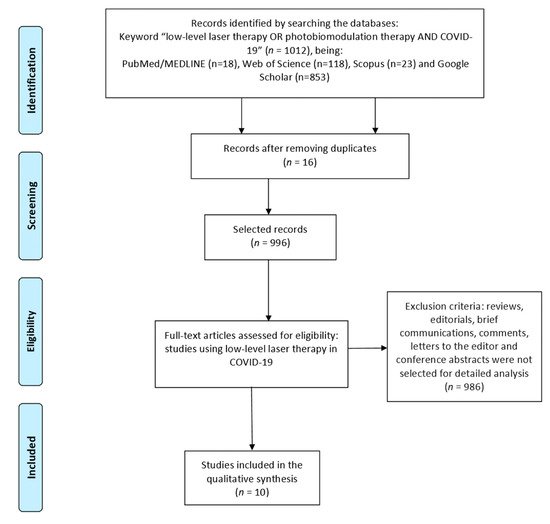
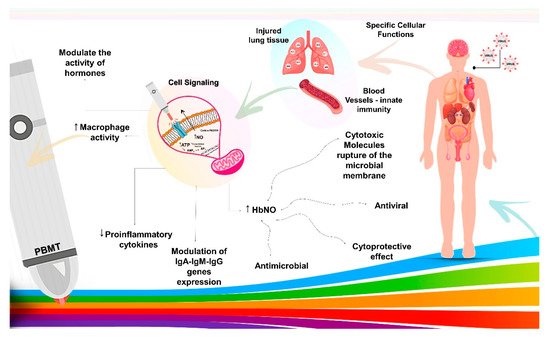
COVID-19 is a viral disease characterized as a pandemic by the World Health Organization in March 2020. Since then, researchers from all over the world have been looking for ways to fight this disease. Many cases of complications arise from insufficient immune responses due to low immunity, with intense release of pro-inflammatory cytokines that can damage the structure of organs such as the lung. Thus, the hypothesis arises that photobiomodulation therapy (PBMT) with the use of a low-level laser (LLLT) may be an ally approach to patients with COVID-19 since it is effective for increasing immunity, helping tissue repair, and reducing pro-inflammatory cytokines. This systematic entry was performed with the use of PubMed/MEDLINE, Web of Science, Scopus and Google Scholar databases with the following keywords: “low-level laser therapy OR photobiomodulation therapy AND COVID-19”.
- COVID-19
- SARS-CoV-2 infection
- immunity
- inflammation
- low-level laser therapy
- photobiomodulation therapy
- systematic review
1. Introduction
2. Selections of Study
3. Photobiomodulation Therapy as a Possible New Approach in COVID-19
This entry is adapted from the peer-reviewed paper 10.3390/life11060580
References
- Jiang, F.; Deng, L.; Zhang, L.; Cai, Y.; Cheung, C.W.; Xia, Z. Review of the Clinical Characteristics of Coronavirus Disease 2019 (COVID-19). J. Gen. Intern. Med. 2020, 2019, 1545–1549.
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020, 27, 1–4.
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J.; Sun, F.; et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496.
- Kulcsar, M.A.; Montenegro, F.L.; Arap, S.S.; Tavares, M.R.; Kowalski, L.P. High Risk of COVID-19 Infection for Head and Neck Surgeons. Int. Arch. Otorhinolaryngol. 2020, 24, e129–e130.
- Iser, B.P.M.; Silva, I.; Raymundo, V.T.; Poleto, M.B.; Schuelter-Trevisol, F.; Bobinski, F. Suspected COVID-19 case definition: A narrative review of the most frequent signs and symptoms among confirmed cases. Epidemiol. Serv. Saude 2020, 29, e2019354.
- Buchaim, R.L.; Barbalho, S.M.; Hamzé, A.L.; Goulart, R.d.A.; Rocha, K.T.P.; Reis, C.H.B.; Pilon, J.P.G.; Biteli, P.; Marinho, C.A.F.; Parra, M.C.G.; et al. Loss of smell and COVID-19: Anatomical and physiological considerations. Int. J. Adv. Eng. Res. Sci. 2020, 7, 278–280.
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374.
- Weyh, C.; Krüger, K.; Strasser, B. Physical activity and diet shape the immune system during aging. Nutrients 2020, 12, 622.
- Name, J.J.; Vasconcelos, A.R.; Souza, A.C.R.; Fávaro, W.J. Vitamin D, zinc and glutamine: Synergistic action with OncoTherad immunomodulator in interferon signaling and COVID-19 (Review). Int. J. Mol. Med. 2021, 47, 1–10.
- Mester, E.; Szende, B.; Gartner, P. The effect of laser beams on the growth of hair in mice. Radiobiol. Radiother. 1968, 9, 621–626.
- Anders, J.J.; Lanzafame, R.J.; Arany, P.R. Low-level light/laser therapy versus photobiomodulation therapy. Photomed. Laser Surg. 2015, 33, 183–184.
- Escudero, J.S.B.; Perez, M.G.B.; de Oliveira Rosso, M.P.; Buchaim, D.V.; Pomini, K.T.; Campos, L.M.G.; Audi, M.; Buchaim, R.L. Photobiomodulation therapy (PBMT) in bone repair: A systematic review. Injury 2019, 50, 1853–1867.
- Rosso, M.P.O.; Buchaim, D.V.; Kawano, N.; Furlanette, G.; Pomini, K.T.; Buchaim, R.L. Photobiomodulation therapy (PBMT) in peripheral nerve regeneration: A systematic review. Bioengineering 2018, 5, 44.
- Buchaim, D.V.; de Castro Rodrigues, A.; Buchaim, R.L.; Barraviera, B.; Junior, R.S.; Junior, G.M.; Bueno, C.R.; Roque, D.D.; Dias, D.V.; Dare, L.R.; et al. The new heterologous fibrin sealant in combination with low-level laser therapy (LLLT) in the repair of the buccal branch of the facial nerve. Lasers Med. Sci. 2016, 31, 965–972.
- Pomini, K.T.; Buchaim, D.V.; Andreo, J.C.; Rosso, M.P.O.; Della Coletta, B.B.; German, Í.J.S.; Biguetti, A.C.C.; Shinohara, A.L.; Rosa Júnior, G.M.; Cosin Shindo, J.V.T.; et al. Fibrin sealant derived from human plasma as a scaffold for bone grafts associated with photobiomodulation therapy. Int. J. Mol. Sci. 2019, 20, 1761.
- Buchaim, D.V.; Andreo, J.C.; Ferreira Junior, R.S.; Barraviera, B.; Rodrigues, A.C.; Macedo, M.C.; Rosa Junior, G.M.; Shinohara, A.L.; Santos German, I.J.; Pomini, K.T.; et al. Efficacy of Laser Photobiomodulation on Morphological and Functional Repair of the Facial Nerve. Photomed. Laser Surg. 2017, 35, 442–449.
- Rosso, M.P.O.; Rosa Júnior, G.M.; Buchaim, D.V.; German, I.J.S.; Pomini, K.T.; de Souza, R.G.; Pereira, M.; Favaretto Júnior, I.A.; Bueno, C.R.D.S.; Gonçalves, J.B.O.; et al. Stimulation of morphofunctional repair of the facial nerve with photobiomodulation, using the end-to-side technique or a new heterologous fibrin sealant. J. Photochem. Photobiol. B 2017, 175, 20–28.
- Buchaim, R.L.; Andreo, J.C.; Barraviera, B.; Ferreira Junior, R.S.; Buchaim, D.V.; Rosa Junior, G.M.; De Oliveira, A.L.; De Castro Rodrigues, A. Effect of low-level laser therapy (LLLT) on peripheral nerve regeneration using fibrin glue derived from snake venom. Injury 2015, 46, 655–660.
- De Oliveira Gonçalves, J.B.; Buchaim, D.V.; de Souza Bueno, C.R.; Pomini, K.T.; Barraviera, B.; Júnior, R.S.F.; Andreo, J.C.; de Castro Rodrigues, A.; Cestari, T.M.; Buchaim, R.L. Effects of low-level laser therapy on autogenous bone graft stabilized with a new heterologous fibrin sealant. J. Photochem. Photobiol. B 2016, 162, 663–668.
- Rosso, M.P.O.; Buchaim, D.V.; Pomini, K.T.; Coletta, B.B.D.; Reis, C.H.B.; Pilon, J.P.G.; Duarte Júnior, G.; Buchaim, R.L. Photobiomodulation therapy (PBMT) applied in bone reconstructive surgery using bovine bone grafts: A systematic review. Materials 2019, 12, 4051.
- Rosso, M.P.O.; Oyadomari, A.T.; Pomini, K.T.; Della Coletta, B.B.; Shindo, J.V.T.C.; Ferreira Júnior, R.S.; Barraviera, B.; Cassaro, C.V.; Buchaim, D.V.; de Bortoli Teixeira, D.; et al. Photobiomodulation Therapy Associated with Heterologous Fibrin Biopolymer and Bovine Bone Matrix Helps to Reconstruct Long Bones. Biomolecules 2020, 10, 383.
- Aimbire, F.; Ligeiro De Oliveira, A.P.; Albertini, R.; Corrêa, J.C.; Ladeira De Campos, C.B.; Lyon, J.P.; Silva, J.A.; Costa, M.S. Low level laser therapy (LLLT) decreases pulmonary microvascular leakage, neutrophil influx and IL-1β levels in airway and lung from rat subjected to LPS-induced inflammation. Inflammation 2008, 31, 189–197.
- Silva, V.R.; Marcondes, P.; Silva, M.; Villaverde, A.B.; Castro-Faria-Neto, H.C.; Vieira, R.P.; Aimbire, F.; de Oliveira, A.P.L. Low-level laser therapy inhibits bronchoconstriction, Th2 inflammation and airway remodeling in allergic asthma. Respir. Physiol. Neurobiol. 2014, 194, 37–48.
- De Lima, F.M.; Vitoretti, L.; Coelho, F.; Albertini, R.; Breithaupt-Faloppa, A.C.; De Lima, W.T.; Aimbire, F. Suppressive effect of low-level laser therapy on tracheal hyperresponsiveness and lung inflammation in rat subjected to intestinal ischemia and reperfusion. Lasers Med. Sci. 2013, 28, 551–564.
- Moraes, G.D.C.; Vitoretti, L.B.; De Brito, A.A.; Alves, C.E.; De Oliveira, N.C.R.; Dos Santos Dias, A.; Matos, Y.S.T.; Oliveira, M.C.; Oliveira, L.V.F.; Da Palma, R.K.; et al. Low-level laser therapy reduces lung inflammation in an experimental model of chronic obstructive pulmonary disease involving P2X7 receptor. Oxid. Med. Cell. Longev. 2018, 2018, 6798238.
- Tomé, R.F.F.; Silva, D.F.B.; dos Santos, C.A.O.; de Vasconcelos Neves, G.; Rolim, A.K.A.; de Castro Gomes, D.Q. ILIB (intravascular laser irradiation of blood) as an adjuvant therapy in the treatment of patients with chronic systemic diseases—An integrative literature review. Lasers Med. Sci. 2020, 35, 1899–1907.
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097.
- Hamblin, M.R. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys. 2017, 4, 337–361.
- Jahani-Sherafat, S.; Mokmeli, S.; Rostami-Nejad, M.; Razzaghi, Z.; Tavirani, M.R.; Razzaghi, M. The Effectiveness of Photobiomudulation Therapy (Pbmt) in Covid-19 Infection. J. Lasers Med. Sci. 2020, 11, S23–S29.
- Mokmeli, S.; Vetrici, M. Low level laser therapy as a modality to attenuate cytokine storm at multiple levels, enhance recovery, and reduce the use of ventilators in COVID-19. Can. J. Respir. Ther. 2020, 56, 25–31.
- Enwemeka, C.S.; Bumah, V.V.; Masson-Meyers, D.S. Light as a potential treatment for pandemic coronavirus infections: A perspective. J. Photochem. Photobiol. B Biol. 2020, 207, 111891.
- Hanna, R.; Dalvi, S.; Sălăgean, T.; Bordea, I.R.; Benedicenti, S. Phototherapy as a rational antioxidant treatment modality in covid-19 management; new concept and strategic approach: Critical review. Antioxidants 2020, 9, 875.
- Walski, T.; Drohomirecka, A.; Bujok, J.; Czerski, A.; Wąż, G.; Trochanowska-Pauk, N.; Gorczykowski, M.; Cichoń, R.; Komorowska, M. Low-Level Light Therapy Protects Red Blood Cells Against Oxidative Stress and Hemolysis During Extracorporeal Circulation. Front. Physiol. 2018, 9, 1–13.
- Razzaghi, M.; Kamani, E. Role Low-Power Blue Laser With a Wavelength of 405 Nm in Increasing the Level of Nitric Oxide in Increasing the Resistance of Cells to the Virus (COVID-19) and its Effect on Virus (COVID-19) Mortality in Vitro. OSP J. Case Rep. 2020, 2, JCR-2-118.
- De Lima, F.M.; Villaverde, A.B.; Albertini, R.; De Oliveira, A.P.L.; Neto, H.C.C.F.; Aimbire, F. Low-level laser therapy associated to N-acetylcysteine lowers macrophage inflammatory protein-2 (MIP-2) mRNA expression and generation of intracellular reactive oxygen species in alveolar macrophages. Photomed. Laser Surg. 2010, 28, 763–771.
- De Lima, F.M.; Albertini, R.; Dantas, Y.; Maia-Filho, A.L.; De Loura Santana, C.; Castro-Faria-Neto, H.C.; França, C.; Villaverde, A.B.; Aimbire, F. Low-level laser therapy restores the oxidative stress balance in acute lung injury induced by gut ischemia and reperfusion. Photochem. Photobiol. 2013, 89, 179–188.
- Nejatifard, M.; Asefi, S.; Jamali, R.; Hamblin, M.R.; Fekrazad, R. Probable positive effects of the photobiomodulation as an adjunctive treatment in COVID-19: A systematic review. Cytokine 2021, 137, 155312.
- Min, Y.K.; Yamamoto, T.; Kohda, E.; Ito, T.; Hamaguchi, H.O. 1064 nm near-infrared multichannel Raman spectroscopy of fresh human lung tissues. J. Raman Spectrosc. 2005, 36, 73–76.
- Wajih, N.; Alipour, E.; Rigal, F.; Zhu, J.; Perlegas, A.; Caudell, D.L.; Kim-Shapiro, D. Effects of nitrite and far-red light on coagulation. Nitric Oxide Biol. Chem. 2021, 107, 11–18.
- Kipshidze, N.; Yeo, N.; Kipshidze, N. Photodynamic therapy for COVID-19. Nat. Photonics 2020, 14, 651–652.
- De Mello Pinto, M.V.; Silva, C.H.M.B.; Sampaio, A.R.; Baron, M.V.; Sancho, A.G.; Fortuny, E.; Silva, L.F.A.; Picariello, F.; de Carvalho, R.M. Photodynamic Therapy with Phthalomethyl D: Perspectives against SARS-CoV-2. J. Biosci. Med. 2020, 8, 104–116.
- Schikora, D.; Hepburn, J.; Plavin, S.R.; Health, L. Reduction of the Viral Load by Non-Invasive Photodynamic Therapy in Early Stages of COVID-19 infection. Am. J. Virol. Dis. 2020, 2, 1–5.
- Svyatchenko, V.A.; Nikonov, S.D.; Mayorov, A.P.; Gelfond, M.L.; Loktev, V.B. Antiviral photodynamic therapy: Inactivation and inhibition of SARS-CoV-2 in vitro using methylene blue and Radachlorin. Photodiagn. Photodyn. Ther. 2021, 33, 102112.
- Kamani, E. Effect of Low Level Yellow Laser Light 589nm on Virus Prevention Corona Virus (COVID-19). OSP J. Case Rep. 2020, 2, 2–5.
- Ebadi, M.; Montano-Loza, A.J. Perspective: Improving vitamin D status in the management of COVID-19. Eur. J. Clin. Nutr. 2020, 74, 856–859.
- Pons, S.; Fodil, S.; Azoulay, E.; Zafrani, L. The vascular endothelium: The cornerstone of organ dysfunction in severe SARS-CoV-2 infection. Crit. Care 2020, 24, 4–11.
- Moskvin, S.; Askhadulin, E.; Kochetkov, A. Low-Level Laser Therapy in Prevention of the Development of Endothelial Dysfunction and Clinical Experience of Treatment and Rehabilitation of COVID-19 Patients. Rehabil. Res. Pract. 2021, 2021, 6626932.
- Moskvin, S.V.; Konchugova, T.V.; Khadartsev, A.A. The commonest therapeutic methods for laser irradiation of blood. Vopr. Kurortol. Fizioter. Lech. Fiz. Kult. 2017, 94, 10–17.
- Góralczyk, K.; Szymańska, J.; Szot, K.; Fisz, J.; Rość, D. Low-level laser irradiation effect on endothelial cells under conditions of hyperglycemia. Lasers Med. Sci. 2016, 31, 825–831.
- De Marchi, T.; Francio, F.; Ferlito, J.V.; Weigert, R.M.; de Oliveira, C.A.; Merlo, A.P.; Pandini, D.L.; Junior, B.A.P.; Giovanella, D.F.; Tomazoni, S.S.; et al. Effects of photobiomodulation therapy combined with static magnetic field (PBMT-sMF) in patients with severe COVID-19 requiring intubation a pragmatic randomized placebo-controlled trial. medRxiv 2020.
- Sigman, S.; Mokmeli, S.; Vetrici, M. Adjunct low level laser therapy (LLLT) in a morbidly obese patient with severe COVID-19 pneumonia: A case report. Can. J. Respir. Ther. 2020, 56, 52–56.
- Sigman, S.A.; Mokmeli, S.; Monici, M.; Vetrici, M.A. A 57-year-old african american man with severe COVID-19 pneumonia who responded to supportive photobiomodulation therapy (PBMT): First use of PBMT in COVID-19. Am. J. Case Rep. 2020, 21, 1–7.