1.1. Copper as an Antibacterial Agent
The contact-killing ability of copper surfaces was studied with respect to bacteria in the early 1980s due to the emerging of hospital superbugs. In 1983, Kuhn [
64] compared the bioburden on doorknobs made of brass and stainless steel and found that brass doorknobs showed reduced pathogenic growth in the healthcare environment compared to the stainless steel variety. Recently, Schmidt et al. [
17] replaced the normal plastic rails of hospital patients’ beds with copper and then tested for the microbial burden. It was found that the plastic surfaces on the control beds exceeded the recommended amount of bacterial concentrations, but it was not so on the copper beds (94% lower). Salgado et al. [
32] installed copper alloys on common touch surfaces in the hospital environment such as bed rails, overbed tables, intravenous poles, arms of visitor’s chairs, nurses’ call buttons, computer mouses, the bezel of the touch screen monitor, and palm rest of laptop computers in three intensive care units (ICU) of three large hospitals in the USA. A total of 650 randomly selected patients were observed in 16 ICU rooms, with eight copper alloy fitted and eight control rooms. The results showed that the MRSA and VRE concentrations were significantly lower (0.071 vs. 0.123;
p = 0.020) in the copper-alloy equipped ICUs compared to the standard ICUs [
31]. It was also noticed that placing copper alloy surfaces in the ICU rooms reduced the risk of HAI by more than half during the study period, and no HAI outbreak of epidemiologically important organisms occurred in copper-alloy equipped ICUs. A detailed study was conducted in another 16 ICU rooms (eight experimental rooms and eight control rooms) of three hospitals in the USA over 21 months, replacing the normal hand-touch steel surfaces with copper, and this study also found that copper materials at the hand-touch surfaces significantly reduced the microbial burden (698 vs. 6102 CFU per 100 cm
2, 88% reduction) [
57].
A three-year-long study was conducted in France in five extended care facilities, replacing the doorknobs and handrails with copper alloys. Around 1400 samples were collected and analysed and found that copper doorknobs and handrails revealed significantly less microbial burden (59% and 33% reduction, respectively) than the normal doorknobs and handrails [
65]. Other studies conducted in the health care environment have also reported the benefits of replacing plastic hospital beds with copper or copper alloys due to the significant reduction in the microbial burden [
66,
67,
68,
69]. However, the studies revealed that the contact-killing property increases with an increase in copper concentration, and a minimum of 60% copper concentration is required in alloys to get the best result [
16,
57,
70,
71,
72]. Souli et al. [
72] studied the antibacterial efficacy of two copper coatings (99% and 63% copper concentrations) on various multi-drug resistant Gram-negative pathogens responsible for nosocomial infections such as
E. coli,
Enterobacter spp.,
K. pneumonia,
P. aeruginosa, and
Acinetobacter baumannii (A. baumannii). They found that copper coatings worked against all strains of the above microbes, with those having greater than 99% copper concentration being able to kill the microbes below six hours (2 h for
A. baumannii, 3 h for
Enterobacter spp., 5 h for
K.
pneumoniae, and 6 hr for
P.
aeruginosa) [
72]. The contact-killing efficacy of copper surfaces on
Clostridium difficile (C. difficile) (a major cause of hospital-acquired infection globally) showed similar characteristics to alloys with higher copper concentrations (>70% copper), killing the
C. difficile (vegetative cells and spores) after 24–48 h [
73]. This microbial contact-killing efficacy of copper has also been found to be successfully applied in wound dressings (Figures 1–3 in [
50]).
Apart from the copper concentration, the biocidal efficacy of a surface depends on many other factors such as atmospheric temperature, humidity, length of exposure, microbial type, and concentration [
50]. It does seem that contact-killing capability remains high across all standard temperature ranges [
74,
75]. Noyce et al. [
76] studied the characteristics of copper alloys at 22 °C and 4 °C with MRSA and found that at 22 °C, all the three MRSA strains (10
7 MRSA, EMRSA-1, and EMRSA-16) were completely killed after 45, 60, and 90 min respectively, but it took six hours to completely eradicate these strains at 4 °C [
76]. Michels et al. [
75] observed a >6.4 log reduction of MRSA when the temperature was 35 °C and humidity was >90%, whereas it was a >6.1 log reduction when the temperature was reduced to 20 °C. It is also noted that the alloys with higher copper concentration (85% and above) were able to completely kill
E. coli bacteria at a lower temperature [
77]. Similar studies were conducted by Wilks et al. [
78,
79], who found that antibacterial properties exist at all temperatures but were superior when copper concentrations exceeded 85%. Testing for MRSA at 20 °C on four copper alloys—C19700 (99% Cu), C24000 (80% Cu and 20% Zn), C22000 (90% Cu and 10% Zn), and C77000 (55% Cu, 27% Sn, and 18% Ni)—showed that for C19700, there was a drop off within 75 min and for C22000, drop off was after 270 min. Both are considered to be more than 99% effective [
75]. In a similar investigation, Bleichert et al. [
80] looked at the biocidal effects of copper surfaces on bacterial and viral biothreat agents and revealed that cells of bacterial biothreat agents exposed to copper surfaces are inactivated within a few minutes. On the other hand, the cells on the control surface (stainless steel) showed a slower decline of the viable cells over time [
80].
Whilst most recent studies were in the hospital environment, Inkinen et al. [
81] decided to study the antibacterial efficacy of copper in different environmental settings such as retirement homes, kindergartens, and office buildings. Copper replaced traditional materials at the common touch surfaces (such as door handles, light switches, corridor handrails, closet touch surfaces, toilet flush buttons, floor drain lids, and toilet support rails). The study found that the copper surfaces had a lower bacterial load than the reference products and concluded that copper touch surfaces functioned efficiently as an antibacterial surface [
81]. It was found that
C. difficile can form spores and survive on dry surfaces for up to five months, and cannot be killed by hospital-grade disinfectants [
27]. However, copper, including its alloys with greater than 70% copper, can kill the
C. difficile, including the spores [
27]. The antimicrobial property of copper regarding
C. difficile was also studied by Wheeldon et al. [
82] in a clinical setting using carrier test methods against dormant and germinating spores and vegetative cells for three hours in the presence and absence of organic matter. It was found that within 30 min, the copper surface destroyed the vegetative cells and reduced the viability of spores exposed to germination within an hour, giving an additional positive signal for using copper in the hospital environment to reduce infection. Besides copper metal and alloys, a copper coating on a steel surface was also found to enhance the antibacterial property of the steel [
83].
In the food industry, most bacterial contamination is due to
E. coli O157 and is responsible for large-scale food recalls [
77]. Noyce et al. [
77] studied the efficacy of seven cast copper alloys with copper concentration ranges from 61% to 95% to investigate the ability to reduce
E. coli strains in the food industry environment. The study found that without the addition of beef extract, three alloys completely killed the
E. coli inoculum within six hours of exposure at 22 °C, but at a lower temperature (4 °C), only the copper alloys with higher copper concentration (>85%) were able to significantly reduce the inoculum [
77].
Listeria monocytogenes (L. monocytogenes), commonly found in soil, water, plant materials, and animals (including humans), are of considerable concern in the food industry [
79]. It has been recognised as a human pathogen since 1929, and records show that
Listeria infections affect around 2500 people every year in the US, causing 500 deaths annually [
79]. It can be critical to pregnant women, the elderly, and immunocompromised people [
84]. The bacteria cause Listeriosis, whose symptoms are often septicaemia, encephalitis, spinal meningitis, and corneal ulcers, including pneumonia, which is considered the cause of miscarriage and even death [
85,
86]. Aisha [
87] investigated copper alloys’ antimicrobial effect in killing
Listeria and found that copper ions are very effective. Wilks et al. [
79] also studied copper’s efficacy in killing
Listeria, and found no viable
Listeria on any copper alloys after 60 min (5 Log reduction), whereas viable cells were found on stainless steel even after 24 h. Furthermore, they reported that a new alloy called New Silver (65% Cu, 18% Ni, and 17% Zn) also inactivated all bacteria within 90 min of exposure. All these studies support the conclusion that copper products and surfaces can be effectively used in many locations, especially in the health industries and public places, to reduce the bacterial burden and subsequent diseases.
Even though many studies mentioned the influence of copper surfaces in reducing the microbial burden, a review by Cochrane conducted in Australia mentioned that there is only limited evidence available to support the use of environmental fittings with antimicrobial properties in preventing infections with multi-resistant bacterial organisms [
88].
1.2. Copper as an Antiviral Agent
The antiviral activity of copper was studied as early as 1958 by Bauer [
89], whose work was followed by many researchers who demonstrated the efficacy of copper against many viral strains [
1,
10,
15,
51]. Published studies (
Table 1 and
Table 2) confirmed the contact-killing property of copper surfaces against viruses such as influenza virus, norovirus, monkeypox, vaccinia virus, human immunodeficiency virus (HIV), SARS-CoV, and SARS-CoV-2 [
3,
10,
51,
89,
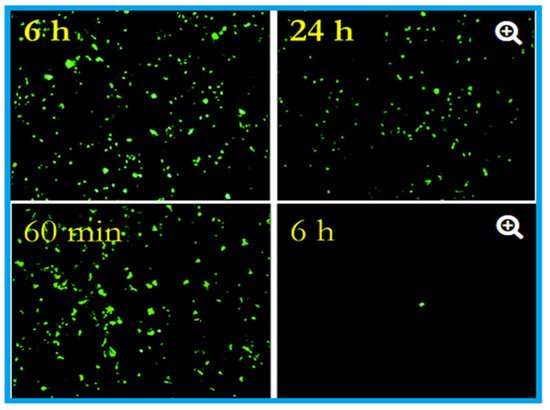
90]. Researchers at the University of Southampton showed that they could significantly prevent the spreading of influenza using copper surfaces, and it was further revealed that the influenza virus could be eradicated within six hours of exposure to a copper surface [
91]. These researchers placed two million active units of influenza A (H1N1) virus on a sheet of copper (C1100, which is pure copper under ISO standards) and stainless steel (S30400) (
Figure 1). After 24 h, the virus on the steel had declined to 500,000 units, but only 500 viruses were found to be active after six hours on the copper [
62,
91,
92].
Figure 1. Effects of influenza A virus on steel surface (top) and copper surface (bottom). The influenza virus was cultured in R-mix vials that contain a monolayer of mink lung and human laryngeal carcinoma cells grown on glass coverslips. This was inoculated into sterile coupons of copper (C11000) and steel (20 µL virus suspension with 10
8 virus particles per millilitre) for the experimental purpose and kept at room temperature (22 ± 2 °C) with a relative humidity of 50 to 60%. Here in the epifluorescent image, the number of green fluorescing cells are proportional to the viral inoculum. After six hours, 10
6 virus particles were found to be remained viable on the steel surface, and after 24 h, 5 × 10
5 particles were present, capable of causing cell infection (top). In contrast to the steel surface, on copper, the virus particles reduce to 5 × 10
5 after 60 min (the equivalent of 24 h of exposure on stainless steel), which reduced to 5 × 10
2 after six hours (nearly 4 log reduction). After 24 h of incubation, 500,000 virus particles were present on stainless steel, but 500 only seen after six hours on the copper surface. Adapted with permission from Ref. [
92]. Copyright 2007, American Society for Microbiology.
Warnes et al. [
93] tested the capability of inactivating one corona group virus, (229E), that can cause common colds and pneumonia. They found that the virus became inactivated immediately after being kept on copper, but it stayed viable for five days on stainless steel and glass (
Figure 2). Similar to bacteria, inoculation efficiency for the virus also depends on temperature, humidity, copper concentration [
3,
76,
77,
78,
93,
94,
95], length of exposure, and microbial density [
76,
78,
79,
96].
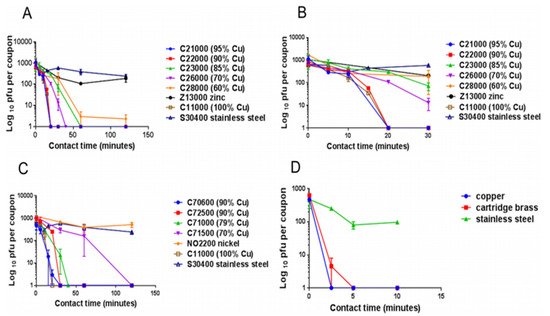
Figure 2. The panels describe the rapid contact-killing efficiency of various copper alloys (varies from 60% copper concentration to 100%) on human coronavirus-229E (HuCoV-229E), which causes the common cold. Initially, around 10
3 PFU HuCoV-229E (20 µL infected cell lysate) was applied on one sq. cm copper alloy coupon(s) with various copper concentrations, including stainless steel, nickel, and zinc (as control metals). (
A) It was found that the coronavirus was inactivated less than 40 min on brass coupons and less than 120 min on copper-nickel alloy (containing less than 70% copper). Surprisingly the alloy with 70% copper showed quick antiviral activity than the alloy with 85% copper. (
B) The observation showed an initial time lag on all alloys and metals, followed by rapid inactivation on copper coupons. The control metals stainless steel and nickel did not show any anti-coronavirus activity, except zinc, which showed little (significant only after 60 min,
p = 0.046). (
C) When the copper concentration was reduced to 70%, it took approximately 80 min more to inactivate all the viruses compared to one with 79% copper. (
D) When the same inoculum was applied at 1 µL per sq. cm, the coupons inactivated the virus eight-time faster. The experiment showed that the concentration of copper and the amount of virus are significant factors in showing the antiviral activity. Adapted from Ref. [
93].
Norovirus is highly infectious, causing viral gastroenteritis, and is spread through touch surfaces [
97]. Warnes and Keevil [
90] investigated the antiviral property of copper alloy surfaces against norovirus and found its effectiveness is proportional to the copper concentration in the alloy. Furthermore, they observed that antiviral effectiveness was not very rapid on brass but was very effective on the copper-nickel alloy. It is also found that copper-based filters inactivate HIV-1, which can significantly reduce HIV-1 infection through breastfeeding and blood donation [
98]. In addition to this, Noyce et al. [
92] indicated that copper surfaces act as a barrier against the avian flu epidemic. Their experiments have shown that, after six hours of exposure on a copper surface, 99.9% of the two million active H5N1 virus particles involved in the experiment became inactive.
Table 1. Biocidal activity of copper on various viruses.
| Types of Virus(es) |
Effect(s) |
Reference(s) |
| SARS-CoV-2 |
The virus was active only up to 4 h on the copper surface |
[51] |
| SARS-CoV |
The virus was active only up to 8 h on the copper surface |
[51] |
| Influenza A virus |
After incubation for six hours on copper 99% of the viral particles were inactivated |
[92] |
| Influenza A virus |
Solid-state copper oxide (Cu2O) inactivated the influenza A virus |
[99] |
Human coronavirus
HuCoV-229E |
Active only 20 min on copper surface |
[93] |
Hepatitis C virus
(HCV) |
Copper oxide-NPs significantly inhibit the infectivity of HCV, both at the entry and attachment stages |
[100] |
Murine norovirus-1
(MNV-1) |
Copper alloy (65 to 99.9% Cu) dry surfaces inactivated the MNV-1 |
[90] |
Vesicular Stomatitis Virus
Coxsackie Virus-B4
Respiratory Syncytial Virus |
Curcumin-copper synthesised compound found to effective against these viruses and could be utilised for the development of vaginal microbicidal gel |
[101] |
Feline Calicivirus
(FCV) |
CuI-NPs reduced the infectivity of FCV by order of seven magnitude |
[102] |
H1N1 Influenza Virus
2009 Pandemic |
CuI-NPs showed antiviral activity against influenza A virus of swine-origin |
[10] |
Human Immunodeficiency
Virus-1 (HIV-1) |
When exposed to copper oxide, the HIV-1 infectivity inhibited in a dose-dependant
manner |
[98] |
| Polio Virus |
Copper sulphate (20 mg/L) completely inactivated the polio virus in the presence of hydrogen peroxide |
[103] |
Herpes Simplex Virus
(HSV) |
Reducing agents such as ascorbic acid, hydrogen peroxide and cysteine enhanced the antiviral property of copper |
[104] |
1.3. Copper as an Antifungal Agent
The antifungal property of copper was first identified in 1761 when it was found that grain seeds soaked in copper sulphate solutions could inhibit the seed-borne fungi, but it took more than 100 years for the more sophisticated development of the fungicide “Bordeaux mixture” (developed by Pierre-Marie-Alexis Millardet and used in the USA) and “Burgundy mixture” (used in France) [
105]. Copper sulphate and lime mixtures were sprayed onto grape wines to make them mildew-free, prevent fungal infection in other plants, and control the algal growth in water reservoirs as well on timber, and were also found useful in preserving fabric [
105]. This experience again shows that even though the antimicrobial property of copper has been used in the agriculture sector for controlling fungal and bacterial infections for many years [
106,
107], it has come to the healthcare environment very lately.
A peer-reviewed study of the fungicidal property of copper was carried out in the 1950s, finding that copper, including copper compounds, are effective in killing several fungi and yeast, including
Candida albicans (C. albicans) [
108,
109],
Aspergillus niger (A. niger) [
107], and
Aspergillus carbonarious (A. carbonarious) [
110]. Indeed, many thousand tons of copper-based antifungal agents, specifically copper sulphate and copper hydroxide, are annually used across the globe for agricultural purposes [
111]. It is also used in wood processing to prevent roof moss formation and as an algae-resistant roofing system in the 3M industry. The biocidal efficacy of copper against
Aspergillus and
Fusarium species as well as
Penicillium chrysogenum (P. chrysogenum) and
C. albicans was studied by Weaver et al. [
9], who found that copper surfaces were able to kill most of these fungi and were able to prevent germination of new spores. The mechanism for control with bacteria and fungi is similar as inoculation starts with membrane damage, followed by enlargement and disappearance of vacuoles and the onset of oxidative stress.
Candida spp. can commonly survive in the healthcare environment and can cause HAIs [
112]. The efficacy of copper-sputtered polyester surfaces (Cu-PES) was tested against azole-resistant
C. albicans and
Candida glabrata (C. glabrata) under dark and low-intensity visible light, with the results showing that under low-intensity visible light, the Cu-PES exhibited fungicidal activity against both strains within 30 min of exposure [
112]. Of interest, it was found that, in addition to the pure copper surfaces, many copper compounds, such as the copper (II) complex of quinoline-2, could act as antifungal agents [
113]. Ghasemian et al. [
114] tested the antifungal efficiency of Cu-NPs against filamentous fungi (
Alternaria alternate (A. alternate), Aspergillus flavus (A. flavus), Fusarium solani (F. solani), and
P. chrysogenum) and found that Cu-NPs are very effective control agents, finding that particle size is a significant factor in antimicrobial activity. Two other studies also found that Cu-NPs are effective against
Candida species [
115,
116]. The contact-killing ability of copper for various microbes, including fungi, is summarised in
Table 2.
Table 2. Details of contact-killing or inactivation of microbes by copper surfaces. Adapted with permission from Ref. [
3]. Copyright 2007, American Society for Microbiology.
| Species |
Application Method
(Wet (W)/Dry (D)) |
Time to No Viable Forms Detected |
Reference(s) |
| SARS-CoV-2 |
D, 105.25 50% (TCID50) per mm |
4 h |
[51] |
| SARS-CoV |
D, 106.75–7.00 TCID50/mm |
8 h |
[51] |
| Human coronavirus—HCoV-229E |
W, 103 PFU |
20 min |
[93] |
| Influenza A virus (H1N1) |
W, 5 × 105 viruses h |
5 h |
[92] |
| Penicillium crysogenum |
W, (2–300) × 105 spores c |
24 h |
[9] |
| Fusarium solani |
W, (2–300) × 105 spores c |
24 h |
[9] |
| Fusarium oxysporum |
W, (2–300) × 105 spores c |
24 h |
[9] |
| Fusarium culmonium |
W, (2–300) × 105 spores c |
24 h |
[9] |
| Aspergillus niger |
W, (2–300) × 105 spores c |
>576 h |
[9] |
| Aspergillus fumigatus |
W, (2–300) × 105 spores c |
>120 h |
[9] |
| Aspergillus flavus |
W, (2–300) × 105 spores c |
120 h |
[9] |
| Candida albicans |
W, 105 CFU f |
1 h |
[59] |
| Saccharomyces cerevisiae |
D, 106 CFU k |
30 s |
[117] |
| Candida albicans |
D, 106 CFU k |
5 min |
[117] |
| Candida albicans |
W, (2–300) × 105 spores c |
24 h |
[118] |
| MRSA d |
W, 107 CFU f |
3 h |
[59] |
| MRSA NCTC 10442 |
W, 2 × 107 CFU |
75 min |
[75] |
| EMRSA-16 e (NCTC13143) |
W, (1–1.9) × 105 CFU c |
90 min |
[74] |
| EMRSA-1 e (NCTC11939) |
W, (1–1.9) × 107 CFU c |
1 h |
[74] |
| MRSA d (NCTC10442) |
W, (1–1.9) × 107 CFU c |
45 min |
[74] |
| Acinetobacter baumannii |
W, 107 CFU f |
3 h |
[59] |
| Pseudomonas aeruginosa |
W, 107 CFU f |
3 h |
[59] |
| Klebsiella pneumoniae |
W, 107 CFU f |
1 h |
[59] |
| Mycobacterium tuberculosis |
W, 2.5 × 107 CFU f |
5–15 days |
[59] |
| C. difficile (ATCC 9689) vc&spores |
W, 2.2 × 105 CFU c |
24–48 h |
[73] |
| Pseudomonas aeruginosa PAO1 |
W, 2.2 × 107 CFU j |
2 h |
[74] |
| Escherichia coli O157 |
W, 2.7 × 107 CFU c |
75 min |
[75] |
| Listeria monocytogenes Scott A |
W, 107 CFU c |
1 h |
[77] |
| Escherichia coli O157 |
W, (3–4) × 107 CFU c |
65 min |
[78] |
| Brucella melitensis NCTC 10094 |
D, 106 CFU k |
<5 min |
[80] |
| Burkholderia mallei NCTC 3709 |
D, 106 CFU k |
<5 min |
[80] |
| Burkholderia pseudomallei NCTC 0816-03 |
D, 106 CFU k |
<5 min |
[80] |
| Francisella tularensis FSC 237 |
D, 106 CFU k |
<5 min |
[80] |
| Yersinia pestis NCTC 2028 |
D, 106 CFU k |
<5 min |
[80] |
| C. difficile germinating spores |
W, 8 × 106 CFU i |
3 h |
[82] |
| C. difficile dormant spores |
W, 8 × 106 CFU i |
ua-3 h |
[82] |
| C. difficile NCTC11204/R20291 vc |
W, (1–5) × 106 CFU i |
30 min |
[82] |
| Different Enterococcus spp. |
W, 106 CFU f |
1 h |
[96] |
| Enterococcus hirae ATCC 9790 |
W, 107 CFU c |
90 min |
[96] |
| Escherichia coli W3110 |
D, 109 CFU k |
1 min |
[119] |
| Brachybacterium conglomeratum DSM10241 |
D, 109 CFU k |
A few min |
[119] |
| Staphylococcus warneri DSM 20316 |
D, 109 CFU k |
A few min |
[119] |
| Pseudomonas oleovorans DSM1045 |
D, 109 CFU k |
1 min |
[119] |
| Pantoea stewartii DSM30176 |
D, 109 CFU k |
1 min |
[119] |
| Acinetobacter johnsoni SM6963 |
D, 109 CFU k |
1 min |
[119] |
| Campylobacter jejuni |
W, 4.5 × 106 CFU b |
8 h |
[120] |
| Salmonella enterica |
W, 4.5 × 106 CFU b |
4 h |
[120] |