table 1. Selected properties of alumina, evidencing the development of the material [
5].
| Property |
Units |
First-Generation Alumina
(1970s) |
Second-Generation
(BIOLOX®, Since 1974) |
Third-Generation
(BIOLOX®Forte Since 1995) |
| Al2O3 content |
vol.% |
99.1–99.6 |
99.7 |
>99.8 |
| Density |
g cm−3 |
3.90–3.95 |
3.95 |
3.97 |
| Av. grain size |
μm |
≤4.5 |
4 |
1.75 |
| Flexural strength |
MPa |
>300 |
400 |
630 |
| Young’s modulus |
GPa |
380 |
410 |
407 |
| Hardness |
HV |
1800 |
1900 |
2000 |
Nevertheless, the feasibility to obtain alumina components with specific design was limited by its typical brittle fracture behavior [
7]. In response to these issues, the company Desmarquest (now Saint Gobain Céramiques Avancées Desmarquest—SGCAD, Evreux, France) followed a different approach: they focused their attention on a different, intrinsically tough ceramic, Yttria-stabilized Zirconia Polycrystal (Y-TZP). Zirconia (zirconium dioxide, ZrO
2) is characterized by the polymorphism of its crystal lattice; therefore, it exists in three thermodynamically stable crystalline phases: monoclinic (up to 1170 °C), tetragonal (1170–2370 °C), and cubic (2370–2680 °C). Effective applications of zirconia ceramics in medicine were made possible since the discovery of the stabilization of the tetragonal phase at room temperature based on the introduction of small amounts of oxide phases as stabilizers. Such a discovery led to the development of Partially Stabilized Zirconia (PSZ) [
8] because the low concentration of the stabilizing oxide did not allow the full stabilization of the cubic phase. PSZ was firstly obtained by using calcium oxide as stabilizer, but successively either magnesium oxide (magnesia, MgO) or yttrium oxide (yttria, Y
2O
3) were used for this purpose. The real breakthrough in the development of zirconia ceramics occurred in 1975 with the publication of the research paper “Ceramic Steel?” by Garvie, Hannink, and Pascoe [
9]. They reported the increase in toughness in MgO-stabilized PSZ (Mg-PSZ) due to the transformation of the tetragonal phase into monoclinic. Such a transformation, taking place in a “martensitic” way as in some steels, results in an effective dissipative mechanism for fracture energy and, finally, in a self-toughening effect.
More recently, Gupta et al. [
10] reported that a tetragonal zirconia ceramic showing grain size ≈0.3 to 0.5 µm could be obtained by using 2–3 mol% of Yttrium Oxide (Yttria—Y
2O
3) as a stabilizer, thus resulting in minimal residual cubic and monoclinic zirconia. Since then, although many studies had been dedicated to materials stabilized by CaO, MgO, and CeO, the main zirconia ceramic that was developed industrially for the production of medical devices was the one stabilized by Y
2O
3. The tetragonal grains in Y-TZP—being metastable—can shift to the monoclinic natural form at the expense of an external source of energy, i.e., the elastic stress field that yields an advancing crack. Thus, phase transformation results as an efficient dissipative mechanism for the energy that otherwise would lead to fracture. Indeed, it was evaluated that the tetragonal–monoclinic phase transformation implies (for a free grain) a volume expansion 4–5 vol %. As each grain is constrained by its neighbors (the matrix), the constrained phase transformation generates a compressive stress field that increases the energy threshold that a crack has to overcome to develop further. These concurrent, energy-dissipative, microscopic-scale phenomena above outlined result, at a macroscopic level, in the remarkable bending strength and toughness of Y-TZP (see
Table 2).
Table 2. Selected properties of Y-TZP. Alumina data reported for comparison.
| Property |
Units |
Alumina
(1970s) |
Y-TZP |
| Al2O3 Content |
vol % |
99.1–99.6 |
-- |
| ZrO2 Content |
vol % |
-- |
>99 |
| Av. Grain Size Al2O3 |
µm |
≤4.5 |
0.3 |
| Density |
g/cm3 |
3.90–3.95 |
6.02 |
| Thermal Conductivity |
W/mK |
30 |
2.5 |
| Hardness |
HV |
2000 |
1200 |
| Flexural Strength |
MPa |
>300 |
1000 |
| Fracture Toughness |
MPa m½ |
3.5 |
4.5 |
| Young Modulus |
GPa |
380 |
210 |
Several manufacturers worldwide started the production of Y-TZP ball heads. Among them, SGCAD—the main manufacturer of zirconia (Y-TZP) ball heads worldwide—and Kyocera (Kyoto, Japan) developed also zirconia knee condylar components for total knee replacements (TKR).
The metastability of Y-TZP is the key for its outstanding mechanical performances. However, the metastability of Y-TZP was a cause of concern since the beginning of the clinical use of Y-TZP components. In the biologic environment, Y-TZP may spontaneously transform from tetragonal to monoclinic, drastically decreasing its mechanical properties [
11]. Such an undesired phenomenon is named aging or low-temperature degradation (LTD). In THR bearings, the onset of LTD at the surface of the component is related to an increase of the surface roughness, in turn leading to the wear increase of UHMWPE acetabular cups that are usually coupled to Y-TZP heads [
3]. The studies on the physicochemical mechanisms giving rise to LTD are still running: several models have been proposed to explain such a behavior, but none have been fully satisfactory to date [
12], although it is acknowledged that LTD kinetics is promoted by temperature (especially for T > 100–150 °C), by the presence of water in the environment, and by applied stresses. In addition, different LTD kinetics were observed in Y-TZP ball heads obtained from different manufacturers or from different batches produced by the same manufacturer, thus leaving open the main questions about the possible influence of the production process on LTD [
13]. Finally, the unexpected high rates of failure in some batches of Y-TZP since 2000 [
14] led to the abandon of its use in orthopedics.
3. Alumina Zirconia Composites: Early Studies
The abandon of zirconia in 2001 opened a technological gap, leaving unmet the urgent need of ceramic components for arthroplasty with effective design and increased reliability and longevity. Then, materials scientists turned their attention toward different zirconia-toughened ceramics (ZTCs), and promising results were obtained in the development of ceramic composites to be used as biomaterials in orthopedics. The work was focused on composites having alumina (in Zirconia-Toughened Alumina—ZTA) as the main component or zirconia (Alumina-Toughened Zirconia—ATZ).
Special attention was devoted to ZTAs. The basic concept of a ZTA material is to substantially increase the material fracture toughness and strength with respect to alumina, while maintaining relevant properties of alumina such as hardness, stiffness, and thermal conductivity, which are key factors for its successful clinical use in joint replacements. This is achieved by exploiting the tetragonal-to-monoclinic phase transformation of zirconia, which is introduced in ZTA as a reinforcing element. The key point for the excellent mechanical properties of ZTA ceramics is the transformability of the tetragonal zirconia. As a consequence, essential aspects are to retain a significant amount of the zirconia tetragonal phase at body temperature and its degree of stabilization in order to reach the desired toughening mechanism. The proper selection of the stabilizing oxide, the homogeneous and finely distribution of Y-TZP in the alumina matrix, and the control of the microstructure and grain size are key parameters to “tune” the stability of the tetragonal phase. In addition, the compressive residual stresses that develop on cooling, due to the mismatch in thermal expansion coefficients between the alumina matrix and the dispersed zirconia phase, increase the energy threshold for the T-M phase transformation, contributing to the strength of the composite [
16].
This aspect is critical in the design of a ZTA composite: higher tetragonal zirconia stabilization as a consequence, for example, of a too high yttria concentration would lead to suppression of the zirconia phase transformation, then losing almost all the improvements of ZTA. On the other hand, poor zirconia stabilization—i.e., due to zirconia uncontrolled grain growth because of inappropriate sintering processes—would enhance the LTD of the material. Nevertheless, in the latter case, the mechanical properties might be outstanding, but the material could have unreliable performance, thus leading to catastrophic consequences due to the LTD of the zirconia phase.
Furthermore, it is perceived that the toughening mechanisms in monolithic Y-TZP and ZTA are significantly different. In monolithic zirconia, the stress induced by the single transformed ceramic grain makes the neighbor tetragonal zirconia transform as well, consequently spreading the transformation effect throughout the material. Such a transformation results in LTD and deterioration under long-term usage. In the case of alumina–zirconia composites, the zirconia phase is constrained in the stable alumina matrix, thereby preventing the transformation of the adjacent grains. Hence, the ZTA has a better retention of the tetragonal phase compared to the monolithic zirconia, when exposed to hydrothermal conditions in vitro [
19].
The first studies on alumina–zirconia composites as biomaterials started during the mid-1980s by French researchers (INSA-Lyon, Ecole Centrale de Lyon) looking for a material strong and tough as zirconia but characterized by better resistance to LTD [
20]. Among the tested material, a hot-pressed ZTA (Alumina-20 vol % Y-TZP) showed bending strength (four-point bending) higher than 1100 MPa and fracture toughness of about 10 MPa√m. Aging tests carried out using small bars implanted under the skin of Wistar rats—then in unloaded conditions –showed a limited decrease of the strength due to LTD. Laboratory wear tests (pin-on-disk, cylinder-on-flat) carried out against UHMWPE demonstrated an improved friction and wear behavior of hot-pressed ZTA in comparison with Y-TZP [
21].
A further research project was carried out in the framework of the EUREKA programme (project EU 294) under the scientific coordination of the Italian Ceramic Centre (Bologna, Italy). The main goals attained were the production by slip casting of ZTA ball heads with several Z/A ratios [
22,
23] and the assessment in a hip simulator of the wear behavior of ZTA-UHMWPE bearings. Wear tests were carried out in a hip simulator using Alumina-UHMWPE bearings as the reference. The results did not show significant differences between the experimental and reference material [
24]. Cytotoxicity assays confirmed the absence of harmful effects elicited by the composite materials [
25].
3. Alumina–Zirconia Composites in Orthopedics
Zirconia-Toughened Alumina
The first ceramic composite introduced into the orthopedic market in 2002 was the alumina matrix composite (AMC) BIOLOX
®delta, made by CeramTec GmbH, Plochingen, Germany [
26,
27]. As reported by Burger [
28], such a material was made of a fine-grained, high-purity alumina matrix (approximately 80 vol %) combined with three different oxides, so as to retain the relevant properties typical of alumina such as stiffness, hardness, thermal conductivity, but improving fracture toughness and strength. To this aim, such an alumina matrix contained a tailored amount of zirconia phase (i.e., ≈17 vol %), on the basis of indications provided by Pecharromán et al. [
29], to obtain the best compromise between appropriate mechanical performance and chemical stability.
Previous works described the addition of strontium oxide (SrO) to the base formulation, with the purpose of activating solid-state reaction with alumina during sintering and triggering the in situ growth of elongated strontium hexa-aluminate (SrAl
12O
19—SHA) crystals with a magneto-plumbite structure. These platelet-shaped SHA grains, homogenously dispersed in the ceramic composite matrix, increased the toughness of the material through a mechanism of crack deflection/bridging. The effectiveness of this approach was demonstrated by Cutler et al. [
30], who investigated a three-phase system formed by a 12 wt % Ce-TZP matrix containing Al
2O
3 and SHA platelets nucleated in situ during sintering. The maximum platelets length is about 5 µm with an aspect ratio of 5–10.
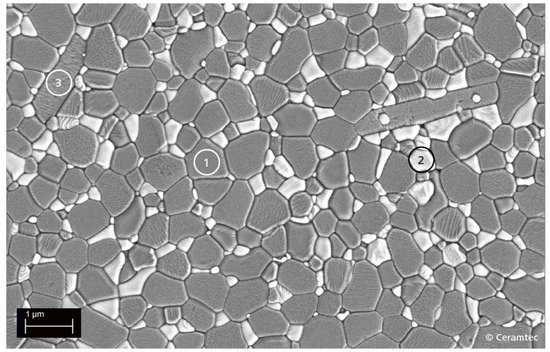
Figure 1 shows the microstructure of BIOLOX
®delta, where the gray-colored grains represent the alumina matrix, while the white-colored grains represent the zirconia phase.
Figure 1. SEM image of the microstructure of the AMC composite ceramic BIOLOX®delta (Courtesy CeramTec GmbH, Plochingen, Germany). The gray grains (1) are the alumina matrix, the white grains (2) are the zirconia phase, and the elongated grains (3) consist of reinforcing strontium hexaaluminate (SHA) platelets.
Then, two mechanisms are concurring to toughen and to reinforce such a composite: on one hand, the phase transformation of Y-TZP triggered by the tensile stresses in proximity of a crack tip is an effective energy-dissipative mechanism. On the other hand, the volume expansion associated to the T-M transformation is contrasted by the high stiffness of the alumina matrix, thus resulting in a compressive stresses field, which is highly effective in blocking the cracks propagation. Furthermore, the elongated zirconium aluminate crystals—formed upon solid-state reaction between alumina and zirconia during the sintering process—gave an additional contribution to the enhancement of the mechanical performance, acting indeed as short fibers capable of increasing the fracture strength and exerting an additional toughening effect. In addition to the reinforcing components, there are minor stabilizing oxides added to the material, giving additional effects such as specific coloring, such as the example of doping alumina with little chromium oxide amount (Cr2O3), which gives the material its characteristic pink color.
CeramTec BIOLOX®delta is considered as the golden standard for ceramics in joint replacements bearings. BIOLOX®delta—which is characterized by a pink color, patented in the European market—is presently used for the production of ball heads that are manufactured in nine different diameters from 22 to 44 mm with four different neck lengths. The production of inserts is more differentiated, because it considers not only the inner but also the external design of the insert, to comply with the metallic shells of the different cup design now on the market.
A number of new ceramic devices were developed thanks to the behavior of AMC, as illustrated in
Figure 2. This is including THR ball heads expressly designed for use during revision surgeries, ceramic components for knee replacements, humeral heads for shoulder replacements, and ceramic hip resurfacing implants [
31].
Figure 2. AMC BIOLOX® delta products (Courtesy CeramTec GmbH, Plochingen, Germany).
Kyocera Medical Corp (Kyoto, Japan—formerly Japan Medical Materials) followed an original approach. The company is a historical manufacturer of fine ceramics for biomedical applications, the first implants of its alumina Bioceram
® may be traced back to 1976. In 2010, Kyocera developed a ZTA (BioCeram
® AZ209) where zirconia is stabilized in the tetragonal state by residual stresses only [
32]. This is obtained by fine tuning of the grain size during cooling.
A more complex composite was released to the market in 2015 under the trademark of Bioceram
®AZUL, which was likely chosen for its characteristic blue color [
33,
34]. AZUL contains approximately 19 wt % zirconia and 2 wt % oxide additives mixed with high-purity fine alumina. The addition of a mixture of oxides characterized by platelet-like grains, such as TiO
2, MgO, Co
3O
4, SiO
2, and SrO, aimed to reduce the grain size and induce the precipitation of platelet-like SHA grains. Additives used in the ZTA synthesis, except for silicon, were located in that platelet-like grain, substituting for strontium and/or aluminum [
35]. Stress relaxation due to the zirconia particles and the crack-diverting effect of S6H crystals are relevant factors promoting the high strength and toughness of Bioceram
®AZUL.
A further ZTA (25 vol % Y-TZP, alumina balance) was introduced on the orthopedic market under the trade name Symarec
® on 2015 by Mathys Orthopedie (Bettlach, Switzerland), who incorporated the company Keramed (formerly Keramik Werk Hermsdorf—KWK Moesdorf, Germany). Keramed is among the pioneers in bioceramics, manufacturing alumina Bionit
® since the early 1970s. Symarec
® contains 25 vol % Y-TZP finely dispersed in the alumina matrix (75 vol %) [
36].
This entry is adapted from the peer-reviewed paper 10.3390/jcs5080206