Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Oncology
Lung cancer is a worldwide prevalent malignancy. This disease has a low survival rate due to diagnosis at a late stage challenged by the involvement of metastatic sites. Non-small-cell lung cancer (NSCLC) is presented in 85% of cases. The last decade has experienced substantial advancements in scientific research, leading to a novel targeted therapeutic approach. The newly developed pharmaceutical agents are aimed towards specific mutations, detected in individual patients inflicted by lung cancer. These drugs have longer and improved response rates compared to traditional chemotherapy.
- lung cancer
- non-small cell lung cancer
- gene alterations
- mutations
- targeted therapy
- pharmaceutical agents
- clinical trials
- response rate
- progression-free survival
- side effects
1. Introduction
Lung cancer (LC) is the most commonly diagnosed malignancy in the world, with more than 2 million new cases a year. It is the leading cause of death, responsible for approximately 19% of cancer-related deaths, more than breast, prostate and colon malignancies combined [1][2]. There are two major subtypes of LC, based on histology examination. Non-Small Cell Lung Cancer (NSCLC) is the most prevalent lung cancer subtype, accounting for 85% of cases. NSCLC is further histologically classified as non-squamous (70%) and squamous (25%). The remaining 15% are Small Cell Lung Cancer (SCLC) [3]. The majority of LC cases are diagnosed in an advanced stage, and thus have poor prognosis [4]. In recent years, a profound progression in the fields of diagnosing and treating LC has been achieved. In the field of diagnosis, the progress is attributed to our understanding of the molecular pathogenic pathways leading to this type of cancer, while in the field of treatment, the progress is related to the introduction of Immunotherapy and Biological treatments for patients with LC. While immunotherapy acts via augmenting the response of the immune system against cancer cells, the biological treatments promote their activity by blocking signal transduction pathways. The discovery of targetable genetic alterations has thoroughly shifted the treatment paradigm of metastatic lung cancer. This change has affected the means of drug administration, tailored to individual patients’ specific classification of tumor mutation, and thus improved response rates. Intravenous chemotherapeutic agents prescribed to all NSCLC patients, resulting in limited response rates (RR), have been replaced by targeted therapies. The latter are mostly orally administered, and are given to a specific group of patients, characterized by certain genetic alterations. These treatments provide profound and durable responses, expressed by longer progression-free survival (PFS) rates [5].
The paradigm shift is also true regarding the use of Immune Checkpoint Inhibitors (ICIs). While ICIs today serve as the backbone treatment of Stage IV LC with no targetable mutations, their use in the treatment plan of LC with driver mutation is controversial. Treating oncogenic-driven metastatic NSCLC with ICIs causes unacceptable toxicities before and after administering a Tyrosine Kinase Inhibitor (TKI) while yielding to only low to modest RRs in the first line setting [6].
2. Rare LC Mutations
2.1. ROS1 Gene
2.1.1. Description
ROS1 is a tyrosine-kinase receptor not normally expressed in the lung, and its role in humans is undefined [7]. Rearrangements in ROS1 gene happen in 1–2% of NSCLC, usually in females, younger patients, light smokers or non-smokers [8][9]. ROS1 gene mutations cause the dysregulation and constitutive activation of growth and survival pathways such as mitogen-activated protein kinase (MAPK), PI3K/AKT/mTOR pathway, and STAT3 [10][11]. Approximately 36% of treatment-naïve ROS1 LC patients are diagnosed with brain metastases [12].
2.1.2. Detection Methods
ROS1 gene rearrangements can be detected by fluorescence in situ hybridization (FISH), immunohistochemistry (IHC), polymerase chain reaction (PCR) and NGS.
2.1.3. Pharmaceutical Agents
Crizotinib, a tyrosine kinase inhibitor (TKI) was developed and used for ALK and MET alterations. It received approval by the FDA for treating ROS1-rearranged NSCLC patients, after Phase I study PROFILE 1001 showed a 72% overall response rate (ORR), 90% disease control rate (DCR), and 19.2 months of median PFS (mPFS) [13]. Even though, phase II studies showed more modest mPFS (10–15 months) results, Crizotinib was the standard of care for many years [14][15]. The December 2020 National Comprehensive Cancer Network (NCCN) guidelines recommend treating ROS1 rearranged NSCLC with Crizotinib, Ceritinib and Entrectinib as first-line therapies (Table 1).
Table 1. FDAapproved pharmaceutical agents to treat NSCLC gene alterations.
| Agent | Target | Approved for | Date |
|---|---|---|---|
| Ceritinib | ALK | ROS1 rearranged | 2014 |
| Crizotinib | ALK, MET | ROS1 rearranged, MET mutated | 2016 |
| Entrectinib | TRK, ROS, ALK | ROS1 rearranged, NTRK fused | 2019 |
| Dabrafenib | BRAF | BRAF mutated (In combination with trametinib) |
2015 |
| Trametinib | MEK1/2 | BRAF mutated (In combination with dabrafenib) |
2015 |
| Larotrectinib | NTRK | NTRK fused | 2018 |
| Capmatinib | MET | MET mutated | 2020 |
| Selpercatinib | RET | RET mutated | 2020 |
| Pralsetinib | RET | RET mutated | 2020 |
| Cabozantinib | VEGFR2, PDGFR, KIT | RET mutated | 2020 |
| Lorlatinib | ALK, ROS1 | ROS1 rearranged | 2018 |
Ceritinib, another potent ALK inhibitor, showed profound ORR (62%), DCR (81%) and mPFS (19.3 months) in a Korean phase II study. However, these results were demonstrated only in Crizotinib-naïve patients, thereby approving Ceritinib only as a first-line therapy [16].
Entrectinib, a TKI that selectively targets ROS1/ALK/NTRK, was shown to be more potent than Crizotinib in preclinical studies [17]. An analysis of several early studies showed substantial ORR (41%) and mPFS of 19 months. Entrectinib crosses the blood brain barrier (BBB) and has significant activity in the central nervous system (CNS) metastasis. Due to the fact that CNS is a common first site of progression in ROS1 NSCLC patients on Crizotinib, Entrectinib serves as an attractive option for second-line treatment [12][18]. One study showed that Entrectinib has 55% Intracranial ORR and more than 12 months duration of response. Patients without CNS metastasis had mPFS of 26 months [19].
Additional agents, although not yet recommended by NCCN, were investigated. Lorlatinib was studied on 69 ROS1 rearranged LC patients, showing ORR of 62% and mPFS of 21 months in Crizotinib-naïve patients. Additional advantages of Lorlatinib are its good intracranial activity and efficacy in pretreated patients. Lorlatinib had 64% intracranial ORR in Crizotinib-naïve and 50% in Crizotinib-treated patients. Since Crizotinib-refractory patients have limited treatment options, Lorlatinib potentially serves as an important next-line targeted agent [20]. Crizotinib has the lowest effect on intracranial disease due to its limited penetrance to the BBB, while Ceritinib, Entrectinib, and, as mentioned above, Lorlatinib, have good BBB penetrance and demonstrable intracranial efficacy.
No disease-limiting toxicities (DLTs) were reported for Crizotinib. However, the majority of treated patients suffered mild visual impairments.
All TKIs used to treat NSCLC ROS1 mutations cause gastrointestinal (GI) side effects. The highest incidence of symptoms was reported as a consequence of Ceritinib therapy (40%), while Lorlatinib and Entrectinib caused less frequent GI symptoms [21]. A specific adverse effect, occurring in 40% of Lorlatinib-treated patients, is peripheral neuropathy (Figure 1). NCCN guidelines recommend Lorlatinib and Entrectinib as second-line therapies (Table 1).
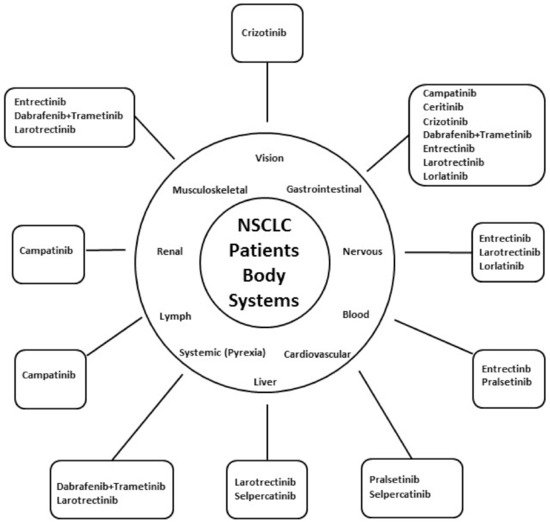
Figure 1. Common targeted therapies’ adverse events, categorized by systems. The figure shows the main targeted therapies causing adverse events in each of the main body systems. Clockwise: The main targeted therapy causing visual impairment is Crizotinib. Capmatinib, Ceritinib, Crizotinib, Dabrafenib + Trametinib, Entrectinib, Larotrectinib and Lorlatinib—cause Gastrointestinal adverse events. Entrectinib, Larotrectinib and Lorlatinib may cause neurological adverse events. Entrectinib and Pralsetinib are the most common causes of cytopenia. Pralsetinib and Selpercatinib could cause cardiovascular adverse events. The main causes of liver toxicity are Larotrectinib and Selpercatinib. Larotrectinib and the combination of Dabrafenib and Trametinib can cause Pyrexia. Capmatinib is the most common cause of lymphadenopathy. Capmatinib is the most common targeted therapy to cause renal toxicity. Entrectinib, Dabrafenib and trametinib and Larotrectinib may cause musculoskeletal adverse events.
2.1.4. Role of Immunotherapy
Very little is known about the effect of ICIs on ROS1-mutated NSCLC. Most of it is derived from the IMMUNOTARGET registry, which was created to retrospectively examine the real-world data of ICIs effect on targetable NSCLC tumors [22]. The use of monotherapy ICI resulted in 17% RR, but the cohort included only seven patients. Due to this limitation, no mPFS results could be retrieved. Twelve ROS1-mutated patients were treated by ICI and enrolled in a Korean study. They demonstrated 25% RR [23]. Some case reports indicated a certain efficacy of ICIs as advanced lines [24]. Due to the lack of reliable data and many effective targeted therapy options, we suggest treating ROS1-mutated NSCLC with targeted therapies, even in the advanced lines.
2.1.5. Mechanisms of Resistance
The main known mechanisms of drug resistance are associated with resistance to Crizotinib as a first-line therapy. The resistance may occur due to mutations in the ROS1 tyrosine kinase domain or due to the activation of factors in the signaling cascade [25]. The most common mutations are G2032R, D2033N, S1986Y/F, gatekeeper L2026M, and L1951R. As mentioned above, Lorlatinib has good activity in Crizotinib-refractory patients. Other agents known to have activity, although not used due to limited data or toxicities, are Cabozantinib and Repotrectinib [7].
2.2. RET Gene
2.2.1. Description
RET is a growth factor receptor of the glial cell line-derived neurotrophic factor receptor [26]. RET rearrangements/fusions incidence in NSCLC is 1–2%, resulting in independent homodimerization of the receptor and to constitutive kinase activity. These alterations differ from RET mutations, which are more common in Medullary thyroid cancer [27]. Alterations in RET usually occur in young females, light smokers and non-smokers [9][28].
2.2.2. Detection Methods
RET mutations are detected by FISH or NGS, but can also be detected by IHC, Reverse transcription PCR (RT-PCR) and circulating tumor-DNA (ctDNA) [29].
2.2.3. Pharmaceutical Agents
Primarily, RET-altered NSCLC were treated by drugs targeting multiple alterations (Cabozantinib, Lenvatinib, RXDX-105, etc.) [30][31][32], resulting in a modest responses and poor tolerability due to off-targeted activity. As a consequence, two drugs were specifically designed to target RET: BLU-667 (Pralsetinib), LOXO-292 (Selpercatinib). Studies were conducted using these two drugs, which were highly selective RET TKIs and have CNS activity [33][34].
Pralsetinib was studied in phase I/II study, ARROW, conducted on 114 patients. ORR was 57% in 87 patients previously treated with platinum-based chemotherapy, while 70% ORR was reported in 27 treatment-naïve patients. Pralsetinib can cause grade 3–4 neutropenia and hypertension. Of note, in the same trial, 7% of participants discontinued the treatment due to adverse events.
Selpercatinib was tested on 144 patients, demonstrating ORR of 64% in 105 previously treated patients and 85% in 39 treatment-naïve patients. Eleven patients with CNS metastasis had remarkable intracranial response—91% [35]. Selpercatinib may cause grade 3–4 transaminasitis and hypertension. Only 1.7% of patients discontinued treatment with this drug due to adverse events.
The NCCN guidelines recommend Selpercatinib, Pralsetinib, Cabozantinib and Vandetanib as 1st and advanced treatment lines in RET-mutated NSCLC (Table 1).
2.2.4. Role of Immunotherapy
According to a retrospective study which included 29 RET-altered NSCLC patients, ICIs have some activity on RET-rearranged NSCLC as an advanced treatment line. Of the 29 patients, 16 were treated with ICI and had shorter time-to-treatment discontinuation period compared to the 13 patients who were treated with Non-ICI treatment [36]. In the IMMUNOTARGET registry, one of the 16 patients with RET-rearranged NSCLC responded to ICI (16% RR with 2.1 months of mPFS). Other registry (GFPC 01-2018) showed 38% RR for ICI based on 9 RET-altered patients [37]. The majority of RET-altered patients in the registries mentioned above had surprisingly low PD-L1 expression rates, which may negatively influence the results. We suggest treating RET-altered NSCLC with targeted therapies and chemotherapy, especially taking into consideration the data showing the good activity of Pemetrexed-based chemotherapy in RET-altered NSCLC [38].
2.2.5. Mechanisms of Resistance
RET resistance could occur due to gatekeeper mutations or changes in the RAS/MAPK signaling pathway, such as mutations in NRAS, KRAS or MET amplification, EGFR overexpression and AXL overexpression [39]. There are at least fourteen known resistance mutations, resulting in different resistance profiles to multiple TKIs, with Nintedanib being the less affected TKI [40]. Lately, G810 solvent front mutation was described as a recurrent mechanism of resistance to selective RET inhibition with Selpercatinib [41][42].
2.3. BRAF Gene
2.3.1. Description
BRAF mutations promote cell proliferation and survival by phosphorylating and activating the MAPK/extracellular signal-regulated kinase (ERK) downstream signal pathways. BRAF Mutations are found in 1–5% of NSCLC [43][44], equally divided between V600 (Valine replaced by other amino acid at position 600) and non-V600 [45], with V600E (Glutamic acid replacing Valine) being the most common V600 mutation, which occurs at the level of T1799 transversion in exon 15. Non-V600E BRAF mutations may be either activating (i.e., G469A/V, K601E, L597R) or inactivating (i.e., D594G, G466V) [46]. The BRAF V600E mutation results in constitutive activation of the MAPK/ERK pathway, causing a 10-fold increase in BRAF activity [47]. According to previous evaluations, BRAF mutations in NSCLC were believed to be more prevalent in female patients. However, other evaluations did not statistically prove this observation [48]. BRAF mutations’ link to age and smoking status is also invariable [49][50].
2.3.2. Detection Methods
BRAF mutations can be detected by IHC, RT-PCR, Sanger sequencing and NGS.
2.3.3. Pharmaceutical Agents
Targeting BRAF-mutations gained impressive successes in other types of cancer, hereby shedding light on BRAF-mutated NSCLC. Unlike other targetable mutations, BRAF-mutated malignancies-focused therapy consists of addressing both the BRAF and the downstream MEK protein together. Former studies showed that targeting BRAF alone causes the development of upstream and downstream bypass pathways, such as RAS, MEK and ERK pathways and these, in turn, lead to resistance and decreased response to treatment [51][52].
A combination of Dabrafenib and Trametinib was studied in a Phase II study, recruiting 57 previously treated patients. The outcomes were 63% ORR and showed manageable safety profile [53]. Similar study was conducted on 36 treatment-naïve patients. The combination of Dabrafenib and Trametinib demonstrated 64% ORR and mPFS of 10.9 months [54] on treatment-naïve patients. This therapy combination reported side effects were pyrexia (in more than 30% of cases) and, less frequently, nausea, vomiting, diarrhea and asthenia.
The NCCN guidelines recommend a combination of Dabrafenib and Trametinib as first and subsequent lines of therapy for BRAF mutation (Table 1).
2.3.4. Role of Immunotherapy
The most valuable data we have, although retrospective and not necessarily positive, about the effect of ICI in oncogenic-driver-mutated NSCLC is in BRAF-mutated NSCLC. In addition to the IMMUNOTARGET and GFPC 01-2018 registries, retrospective studies from Israel, Italy and the United States evaluated the activity of ICIs on BRAF-mutated NSCLC tumors and reported RRs that range between 10% and 30% with 3 months of mPFS [55][56][57]. Results were better in smoking patients and in non-V600E mutated tumors. Overall, ICIs were shown to be a reasonable tool in the armamentarium of treating BRAF-mutated NSCLC. Due to the limited options of targeted drugs for BRAF-mutated NSCLC, we suggest using ICIs as a second-line treatment after progression on Anti-BRAF and Anti-MEK drugs.
2.3.5. Mechanisms of Resistance
Anti-BRAF drugs revolutionized the treatment paradigm in BRAF-mutated tumors, especially in Melanoma. Almost 50% of metastatic melanoma patients have BRAF-mutant tumors; treating these patients with Anti-BRAF drugs produces magnificent RRs of 50–60% but its Achilles heel is the short duration of treatment before resistance and progression. Several resistance mechanisms are known—expression of CRAF kinases, elevated expression of COT, BRAF V600E amplification, NRAS upregulation, aberrant splicing of BRAF, PTEN loss, persistent activation of insulin-like growth factor 1 receptor, platelet-derived growth factor receptor and EGFR [46]. Some of these resistance mechanisms can be avoided by combining anti-BRAF drugs with anti-MEK drugs. Although second-generation anti-BRAF drugs (such as PLX8394) showed some activity in resistant tumors [46][58], at present, there are no reliable second-generation drugs.
2.4. NTRK Gene
2.4.1. Description
NTRK are tyrosine kinase receptors, which play a physiologic role in the development of the nervous system [59]. The NTRK family genes (NTRK1, NTRK2, NTRK3) comprise of three transmembrane proteins (TRKA, TRKB, TRKC).
NTRK gene fusions in NSCLC were first identified in a study generating NGS tests on lung tumor samples [60]. Further studies revealed that NTRK fusions occur generally in fewer than 1% of NSCLC cases [61][62]. In contrast with other targetable driver mutations, NTRK-rearranged lung cancers are not limited to specific subgroups and are not associated with specific clinical characteristics. NTRK-rearrangements are described in the literature across different histology types, in all sexes, ages and smoking [63].
2.4.2. Detection Methods
NTRK fusions can be detected by IHC, FISH, RT-PCR and NGS.
2.4.3. Pharmaceutical Agents
Early phase clinical trials tested several TKIs as potential treatments for NTRK rearrangements. The most promising TKIs were shown to be Larotrectinib and Entrectinib.
Larotrectinib is a selective TRKA/B/C inhibitor, primarily tested in a Phase I study which enrolled 55 patients with different NTRK-rearranged tumor types, including four patients with NSCLC. The study reported 75% ORR and 80% DCR, granting Larotrectinib the FDA and European Medicine Agency (EMA) approval. Updated results from the expanded patient cohort of the same study (153 patients) confirmed the preliminary results demonstrating 79% ORR, and mPFS of 28 months [64].
Entrectinib inhibits TRKA/B/C and has inhibitory activity in ALK and ROS1 mutations. It was studied in several phase I/II trials including 74 NTRK-rearranged patients (13 NSCLC patients) which reported in an integrated analysis promising results of 63.5% ORR and 11.2 mPFS [65].
Both TKIs, Larotrectinib and Entrectinib, were shown to have potential CNS activity [66].
The most frequent reported side effects related to Larotrectinib were fatigue, elevated transaminases, constipation, dizziness, nausea and vomiting, diarrhea and pyrexia. Entrectinib most frequently causes dysgeusia, dizziness, constipation, diarrhea and fatigue. In 35% of cases, it caused grade 3–4 adverse events, with weight gain and neutropenia being the most common.
The NCCN guidelines recommend Larotrectinib and Entrectinib as first and subsequent lines of therapy in NTRK-fused NSCLC tumors (Table 1).
2.4.4. Role of Immunotherapy
The IMMUNOTARGET and GFPC 01-2018 registries did not enroll any patients with NTRK alterations. Some data suggest that NTRK-fused tumors are associated with relatively high PD-L1 expression levels and a high Tumor mutational burden, suggesting that these tumors may have a good response to immunotherapy [61]. On the other hand, NTRK-fused NSCLC tumors are known to co-exist with STK11 mutations, which seem to be associated with a poor response to ICIs in KRAS mutant disease [67]. To the best of our knowledge, at present, there are no reliable data proving the efficacy or any results of ICI treatment in NTRK-fused NSCLC tumors.
2.4.5. Mechanisms of Resistance
There are several known primary and acquired resistance mechanisms to TKIs targeting NTRK-altered tumors. According to one study, Ponatinib and Nintedanib could overcome a novel NTRK resistance mutation (G667C). Larotrectinib, Entrectinib, Ponatinib and Nintedanib failed to show activity against the G595R resistance mutation [68].
2.5. MET Gene
2.5.1. Description
MET is a hepatocyte growth factor receptor with tyrosine kinase activity [69]. Alterations in the MET signaling pathway have been widely described in carcinogenic processes in several solid tumor types, including NSCLC [70]. While previously treated NSCLC patients mainly harbor MET amplification, approximately 2–4% of NSCLC treatment-naïve patients harbor a skipping mutation in exon 14 of MET [71]. Unlike the other rare mutations described above, which are mainly present in nonsquamous histology, MET mutations are harbored in 2% of squamous cell carcinoma histology [72][73]. Differing from other mutations, the incidence of MET mutations is higher in elderly, non-smoking patients [74].
2.5.2. Detection Methods
MET mutations can be evaluated by differential MET exon expression, quantitative RT-PCR, RNA sequencing and NGS.
2.5.3. Pharmaceutical Agents
Preliminary studies have reported that MET-mutated NSCLC may respond to treatment with MET inhibitors. A multicenter retrospective analysis demonstrated improvement in overall survival when treating MET-mutated NSCLC with MET inhibitors [75].
At present, the NCCN recommend treating MET-mutated NSCLC with Crizotinib or Capmatinib (Table 1).
Profile 1001 study recruited 18 MET-mutated NSCLC patients and treated them with Crizotinib. The oral multi-TKI protocol treatment resulted in 44% ORR. A total of 33% of the 13 patients who had amplified c-MET, responded to treatment, most of them from the high-level amplification group [76][77].
Capmatinib, a highly selective c-MET inhibitor, was tested in phase I clinical trials. The outcomes obtained ORRs between 18% and 63% in c-MET positive, cMET IHC +3 and cMET overexpressed NSCLC [78]. A phase II study GEOMETRY mono-I tested Capmatinib in different patient populations. The ORR reached 40.6% and mPFS was 5.4 months in pretreated NSCLC patients; however, in treatment-naïve patients, ORR levels were 67.9%, resulting in mPFS of 9.7 months. Capmatinib was also shown to have more than 50% Intracranial ORR (7 out of 13 patients with brain metastasis) [79]. The most common adverse events of Capmatinib are peripheral edema, nausea, vomiting and increased creatinine level. In the trial mentioned previously, 67% of patients experienced grade 3–4 toxicity.
2.5.4. Role of Immunotherapy
The IMMUNOTARGET registry enrolled 36 patients with MET exon 14 skipping mutation and demonstrated 16% RR with 3.4 mPFS. A series including 24 patients who were treated with ICI as first or advanced lines showed similar results, with 17% RR and 1.9 months of mPFS [80]. The GFPC 01-2018 registry demonstrated better results, with 36% RR and 4.9 months of mPFS to 30 MET-mutated patients that were enrolled. A German study that enrolled patients with several oncogenic driver mutations concluded that patients with MET exon 14 skipping mutation responded well to therapy, with three out of eight patients partially responding and one patient with stable disease. One of the patients who partially responded had a long PFS of 115.2 weeks [81]. Another study described six MET-mutated patients with long and durable responses to ICI (18–49 months) [82]. Overall, MET exon 14 skipping mutations seem to respond well to ICI, and ICI should be a reasonable treatment strategy. These results need to be confirmed in prospective clinical trials.
2.5.5. Mechanisms of Resistance
Resistance could be acquired due to on-target or off-target mechanisms. On-target acquired mechanisms could be single or polyclonal and include mutations in codons H1094, G1163, L1195, D1228, Y1230 or high levels of amplification of the MET exon 14-mutant allele. Off-target mechanisms could occur due to amplifications in KRAS, MDM2, EGFR, CDK4, HER2, HER3, BRAF, PIK3CA, loss of PTEN and mutations in KRAS [83][84][85]. Two TKIs Merestinib and Glasetinib were recently shown to have activity after acquiring resistance to Crizotinib [83].
2.6. HER2 Gene
2.6.1. Description
Alterations in HER2 genes have been discovered in the carcinogenesis pathway of several cancers. Whereas overexpression is the most known alteration for its implication on breast and gastric cancers, affecting treatment and prognosis, mutations are more clinically relevant in the NSCLC carcinogenesis. HER2 overexpression and gene amplification are seen in NSCLC, but seem to have no clinical implication, besides indicating poorer prognostic outcomes [86][87]. HER2 mutations are present in 1–4% of NSCLC cases, mostly in never-smoking females [88][89].
2.6.2. Detection Methods
To detect HER2 overexpression or amplification, IHC and FISH are usually used, since these molecular essays are cheap and easy to perform, yet practical and precise. To detect HER2 exon 20 insert mutation, NGS is usually used.
2.6.3. Pharmaceutical Agents
Several studies evaluated the effect of TKIs and anti-HER2 antibodies to address HER2 alterations, without providing significant clinical outcomes. Single agents Afatinib, Dacomitinib, Lapatinib and Neratinib provided modest ORRs 0–15% in different studies involving HER2-mutated NSCLC patients [90][91][92]. Ado-Trastuzumab emtansine (T-DM1), an antibody–drug conjugate, provided ORR of 44% with 5 months mPFS in a basket trial [93]. Unfortunately, these results were not consistent in other trials studying T-DM1, and thus T-DM1 did not enter into practice. The activity of Pyrotinib, a pan-HER TKI, was addressed in a multi-center phase II trial including 60 patients, demonstrating promising ORR of 30% and 6.9 months of mPFS [94]. Recently, data from phase II ZENITH20 trial, which addresses Poziotinib in HER2-mutated NSCLC patients, were published, showing mPFS of 5.5 months and 27.8% ORR [95]. As of writing this paper (March 2021), treatment for HER2-mutated NSCLC is without established standard of care (Table 1).
2.6.4. Role of Immunotherapy
Twenty-nine patients with HER2-mutant lung tumors were enrolled in the IMMUNOTARGET registry. Treatment with ICI resulted in poor RR of 7.4% with 2.5 months of PFS. The GFPC 01-2018 registry included 23 HER2-mutated NSCLC patients who were treated by ICI and demonstrated 27.3% RR (six patients), with 2.2 months of PFS. A retrospective study from Memorial Sloan Kettering Cancer Center included 26 patients and showed 12% RR [96].
This entry is adapted from the peer-reviewed paper 10.3390/biomedicines9050534
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424.
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30.
- Cruz, C.S.D.; Tanoue, L.T.; Matthay, R.A. Lung Cancer: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2011, 32, 605–644.
- Cancer Statistics Review, 1975–2017—SEER Statistics. Available online: (accessed on 29 March 2021).
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.-W.; Ou, S.-H.I.; Pérol, M.; Dziadziuszko, R.; Rosell, R.; et al. Alectinib versus Crizotinib in Untreated ALK-Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 829–838.
- Schoenfeld, A.; Arbour, K.; Rizvi, H.; Iqbal, A.; Gadgeel, S.; Girshman, J.; Kris, M.; Riely, G.; Yu, H.; Hellmann, M. Severe immune-related adverse events are common with sequential PD-(L)1 blockade and osimertinib. Ann. Oncol. 2019, 30, 839–844.
- Lin, J.J.; Shaw, A.T. Recent Advances in Targeting ROS1 in Lung Cancer. J. Thorac. Oncol. 2017, 12, 1611–1625.
- Bergethon, K.; Shaw, A.T.; Ou, S.-H.I.; Katayama, R.; Lovly, C.M.; McDonald, N.T.; Massion, P.P.; Siwak-Tapp, C.; Gonzalez, A.; Fang, R.; et al. ROS1 Rearrangements Define a Unique Molecular Class of Lung Cancers. J. Clin. Oncol. 2012, 30, 863–870.
- Takeuchi, K.; Soda, M.; Togashi, Y.; Suzuki, R.; Sakata, S.; Hatano, S.; Asaka, R.; Hamanaka, W.; Ninomiya, H.; Uehara, H.; et al. RET, ROS1 and ALK fusions in lung cancer. Nat. Med. 2012, 18, 378–381.
- Zong, C.S.; Zeng, L.; Jiang, Y.; Sadowski, H.B.; Wang, L.-H. Stat3 Plays an Important Role in Oncogenic Ros- and Insulin-like Growth Factor I Receptor-induced Anchorage-independent Growth. J. Biol. Chem. 1998, 273, 28065–28072.
- Nguyen, K.T.; Zong, C.S.; Uttamsingh, S.; Sachdev, P.; Bhanot, M.; Le, M.-T.; Chan, J.L.-K.; Wang, L.-H. The Role of Phosphatidylinositol 3-Kinase, Rho Family GTPases, and STAT3 in Ros-induced Cell Transformation. J. Biol. Chem. 2002, 277, 11107–11115.
- Patil, T.; Smith, D.E.; Bunn, P.A.; Aisner, D.L.; Le, A.T.; Hancock, M.; Purcell, W.T.; Bowles, D.W.; Camidge, D.R.; Doebele, R.C. The Incidence of Brain Metastases in Stage IV ROS1-Rearranged Non–Small Cell Lung Cancer and Rate of Central Nervous System Progression on Crizotinib. J. Thorac. Oncol. 2018, 13, 1717–1726.
- Shaw, A.T.; Ou, S.-H.I.; Bang, Y.-J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-Rearranged Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2014, 371, 1963–1971.
- Wu, Y.-L.; Yang, J.C.-H.; Kim, D.-W.; Lu, S.; Zhou, J.; Seto, T.; Yang, J.-J.; Yamamoto, N.; Ahn, M.-J.; Takahashi, T.; et al. Phase II Study of Crizotinib in East Asian Patients With ROS1-Positive Advanced Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 1405–1411.
- Mazières, J.; Zalcman, G.; Crinò, L.; Biondani, P.; Barlesi, F.; Filleron, T.; Dingemans, A.-M.C.; Léna, H.; Monnet, I.; Rothschild, S.I.; et al. Crizotinib Therapy for Advanced Lung Adenocarcinoma and a ROS1 Rearrangement: Results From the EUROS1 Cohort. J. Clin. Oncol. 2015, 33, 992–999.
- Lim, S.M.; Kim, H.R.; Lee, J.-S.; Lee, K.H.; Lee, Y.-G.; Min, Y.J.; Cho, E.K.; Lee, S.S.; Kim, B.-S.; Choi, M.Y.; et al. Open-Label, Multicenter, Phase II Study of Ceritinib in Patients With Non–Small-Cell Lung Cancer Harboring ROS1 Rearrangement. J. Clin. Oncol. 2017, 35, 2613–2618.
- Rolfo, C.; Ruiz, R.; Giovannetti, E.; Gil-Bazo, I.; Russo, A.; Passiglia, F.; Giallombardo, M.; Peeters, M.; Raez, L. Entrectinib: A potent new TRK, ROS1, and ALK inhibitor. Expert Opin. Investig. Drugs 2015, 24, 1493–1500.
- Drilon, A.; Siena, S.; Dziadziuszko, R.; Barlesi, F.; Krebs, M.G.; Shaw, A.T.; de Braud, F.; Rolfo, C.; Ahn, M.-J.; Wolf, J.; et al. Entrectinib in ROS1 fusion-positive non-small-cell lung cancer: Integrated analysis of three phase 1–2 trials. Lancet Oncol. 2020, 21, 261–270.
- Barlesi, F.; Drilon, A.; De Braud, F.; Cho, B.; Ahn, M.; Siena, S.; Krebs, M.; Lin, C.; John, T.; Tan, D.; et al. Entrectinib in locally advanced or metastatic ROS1 fusion-positive non-small cell lung cancer (NSCLC): Integrated analysis of ALKA-372-001, STARTRK-1 and STARTRK-2. Ann. Oncol. 2019, 30, ii48–ii49.
- Shaw, A.T.; Solomon, B.J.; Chiari, R.; Riely, G.J.; Besse, B.; Soo, A.R.; Kao, S.; Lin, C.-C.; Bauer, T.M.; Clancy, J.S.; et al. Lorlatinib in advanced ROS1-positive non-small-cell lung cancer: A multicentre, open-label, single-arm, phase 1–2 trial. Lancet Oncol. 2019, 20, 1691–1701.
- Sehgal, K.; Patell, R.; Rangachari, D.; Costa, D.B. Targeting ROS1 rearrangements in non-small cell lung cancer with crizotinib and other kinase inhibitors. Transl. Cancer Res. 2018, 7, S779–S786.
- Mazieres, J.; Drilon, A.; Lusque, A.; Mhanna, L.; Cortot, A.; Mezquita, L.; Thai, A.; Mascaux, C.; Couraud, S.; Veillon, R.; et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: Results from the IMMUNOTARGET registry. Ann. Oncol. 2019, 30, 1321–1328.
- Park, S.; Ahn, B.-C.; Lim, S.W.; Sun, J.-M.; Kim, H.R.; Hong, M.H.; Lee, S.-H.; Ahn, J.S.; Park, K.; La Choi, Y.; et al. Characteristics and Outcome of ROS1-Positive Non–Small Cell Lung Cancer Patients in Routine Clinical Practice. J. Thorac. Oncol. 2018, 13, 1373–1382.
- Yue, D.; Qian, J.; Chen, Z.; Zhang, B.; Chen, P.; Zhang, L.; Li, J.; Zhang, H.; Wang, C. Short-term response to immune-chemotherapy and immune features of a ceritinib-resistant patient with ROS1-rearranged lung adenocarcinoma. J. Immunother. Cancer 2021, 9, e001967.
- Gainor, J.F.; Tseng, D.; Yoda, S.; Dagogo-Jack, I.; Friboulet, L.; Lin, J.J.; Hubbeling, H.G.; Dardaei, L.; Farago, A.F.; Schultz, K.R.; et al. Patterns of Metastatic Spread and Mechanisms of Resistance to Crizotinib in ROS1-Positive Non–Small-Cell Lung Cancer. JCO Precis. Oncol. 2017, 1, 1–13.
- Mulligan, L.M. GDNF and the RET Receptor in Cancer: New Insights and Therapeutic Potential. Front. Physiol. 2019, 9, 1873.
- Drosten, M.; Pützer, B.M. Mechanisms of Disease: Cancer targeting and the impact of oncogenic RET for medullary thyroid carcinoma therapy. Nat. Clin. Pract. Oncol. 2006, 3, 564–574.
- Kohno, T.; Ichikawa, H.; Totoki, Y.; Yasuda, K.; Hiramoto, M.; Nammo, T.; Sakamoto, H.; Tsuta, K.; Furuta, K.; Shimada, Y.; et al. KIF5B-RET fusions in lung adenocarcinoma. Nat. Med. 2012, 18, 375–377.
- Leighl, N.B.; Page, R.D.; Raymond, V.M.; Daniel, D.B.; Divers, S.G.; Reckamp, K.L.; Villalona-Calero, M.A.; Dix, D.; Odegaard, J.I.; Lanman, R.B.; et al. Clinical Utility of Comprehensive Cell-free DNA Analysis to Identify Genomic Biomarkers in Patients with Newly Diagnosed Metastatic Non–small Cell Lung Cancer. Clin. Cancer Res. 2019, 25, 4691–4700.
- Drilon, A.; Rekhtman, N.; Arcila, M.; Wang, L.; Ni, A.; Albano, M.; Van Voorthuysen, M.; Somwar, R.; Smith, R.S.; Montecalvo, J.; et al. Cabozantinib in patients with advanced RET -rearranged non-small-cell lung cancer: An open-label, single-centre, phase 2, single-arm trial. Lancet Oncol. 2016, 17, 1653–1660.
- Drilon, A.; Fu, S.; Patel, M.R.; Fakih, M.; Wang, D.; Olszanski, A.J.; Morgensztern, D.; Liu, S.V.; Cho, B.C.; Bazhenova, L.; et al. A Phase I/Ib Trial of the VEGFR-Sparing Multikinase RET Inhibitor RXDX-105. Cancer Discov. 2018, 9, 384–395.
- Hida, T.; Velcheti, V.; Reckamp, K.L.; Nokihara, H.; Sachdev, P.; Kubota, T.; Nakada, T.; Dutcus, C.E.; Ren, M.; Tamura, T. A phase 2 study of lenvatinib in patients with RET fusion-positive lung adenocarcinoma. Lung Cancer 2019, 138, 124–130.
- Subbiah, V.; Velcheti, V.; Tuch, B.; Ebata, K.; Busaidy, N.; Cabanillas, M.; Wirth, L.; Stock, S.; Smith, S.; Lauriault, V.; et al. Selective RET kinase inhibition for patients with RET-altered cancers. Ann. Oncol. 2018, 29, 1869–1876.
- Gainor, J.F.; Lee, D.H.; Curigliano, G.; Doebele, R.C.; Kim, D.-W.; Baik, C.S.; Tan, D.S.-W.; Lopes, G.; Gadgeel, S.M.; Cassier, P.A.; et al. Clinical activity and tolerability of BLU-667, a highly potent and selective RET inhibitor, in patients (pts) with advanced RET-fusion+ non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2019, 37, 9008.
- Drilon, A.; Oxnard, G.R.; Tan, D.S.; Loong, H.H.; Johnson, M.; Gainor, J.; McCoach, C.E.; Gautschi, O.; Besse, B.; Cho, B.C.; et al. Efficacy of Selpercatinib in RET Fusion–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 813–824.
- Hegde, A.; Andreev-Drakhlin, A.Y.; Roszik, J.; Huang, L.; Liu, S.; Hess, K.; Cabanillas, M.; Hu, M.I.; Busaidy, N.L.; Sherman, S.I.; et al. Responsiveness to immune checkpoint inhibitors versus other systemic therapies in RET-aberrant malignancies. ESMO Open 2020, 5, e000799.
- Guisier, F.; Dubos-Arvis, C.; Viñas, F.; Doubre, H.; Ricordel, C.; Ropert, S.; Janicot, H.; Bernardi, M.; Fournel, P.; Lamy, R.; et al. Efficacy and Safety of Anti–PD-1 Immunotherapy in Patients With Advanced NSCLC With BRAF, HER2, or MET Mutations or RET Translocation: GFPC 01-2018. J. Thorac. Oncol. 2020, 15, 628–636.
- Shen, T.; Pu, X.; Wang, L.; Yu, Z.; Li, J.; Zhang, Y.; Liang, X.; Chen, H.; Xu, C.; Song, Z.; et al. Association between RET Fusions and Efficacy of Pemetrexed-based Chemotherapy for Patients With Advanced NSCLC in China: A Multicenter Retrospective Study. Clin. Lung Cancer 2020, 21, e349–e354.
- Nelson-Taylor, S.K.; Le, A.T.; Yoo, M.; Schubert, L.; Mishall, K.M.; Doak, A.; Varella-Garcia, M.; Tan, A.-C.; Doebele, R.C. Resistance to RET-Inhibition in RET-Rearranged NSCLC Is Mediated By Reactivation of RAS/MAPK Signaling. Mol. Cancer Ther. 2017, 16, 1623–1633.
- Liu, X.; Shen, T.; Mooers, B.H.M.; Hilberg, F.; Wu, J. Drug resistance profiles of mutations in the RET kinase domain. Br. J. Pharmacol. 2018, 175, 3504–3515.
- Solomon, B.J.; Tan, L.; Lin, J.J.; Wong, S.Q.; Hollizeck, S.; Ebata, K.; Tuch, B.B.; Yoda, S.; Gainor, J.F.; Sequist, L.V.; et al. RET Solvent Front Mutations Mediate Acquired Resistance to Selective RET Inhibition in RET-Driven Malignancies. J. Thorac. Oncol. 2020, 15, 541–549.
- Lin, J.; Liu, S.; McCoach, C.; Zhu, V.; Tan, A.; Yoda, S.; Peterson, J.; Do, A.; Prutisto-Chang, K.; Dagogo-Jack, I.; et al. Mechanisms of resistance to selective RET tyrosine kinase inhibitors in RET fusion-positive non-small-cell lung cancer. Ann. Oncol. 2020, 31, 1725–1733.
- Ding, X.; Zhang, Z.; Jiang, T.; Li, X.; Zhao, C.; Su, B.; Zhou, C. Clinicopathologic characteristics and outcomes of Chinese patients with non-small-cell lung cancer andBRAFmutation. Cancer Med. 2017, 6, 555–562.
- Marchetti, A.; Felicioni, L.; Malatesta, S.; Sciarrotta, M.G.; Guetti, L.; Chella, A.; Viola, P.; Pullara, C.; Mucilli, F.; Buttitta, F. Clinical Features and Outcome of Patients With Non–Small-Cell Lung Cancer Harboring BRAF Mutations. J. Clin. Oncol. 2011, 29, 3574–3579.
- Planchard, D.; Kim, T.M.; Mazieres, J.; Quoix, E.; Riely, G.; Barlesi, F.; Souquet, P.-J.; Smit, E.F.; Groen, H.J.M.; Kelly, R.J.; et al. Dabrafenib in patients with BRAFV600E-positive advanced non-small-cell lung cancer: A single-arm, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 642–650.
- Baik, C.S.; Myall, N.J.; Wakelee, H.A. Targeting BRAF-Mutant Non-Small Cell Lung Cancer: From Molecular Profiling to Rationally Designed Therapy. Oncologist 2017, 22, 786–796.
- Roviello, G.; D’Angelo, A.; Sirico, M.; Pittacolo, M.; Conter, F.U.; Sobhani, N. Advances in anti-BRAF therapies for lung cancer. Investig. New Drugs 2021, 39, 879–890.
- Tissot, C.; Couraud, S.; Tanguy, R.; Bringuier, P.-P.; Girard, N.; Souquet, P.-J. Clinical characteristics and outcome of patients with lung cancer harboring BRAF mutations. Lung Cancer 2016, 91, 23–28.
- Cardarella, S.; Ogino, A.; Nishino, M.; Butaney, M.; Shen, J.; Lydon, C.; Yeap, B.Y.; Sholl, L.M.; Johnson, B.E.; Jänne, P.A. Clinical, Pathologic, and Biologic Features Associated with BRAF Mutations in Non–Small Cell Lung Cancer. Clin. Cancer Res. 2013, 19, 4532–4540.
- Cui, G.; Liu, D.; Li, W.; Fu, X.; Liang, Y.; Li, Y.; Shi, W.; Chen, X.; Zhao, S. A meta-analysis of the association between BRAF mutation and nonsmall cell lung cancer. Medicine 2017, 96, e6552.
- Johnson, D.B.; Menzies, A.M.; Zimmer, L.; Eroglu, Z.; Ye, F.; Zhao, S.; Rizos, H.; Sucker, A.; Scolyer, R.A.; Gutzmer, R.; et al. Acquired BRAF inhibitor resistance: A multicenter meta-analysis of the spectrum and frequencies, clinical behaviour, and phenotypic associations of resistance mechanisms. Eur. J. Cancer 2015, 51, 2792–2799.
- Marusiak, A.A.; Edwards, Z.C.; Hugo, W.; Trotter, E.W.; Girotti, M.R.; Stephenson, N.L.; Kong, X.; Gartside, M.G.; Fawdar, S.; Hudson, A.; et al. Mixed lineage kinases activate MEK independently of RAF to mediate resistance to RAF inhibitors. Nat. Commun. 2014, 5, 3901.
- Planchard, D.; Besse, B.; Groen, H.J.M.; Souquet, P.-J.; Quoix, E.; Baik, C.S.; Barlesi, F.; Kim, T.M.; Mazieres, J.; Novello, S.; et al. Dabrafenib plus trametinib in patients with previously treated BRAFV600E-mutant metastatic non-small cell lung cancer: An open-label, multicentre phase 2 trial. Lancet Oncol. 2016, 17, 984–993.
- Planchard, D.; Smit, E.F.; Groen, H.J.M.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M., Jr.; Zhang, P.; Mookerjee, B.; et al. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: An open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1307–1316.
- Dudnik, E.; Peled, N.; Nechushtan, H.; Wollner, M.; Onn, A.; Agbarya, A.; Moskovitz, M.; Keren, S.; Popovits-Hadari, N.; Urban, D.; et al. BRAF Mutant Lung Cancer: Programmed Death Ligand 1 Expression, Tumor Mutational Burden, Microsatellite Instability Status, and Response to Immune Check-Point Inhibitors. J. Thorac. Oncol. 2018, 13, 1128–1137.
- Rihawi, K.; Giannarelli, D.; Galetta, D.; Delmonte, A.; Giavarra, M.; Turci, D.; Garassino, M.; Tiseo, M.; Barbieri, F.; Panni, S.; et al. BRAF Mutant NSCLC and Immune Checkpoint Inhibitors: Results From a Real-World Experience. J. Thorac. Oncol. 2019, 14, e57–e59.
- Offin, M.; Pak, T.; Mondaca, S.; Montecalvo, J.; Rekhtman, N.; Halpenny, D.; Wu, S.; Kris, M.; Paik, P.; Riely, G.; et al. P1.04-39 Molecular Characteristics, Immunophenotype, and Immune Checkpoint Inhibitor Response in BRAF Non-V600 Mutant Lung Cancers. J. Thorac. Oncol. 2019, 14, S455.
- Okimoto, R.A.; Lin, L.; Olivas, V.; Chan, E.; Markegard, E.; Rymar, A.; Neel, D.; Chen, X.; Hemmati, G.; Bollag, G.; et al. Preclinical efficacy of a RAF inhibitor that evades paradoxical MAPK pathway activation in protein kinaseBRAF-mutant lung cancer. Proc. Natl. Acad. Sci. USA 2016, 113, 13456–13461.
- Passiglia, F.; Caparica, R.; Giovannetti, E.; Giallombardo, M.; Listi, A.; Diana, P.; Cirrincione, G.; Caglevic, C.; Raez, L.E.; Russo, A.; et al. The potential of neurotrophic tyrosine kinase (NTRK) inhibitors for treating lung cancer. Expert Opin. Investig. Drugs 2016, 25, 385–392.
- Vaishnavi, A.; Capelletti, M.; Le, A.T.; Kako, S.; Butaney, M.; Ercan, D.; Mahale, S.; Davies, K.D.; Aisner, D.L.; Pilling, A.B.; et al. Oncogenic and drug-sensitive NTRK1 rearrangements in lung cancer. Nat. Med. 2013, 19, 1469–1472.
- Gatalica, Z.; Xiu, J.; Swensen, J.; Vranic, S. Molecular characterization of cancers with NTRK gene fusions. Mod. Pathol. 2019, 32, 147–153.
- Xia, H.; Xue, X.; Ding, H.; Ou, Q.; Wu, X.; Nagasaka, M.; Shao, Y.W.; Hu, X.; Ou, S.-H.I. Evidence of NTRK1 Fusion as Resistance Mechanism to EGFR TKI in EGFR+ NSCLC: Results From a Large-Scale Survey of NTRK1 Fusions in Chinese Patients with Lung Cancer. Clin. Lung Cancer 2020, 21, 247–254.
- Farago, A.F.; Taylor, M.S.; Doebele, R.C.; Zhu, V.W.; Kummar, S.; Spira, A.I.; Boyle, T.A.; Haura, E.B.; Arcila, M.E.; Benayed, R.; et al. Clinicopathologic Features of Non–Small-Cell Lung Cancer Harboring an NTRK Gene Fusion. JCO Precis. Oncol. 2018, 2, 1–12.
- Hong, D.S.; DuBois, S.G.; Kummar, S.; Farago, A.F.; Albert, C.M.; Rohrberg, K.S.; van Tilburg, C.M.; Nagasubramanian, R.; Berlin, J.D.; Federman, N.; et al. Larotrectinib in patients with TRK fusion-positive solid tumours: A pooled analysis of three phase 1/2 clinical trials. Lancet Oncol. 2020, 21, 531–540.
- Rolfo, C.D.; De Braud, F.G.; Doebele, R.C.; Drilon, A.E.; Siena, S.; Patel, M.; Cho, B.C.; Liu, S.V.; Ahn, M.-J.; Chiu, C.-H.; et al. Efficacy and safety of entrectinib in patients (pts) with NTRK-fusion positive (NTRK-fp) solid tumors: An updated integrated analysis. J. Clin. Oncol. 2020, 38, 3605.
- Ziegler, D.S.; Wong, M.; Mayoh, C.; Kumar, A.; Tsoli, M.; Mould, E.; Tyrrell, V.; Khuong-Quang, D.-A.; Pinese, M.; Gayevskiy, V.; et al. Brief Report: Potent clinical and radiological response to larotrectinib in TRK fusion-driven high-grade glioma. Br. J. Cancer 2018, 119, 693–696.
- Skoulidis, F.; Goldberg, M.E.; Greenawalt, D.M.; Hellmann, M.D.; Awad, M.M.; Gainor, J.F.; Schrock, A.B.; Hartmaier, R.J.; Trabucco, S.E.; Gay, L.; et al. STK11/LKB1 Mutations and PD-1 Inhibitor Resistance in KRAS-Mutant Lung Adenocarcinoma. Cancer Discov. 2018, 8, 822–835.
- Fuse, M.J.; Okada, K.; Oh-Hara, T.; Ogura, H.; Fujita, N.; Katayama, R. Mechanisms of Resistance to NTRK Inhibitors and Therapeutic Strategies in NTRK1-Rearranged Cancers. Mol. Cancer Ther. 2017, 16, 2130–2143.
- Weir, B.A.; Woo, M.S.; Getz, G.; Perner, S.; Ding, L.; Beroukhim, R.; Lin, W.M.; Province, M.A.; Kraja, A.; Johnson, L.A.; et al. Characterizing the cancer genome in lung adenocarcinoma. Nat. Cell Biol. 2007, 450, 893–898.
- Liu, X.; Newton, R.C.; Scherle, P.A. Developing c-MET pathway inhibitors for cancer therapy: Progress and challenges. Trends Mol. Med. 2010, 16, 37–45.
- The Cancer Genome Atlas Research Network Comprehensive molecular profiling of lung adenocarcinoma. Nat. Cell Biol. 2014, 511, 543–550.
- Frampton, G.M.; Ali, S.M.; Rosenzweig, M.; Chmielecki, J.; Lu, X.; Bauer, T.M.; Akimov, M.; Bufill, J.A.; Lee, C.; Jentz, D.; et al. Activation of MET via Diverse Exon 14 Splicing Alterations Occurs in Multiple Tumor Types and Confers Clinical Sensitivity to MET Inhibitors. Cancer Discov. 2015, 5, 850–859.
- Schrock, A.B.; Frampton, G.M.; Suh, J.; Chalmers, Z.R.; Rosenzweig, M.; Erlich, R.L.; Halmos, B.; Goldman, J.; Forde, P.; Leuenberger, K.; et al. Characterization of 298 Patients with Lung Cancer Harboring MET Exon 14 Skipping Alterations. J. Thorac. Oncol. 2016, 11, 1493–1502.
- Awad, M.M.; Oxnard, G.R.; Jackman, D.M.; Savukoski, D.O.; Hall, D.; Shivdasani, P.; Heng, J.C.; Dahlberg, S.E.; Jänne, P.A.; Verma, S.; et al. MET Exon 14 Mutations in Non–Small-Cell Lung Cancer Are Associated With Advanced Age and Stage-Dependent MET Genomic Amplification and c-Met Overexpression. J. Clin. Oncol. 2016, 34, 721–730.
- Awad, M.M.; Leonardi, G.C.; Kravets, S.; Dahlberg, S.E.; Drilon, A.; Noonan, S.A.; Camidge, D.R.; Ou, S.-H.I.; Costa, D.B.; Gadgeel, S.M.; et al. Impact of MET inhibitors on survival among patients with non-small cell lung cancer harboring MET exon 14 mutations: A retrospective analysis. Lung Cancer 2019, 133, 96–102.
- Camidge, D.R.; Ou, S.-H.I.; Shapiro, G.; Otterson, G.A.; Villaruz, L.C.; Villalona-Calero, M.A.; Iafrate, A.J.; Varella-Garcia, M.; Dacic, S.; Cardarella, S.; et al. Efficacy and safety of crizotinib in patients with advanced c-MET-amplified non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2014, 32, 8001.
- Drilon, A.E.; Camidge, D.R.; Ou, S.-H.I.; Clark, J.W.; Socinski, M.A.; Weiss, J.; Riely, G.J.; Winter, M.; Wang, S.C.; Monti, K.; et al. Efficacy and safety of crizotinib in patients (pts) with advanced MET exon 14-altered non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2016, 34, 108.
- Schuler, M.; Berardi, R.; Lim, W.-T.; de Jonge, M.; Bauer, T.; Azaro, A.; Gottfried, M.; Han, J.-Y.; Lee, D.; Wollner, M.; et al. Molecular correlates of response to capmatinib in advanced non-small-cell lung cancer: Clinical and biomarker results from a phase I trial. Ann. Oncol. 2020, 31, 789–797.
- Wolf, J.; Seto, T.; Han, J.-Y.; Reguart, N.; Garon, E.B.; Groen, H.J.; Tan, D.S.; Hida, T.; de Jonge, M.; Orlov, S.V.; et al. Capmatinib inMETExon 14–Mutated orMET-Amplified Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 944–957.
- Sabari, J.; Leonardi, G.; Shu, C.; Umeton, R.; Montecalvo, J.; Ni, A.; Chen, R.; Dienstag, J.; Mrad, C.; Bergagnini, I.; et al. PD-L1 expression, tumor mutational burden, and response to immunotherapy in patients with MET exon 14 altered lung cancers. Ann. Oncol. 2018, 29, 2085–2091.
- Kauffmann-Guerrero, D.; Tufman, A.; Kahnert, K.; Bollmann, B.A.; Reu, S.; Syunyaeva, Z.; Schneider, C.; Manapov, F.; Huber, R.M.; Golpon, H. Response to Checkpoint Inhibition in Non-Small Cell Lung Cancer with Molecular Driver Alterations. Oncol. Res. Treat. 2020, 43, 289–298.
- Mayenga, M.; Assié, J.-B.; Monnet, I.; Massiani, M.-A.; Tabeze, L.; Friard, S.; Fraboulet, S.; Métivier, A.-C.; Chouaïd, C.; Zemoura, L.; et al. Durable responses to immunotherapy of non-small cell lung cancers harboring MET exon-14–skipping mutation: A series of 6 cases. Lung Cancer 2020, 150, 21–25.
- Recondo, G.; Bahcall, M.; Spurr, L.F.; Che, J.; Ricciuti, B.; Leonardi, G.C.; Lo, Y.-C.; Li, Y.Y.; Lamberti, G.; Nguyen, T.; et al. Molecular Mechanisms of Acquired Resistance to MET Tyrosine Kinase Inhibitors in Patients with MET Exon 14–Mutant NSCLC. Clin. Cancer Res. 2020, 26, 2615–2625.
- Shah, R.; Alex, D.; Xu, Z. MET Exon 14 Skipping Alterations in Non-small Cell Lung Carcinoma—Current Understanding and Therapeutic Advances. Oncol. Hematol. Rev. (US) 2021, 16, 100–110.
- Jamme, P.; Fernandes, M.; Copin, M.-C.; Descarpentries, C.; Escande, F.; Morabito, A.; Grégoire, V.; Jamme, M.; Baldacci, S.; Tulasne, D.; et al. Alterations in the PI3K Pathway Drive Resistance to MET Inhibitors in NSCLC Harboring MET Exon 14 Skipping Mutations. J. Thorac. Oncol. 2020, 15, 741–751.
- Liu, L.; Shao, X.; Gao, W.; Bai, J.; Wang, R.; Huang, P.; Yin, Y.; Liu, P.; Shu, Y. The Role of Human Epidermal Growth Factor Receptor 2 as a Prognostic Factor in Lung Cancer: A Meta-Analysis of Published Data. J. Thorac. Oncol. 2010, 5, 1922–1932.
- Li, B.T.; Ross, D.S.; Aisner, D.L.; Chaft, J.E.; Hsu, M.; Kako, S.L.; Kris, M.G.; Varella-Garcia, M.; Arcila, M.E. HER2 Amplification and HER2 Mutation Are Distinct Molecular Targets in Lung Cancers. J. Thorac. Oncol. 2016, 11, 414–419.
- Li, C.; Sun, Y.; Fang, R.; Han, X.; Luo, X.; Wang, R.; Pan, Y.; Hu, H.; Zhang, Y.; Pao, W.; et al. Lung Adenocarcinomas with HER2-Activating Mutations Are Associated with Distinct Clinical Features and HER2/EGFR Copy Number Gains. J. Thorac. Oncol. 2012, 7, 85–89.
- Pillai, R.N.; Behera, M.; Berry, L.D.; Rossi, M.R.; Kris, M.G.; Johnson, B.E.; Bunn, P.A.; Ramalingam, S.S.; Khuri, F.R. HER2 mutations in lung adenocarcinomas: A report from the Lung Cancer Mutation Consortium. Cancer 2017, 123, 4099–4105.
- Kris, M.G.; Camidge, D.R.; Giaccone, G.; Hida, T.; Li, B.T.; O’Connell, J.; Taylor, I.; Zhang, H.; Arcila, M.E.; Goldberg, Z.; et al. Targeting HER2 aberrations as actionable drivers in lung cancers: Phase II trial of the pan-HER tyrosine kinase inhibitor dacomitinib in patients with HER2-mutant or amplified tumors. Ann. Oncol. 2015, 26, 1421–1427.
- De Grève, J.; Moran, T.; Graas, M.-P.; Galdermans, D.; Vuylsteke, P.; Canon, J.-L.; Schallier, D.; Decoster, L.; Teugels, E.; Massey, D.; et al. Phase II study of afatinib, an irreversible ErbB family blocker, in demographically and genotypically defined lung adenocarcinoma. Lung Cancer 2015, 88, 63–69.
- Mazières, J.; Barlesi, F.; Filleron, T.; Besse, B.; Monnet, I.; Beau-Faller, M.; Peters, S.; Dansin, E.; Früh, M.; Pless, M.; et al. Lung cancer patients with HER2 mutations treated with chemotherapy and HER2-targeted drugs: Results from the European EUHER2 cohort. Ann. Oncol. 2016, 27, 281–286.
- Li, B.T.; Shen, R.; Buonocore, D.; Olah, Z.T.; Ni, A.; Ginsberg, M.S.; Ulaner, G.A.; Offin, M.; Feldman, D.; Hembrough, T.; et al. Ado-Trastuzumab Emtansine for Patients With HER2-Mutant Lung Cancers: Results from a Phase II Basket Trial. J. Clin. Oncol. 2018, 36, 2532–2537.
- Zhou, C.; Li, X.; Wang, Q.; Gao, G.; Zhang, Y.; Chen, J.; Shu, Y.; Hu, Y.; Fan, Y.; Fang, J.; et al. Pyrotinib in HER2-Mutant Advanced Lung Adenocarcinoma After Platinum-Based Chemotherapy: A Multicenter, Open-Label, Single-Arm, Phase II Study. J. Clin. Oncol. 2020, 38, 2753–2761.
- Socinski, M.; Cornelissen, R.; Garassino, M.; Clarke, J.; Tchekmedyian, N.; Molina, J.; Goldman, J.; Bhat, G.; Lebel, F.; Le, X. LBA60 ZENITH20, a multinational, multi-cohort phase II study of poziotinib in NSCLC patients with EGFR or HER2 exon 20 insertion mutations. Ann. Oncol. 2020, 31, S1188.
- Lai, W.-C.V.; Feldman, D.L.; Buonocore, D.J.; Brzostowski, E.B.; Rizvi, H.; Plodkowski, A.J.; Ni, A.; Sabari, J.K.; Offin, M.D.; Kris, M.G.; et al. PD-L1 expression, tumor mutation burden and response to immune checkpoint blockade in patients with HER2-mutant lung cancers. J. Clin. Oncol. 2018, 36, 9060.
This entry is offline, you can click here to edit this entry!