Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), as with the influenza virus, has been shown to spread more rapidly during winter. Severe coronavirus disease 2019 (COVID-19), which can follow SARS-CoV-2 infection, disproportionately affects older persons and males as well as people living in temperate zone countries with a tropical ancestry. The available data are consistent with optimal warming and humidifying of inspired air by the nose (nasal air conditioning) being essential for minimising SARS-CoV-2 infectivity of the upper respiratory tract (URT) and, as a consequence, severe COVID-19.
- COVID-19
- gender
- genetic factors in SARS-CoV-2 susceptibility
- innate immunity
- nasal conditioning of inspired air
- SARS-CoV-2 infectivity
- upper respiratory tract immunity
1. SARS-CoV-2 Infection in the Upper Respiratory Tract
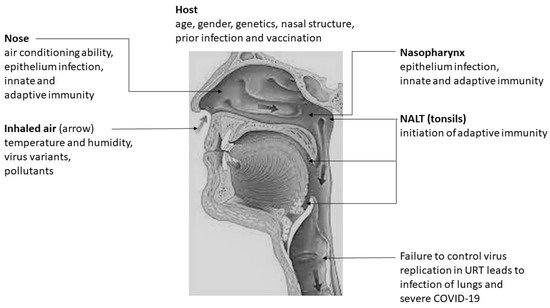
Recent molecular studies demonstrate that SARS-CoV-2 viral load and the expression of host proteins needed for infection, are higher in the nasal epithelium than the lower respiratory tract, and therefore that the nasal epithelium is the probable initial infection site followed by infection of the pharynx as a result of mucociliary clearance of virus towards the nasopharynx and later the likely seeding of the lower respiratory tract and lungs by aspiration [29,30,31], as is the case with influenza viruses [32]
2. Innate and Adaptive Immune Response in the Upper Respiratory Tract in Protection against SARS-CoV-2 Infection
Innate immune mechanisms, analogous to those characterised in influenza virus infections [12,13,14], that can also protect against infection by SARS-CoV-2 in the URT are summarised in Table 1.
| Induction | Effector Cell or Molecule | Effector Mechanism |
|---|---|---|
| - | Naturally occurring mucins, defensins and collectins | Bind virion and prevent cell binding and entry |
| Altered surface of the virion and virus-infected cells |
Complement | Activation through the alternate or lectin pathway to promote lysis and opsonisation, inflammation |
| Pathogen associated molecular pattern (PAMP) recognition by pattern recognition receptors (PRRs) | Type 1 (α,β) and Type 3 (λ) interferons (IFNs) | Induction of anti-viral state in infected and neighbouring cells through inhibition of protein synthesis and mRNA degradation. Activation of phagocytic cells and dendritic cells |
| PRR | Inflammasome in macrophages and dendritic cells | Production of IL-1, IL-6 and TNF that promote an inflammatory response in tissue, fever and the synthesis of acute phase proteins |
| PRR | Macrophage and dendritic cell synthesis of IL-12, IL-18 |
Activation of NK cells to lyse virus infected cells and enhancement of adaptive immune response |
| Stress molecules expressed by infected cells |
γδT cells secreting Type 2 IFNγ |
Activation of NK cells, phagocytes, dendritic cells and the adaptive immune response |
An adaptive or antigen-specific immune response follows soon after an innate or non-antigen-specific immune response and the principal adaptive immune mechanisms that can protect against infection by SARS-CoV-2 in the URT are summarised in Table 2.
| Effector Molecule or Cell | Mechanism of Action |
|---|---|
| Secreted IgA antibodies in mucus | Prevention of virion binding to epithelial cells by agglutination and neutralization of virions |
| IgG and IgM antibodies in mucosa and blood, including anti-A and anti-B blood group antibodies |
Prevention of virion binding to host cells through agglutination and neutralization, activation of complement through the classical pathway, promoting opsonisation and phagocytosis, assisting NK cell killing through Fcγ receptors |
| CD4+ TH lymphocytes | Activation of B cells, promoting immunoglobulin class switching and affinity maturation, secretion of cytokines like IFNγ that activate phagocytes and NK cells and upregulate major histocompatibility complex molecules. |
| CD8+ cytotoxic lymphocytes | Apoptosis of virus-infected cells by granzyme, perforin, etc. |
3. Humidity of Inspired Air and Protection against SARS-CoV-2 Infection
The multiple ways in which humidity may affect the stability of respiratory viruses and the mucosal barrier function have been recently reviewed [37] and may be summarized as follows for the URT: (i) airborne enveloped viruses may be more stable at low and high humidities and less stable at intermediate humidities, (ii) mucoepithelial integrity is decreased by inspired air of low humidity, and (iii) mucocilary clearance, which removes virions trapped in the mucus from the airway, is reduced at low humidity. Inadequate humidification of inhaled air of relatively low moisture content that is characteristic of winter may, therefore, be expected to enhance infection of the URT epithelium by SARS-CoV-2.
4. Temperature of Inspired Air and Protection against SARS-CoV-2 Infection
Low temperature affects the stability of respiratory viruses in the environment and also compromises mucosal barrier function [37,49]. There is evidence to suggest that SARS-CoV-2 survives better at lower temperatures in human nasal mucus and sputum [50], which is pertinent to both airborne and fomite transmission. Essentially, it can be surmised that lower than optimal temperatures in the URT: (i) may improve the stability of the lipid bilayer in enveloped viruses, (ii) reduce the mucociliary clearance of viruses, (iii) compromise URT-epithelium repair during infections [37,49], and (iv) adversely affect the Type 1 and 3 interferon dependent early innate immune responses in the URT [55-58].
Colder-than-normal inspired air in winter may be expected to produce temperatures in parts of the nasal cavity that are lower than its usual 33-34°C, thereby, likely further facilitating the infectivity of SARS-CoV-2 in the nasal epithelium and nasopharynx. The relationships between the temperature of inspired air, intranasal temperatures, and nasal air conditioning have not been systematically studied to date. However, modelling studies showed that the anterior nasal cavity is responsible for most of the warming of inspired air [59].
5. Nasal Air Conditioning and Genetic Differences in Susceptibility to SARS-CoV-2 Infection
Defects in specific genes involved in the Type 1 and 3 interferon pathway increase the risk of developing severe COVID-19 and this may likely be due to a failure to control SARS-CoV-2 infection in the URT [57,58]. Additionally, recent GWAS have identified large segments of human chromosomes inherited from Neanderthals that are associated with a major risk for susceptibility [60] or protection [61] against severe COVID-19. These two studies did not identify specific genes responsible for susceptibility or protection but demonstrated a variable distribution of the relevant chromosomal regions in different parts of the world.
The differential susceptibility and resistance to a variety of human infectious diseases are governed by genetic factors [62] and are particularly well studied in malaria [62,63,64,65]. However, genetic factors that specifically affect the initial infectivity of SARS-CoV-2, in contrast to the severity of ensuing COVID-19, have not been clearly established. The nearest experimental approach to investigate this difference recently examined SARS-CoV-2 RNA test positivity separately from disease phenotype in a US-based GWAS [66]. The results showed that blood group O was significantly associated with reduced SARS-CoV-2 test positivity and an association between some types of tropical ancestry and SARS-CoV-2 test positivity [66]. It is possible to hypothesise that the blood group O association is due to protection conferred in the URT by natural anti-A and anti-B antibodies universally present in blood group O individuals acting against infecting virions carrying membrane A and B antigens derived from infecting individuals of blood groups A and B.
Variations in nasal structure between human populations living in geographically disperse locations with different climates have been correlated with the greater need to humidify and warm inspired air during cold and dry winters on one hand and the correspondingly reduced need for this in warm and humid climates of the tropics on the other [67,68,69]. It is reasonable to postulate that selection by respiratory viral infections in temperate zones in ancient times may have been a factor that contributed to such nasal variations. SARS-CoV-2 may, therefore, be more infectious in temperate zone countries to persons with a tropical ancestry [66] due to a weaker nasal air conditioning ability, and that this may contribute, in addition to socio-economic factors, to their observed propensity to develop more severe COVID-19 [23,24].
6. Differences in Nasal Air Conditioning and the Age and Gender Differences in Susceptibility to SARS-CoV-2 Infection
7. Other Factors Influencing Susceptibility to SARS-CoV-2 Infection
8. Conclusions
This entry is adapted from the peer-reviewed paper 10.3390/ijms22157919