Prophylactic interventions for the prevention of allergic diseases differ depending on the timing and the stage in the ontogeny of the processes leading from sensitisation to clinical symptoms. They can be divided into primary, secondary and tertiary prophylaxis
- Allergy
- Allergic Diseases
- Developmental origins of allergy
- Prevention
- Microbiome
- Allergen immunotherapy
- Breast feeding
- Weaning diet
- Allergen avoidance
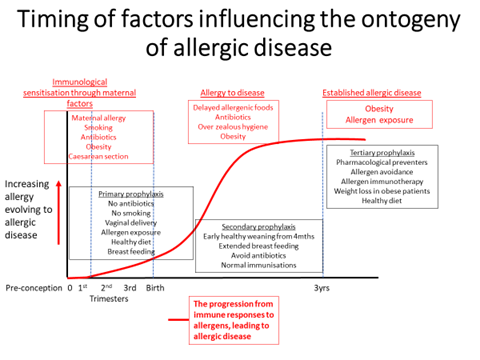
Figure: A diagramatic representation of the factors influencing the evolution of allergic sensitisation through to established allergic disease in relation to timing during early development. The red boxes list those factors increasing and the black boxes those decreasing risks of progression divided by timing into primary, secondary and tertiary prophylaxis.
Primary prophylaxis commences before raised IgE antibodies or positive allergy skin tests have been detected and is directed at what has become known as the first 1000 days from conception to the 2nd birthday.
There are interacting events which affect the relative risk of allergy development involving a subtle interaction between sub-types of helper lymphocytes. Those triggered to generate cytokines such as interferon gamma which are important for infection control are T-helper -1 (Th-1) cells. They suppress those associated with the evolution of allergy (Th-2) cells which in turn can suppress Th-1 activity. The decidual tissues around the foetus promote a Th-2 and T-regulatory environment through the generation of IL-4, IL-13, and Transforming Growth Factor beta (TGF-β). These are components of the mechanisms generating protection against a maternal Th-1 response to foeto-paternal antigens[1]. Absence of this regulation is associated with recurrent early miscarriage and intra-uterine growth retardation in both murine models and humans[2]. The foetus has the capacity to switch on adaptive immune responses to antigens via lymphoid accumulations in the small bowel from the middle of the 2nd trimester of pregnancy[3]. The foetus is exposed to the allergens that are in the mothers environment via passive transfer from her blood stream into amniotic fluid. When presented in association with Th-2 promoting cytokines through swallowed amniotic fluid in 2nd trimester this results in antigen presentation and allergy biased sensitisation in the foetal gut [4]. Consequently, all neonates have a Th-2 biased immune response which is more entrenched when the mother is also allergic[1][2]. A component of balancing the response occurs in 3rd trimester through allergen aggregated with IgG transported across the placenta which down-regulates sensitisation through inhibitory IgG receptors[5]. Balancing of Th-1 and Th-2 responses after delivery is affected by a rapidly diversifying ecological balance of organisms (microbiome) on the infant’s skin and in the respiratory and gastro-intestinal tracts. The microbiome associated with health (Eubiosis) is achieved by 2-3 years of age and is facilitated by pre-biotic oligosaccharides in human breast milk and a diverse healthy diet during weaning[6][7]. The symbiotic relationship with our microbiome results in facilitation of digestion, absorption, protection against pathogens, normal immunological and metabolic responses[8].
Several studies both in relation to food and inhalant allergy have indicated that early high exposure, from conception through the first months of life, may reduce the later risk of allergic sensitization and disease. During pregnancy levels of IgG-specific antibodies reflecting maternal exposure to food and inhalant allergens are actively transferred across the placenta from mother to foetus in the last trimester of pregnancy. High levels are associated with a lower risk of later allergic sensitization in infants. Neonatal cohort studies have demonstrated an inverse relationship between high cord blood IgG specific antibodies to egg, house mite and cat and subsequent allergy[5][9]. One observational study showed that children of mothers who received rye-grass allergen immunotherapy during pregnancy and consequently had high IgG antibody levels compared to children born to rye-grass allergic mothers not receiving immunotherapy showed fewer positive skin tests to rye-grass 3 – 12 years[10]. There is not a linear relationship between exposure and allergy. There is a bell-shaped curve, with low levels being insufficient to switch on a response, while high levels induce immune tolerance by creating anergy (non-immunological responsiveness) or deletion of sensitized T-lymphocytes. Intermediate exposure is more likely to be associated with sensitization and the evolution of allergic disease[2]. Based on immunological insights and observations from pregnancy and neonatal cohort studies, allergen avoidance has no place as a primary preventive strategy. High dose exposure is more likely achieve life-long tolerance of allergens. Until trials of this approach are completed the recommendation is to sustain a health, diverse and balanced diet and maternal environment throughout pregnancy.
The evolving skin, gut and airway microbiome has significant effects on the risks of allergic sensitisation. The seeding of organisms following exposure to mother’s gut microbiome during a normal delivery and subsequently in breast milk is pivotal in establishing eubiosis. The mothers’ diet, exposure to antibiotics and the mode of delivery all impact on outcomes. Caesarean section insulates the neonate from its mother’s gut microbiome, while antibiotic treatment during pregnancy and in the infant changes the microbiome leading to colonisation of the infant gut by different organisms which in turn leads to increase risks of food allergy, asthma and remarkably also obesity[11][12][13]. Thus, breast feeding, avoidance of pregnancy antibiotics and caesarean section; and a healthy weaning diet are essential pre-requisites to reducing risks of allergy. Breast feeding must be the first option for all infants, but if this is not possible trials of pre-biotic supplemented infant milk formulae have shown reduced prevalence of eczema at least over the first year of life[14].
Individual dietary constituents during pregnancy and lactation also have effects on outcomes. Various cohort studies have suggested that high fish, fresh fruit and vegetable intake is associated with less asthma in off-spring. The greatest beneficial effect is seen with the so-called Mediterranean diet[15][16]. Obesity in the mother increases the risk of a caesarean section delivery and with offspring obesity[13]. These factors in turn increase the risk of allergy and asthma[17].
Secondary prophylaxis is focused on those infants that are allergically sensitised but are yet to manifest allergic disease or have the first symptoms of allergy where there is potential to interrupt the allergic march from eczema and food allergy to inhalant allergy resulting in united airway disease (rhinitis/asthma).
The usual representation of the allergic march presents food allergy followed in succession by eczema, asthma and finally hay fever. The concept leads to the false impression that one condition leads inexorably to another. As our understanding of the genetic basis of eczema and asthma has increased it has become clear that there are independent influences on each. Nevertheless, there are mechanistic explanations for progression through the march for a proportion of subjects. The genetic basis for eczema is a defect in skin barrier function of which the best known is polymorphisms are in the gene coding for filaggrin. Defects in this protein lead to increased fluid losses from the epidermis and greater susceptibility to inflammation induced by irritants and micro-organisms, thereby leading to eczema[18]. The defect also renders the skin more susceptible to both food and inhalant allergen penetration into the dermis where antigen presenting cells can pick up allergen and migrate to regional lymphoid accumulations for sensitisation to occur[19]. Thus, the sequence of the march is incorrect with food allergy a consequence of the gene defect contributing to eczema and more likely to follow rather than precede it. Indeed, in the past peanut oils in topical preparations for the treatment of eczema have been implicated as initiating peanut allergy[20]. Inhalant allergy also evolves by the same route and increases the risk of rhinitis and asthma[19]. This could be viewed as a true march, though it may be better to view the overall allergic diseases associations as a complex stop/start dance, such as a tango[21].
Several trials have focused on interventions to interrupt the march. Early introduction of common allergenic foods during weaning from 4 months of age onwards in infants with eczema and/or food allergen sensitisation but without clinical reaction has been shown to appreciably reduce the later risk of clinical allergy to some but not all foods[22]. The principle is that oral exposures will induce tolerance and ideally this should be achieved before sensitisation has occurred through the skin or respiratory tract. Subcutaneous allergen immunotherapy administered to children with allergic rhinitis but no asthma has been shown to reduce the subsequent risk of new asthma onset and when given to those with only 1 allergen sensitisation are less likely to become allergic to new allergens[23][24].
The other discrepancy in the conventional representation of the march is that rhinitis is more likely to precede rather than follow the development of asthma. This is very clear in the evolution of occupational allergic airway disease. Sensitisation to an occupational allergen is followed by rhinitis and skin manifestations. Asthma develops after more sustained exposures. Provided avoidance is instituted early, asthma can be prevented or completely resolved. However, if exposure continues eventually asthma becomes entrenched and will continue even if the occupational allergen is avoided[25]. If this sequence occurs in allergic asthma, as is very likely, then early avoidance of the primary allergic trigger could have much greater benefit than has been achieved once asthma is established and has reached a chronic stage with structural remodeling changes to the airway wall. This approach requires more research trials. There appears to be a paradox with both early exposure and early avoidance recommended. However, avoiding respiratory tract exposure to inhaled allergen will reduce enhancement of the allergy and disease, while immunotherapy and high exposure by a different route can enhance regulatory T-cell activity and suppress allergic responses.
In relation to microbiome exposure (previously known as the hygiene hypothesis), there is evidence that early respiratory infections while increasing wheezing episodes in infancy are associated with less subsequent asthma. Families living on farms, drinking unpasteurised milk and being exposed to dogs and farm animals have less allergy and allergic diseases[26]. To what extent over-zealous hygiene increases risks remains to be established. However, the standard immunisations against the common pathogens, pertussis, diphtheria, tetanus, polio, haemophilus influenzae b, pneumococcus, menincoccus C, measles, mumps, rubella and for some BCG should proceed normally. If anything, the greater the number of immunisations administered the lesser the subsequent impact of eczema[27].
Tertiary prophylaxis addresses the management of established allergic disease. Aero-allergen exposure, in those who have rhinitis and/or asthma and are already allergically sensitized, induces immediate (within minutes) mast-cell degranulation, and thereby sneezing, rhinorrhoea, coughing and wheezing. In those with more severe disease, a late inflammatory reaction, dominated by first neutrophil and then eosinophil influx into airways, evolves three to four hours later. The immediate response is self-limiting and can be completely reversed by antihistamines for rhinitis and bronchodilators for asthma, while the late reaction is poorly anti-histamine/bronchodilator responsive and is only abrogated by prior treatment with inhaled (or oral/parenteral) cortico-steroids (ICS). The late reaction occurs more frequently in those with more severe airway disease[28][29]. This provides a basis for understanding the place of each medication in a therapeutic strategy. There is no evidence that any form of pharmacotherapy has primary or secondary prophylactic effects. Whether or not any of the new targeted biological agents will have any impact remains to be investigated. There is an impression that the earlier effective control of allergic disease is achieved the better the outcomes. However, evidence for this is at best equivocal.
Implicit to the knowledge that allergen exposure aggravates pre-existing allergic airway disease is the concept that allergen avoidance will be of benefit. However, many trials have failed to demonstrate consistent efficacy, particularly in relation to house dust mite (HDM) allergic asthma/rhinitis. This has led to Cochrane systematic reviews, reaching the conclusion that allergen avoidance has no place in therapeutic algorithms for asthma[30]. The difficulty is that exposures occur in many places, and strategies to reduce aero-allergen levels, whether to HDM, animals, pollens or moulds, have been insufficient. There is evidence that perfect avoidance, such as in high altitude environments, as in the Alps, can have considerable benefits[31]. Furthermore, recent trials of an effective environmental control system, based on temperature controlled laminar airflow, employed overnight, have shown significant improvements in quality of life and eosinophilic airway inflammation (represented by raised exhaled nitric oxide levels) in severe asthma in both children and adults[32][33]. While guidelines for asthma management have tended, mistakenly in my view, to consider allergen avoidance as secondary to pharmaco-therapy[34], those for rhinitis have given this approach a higher priority[35].
In patients with food allergy the standard practice is avoidance of the offending food(s) with treatment immediately available to deal with accidental exposures. This includes adrenalin (epinephrine) for potential anaphylaxis, and antihistamine for mild reaction. Avoidance diets have the potential to be nutritionally inadequate and it is difficult to achieve full avoidance. Food product labelling is often confusing and due to “may-contain” or related statements results in considerable restriction of choice[36]. Dietetic support is, therefore, a critical component of the management programme. Nutritional supplements may be required.
Obesity is associated with higher prevalence of asthma. The relationship is complex but based on Mendelian randomisation could well be causal[37]. Pro-inflammatory adipokines from fat cells increase inflammation thereby aggravating pre-existing airway inflammation. Weight loss in children with asthma has been associated with improved asthma control[38]. There is however, no evidence that any other dietary manipulation will have any impact[34]. Vitamin D has immune modulatory properties which theoretically should reduce susceptibility to inflammation. However, evidence from trials of dietary supplementation have not produced consistent evidence of benefit[39].
After allergen avoidance, allergen immunotherapy is the other specific approach to tertiary prophylaxis. It was first developed in 1911 for seasonal allergic rhinitis on the false assumption that pollen released a toxin causing the symptoms. Consequently, it was viewed as an infection which would improve with an immunisation strategy. Sequential injections of progressively increasing doses of a pollen extract were shown to reduce conjunctival challenge responses and improve symptoms through the pollen season[40][41]. At a time when there were no other effective treatments, immunotherapy became the mainstay of management. However, severe and very occasional fatal allergic reactions to the therapy inevitably occurred in some patients, most notably in those with severe asthma. Unfavourable comparisons with relatively safe pharmacotherapy for asthma and rhinitis relegated its use to severe insect venom allergy and seasonal allergic rhinitis alone. There is no doubting the efficacy of inhalant allergen immunotherapy in directly reducing allergic reactions and it is the only approach which modifies the natural history. Cochrane reviews have shown benefits in improving asthma symptoms, reducing treatment requirements and bronchial hyper-responsiveness[42]. It can interrupt the allergic march(23,24) and has a sustained effect following cessation of treatment after 3 years[43]. More recent developments of modified vaccines and different routes of administration (sub-lingual; intra-dermal) which retain immunogenicity but with reduced allergenicity have raised the potential for more extensive use in the future[44].
The immunotherapy approach has also been used in acute food allergy and has sometimes been labelled Systemic Oral Tolerance Induction (SOTI). The principle of administering progressively increasing doses of the allergen is similar for all allergen immunotherapy but hitherto has involved relatively unmodified food proteins with inevitable acute allergic reactions during treatment. The advent of allergen modification, co-administration of immune modulators and alternate routes of administration may make this approach more clinically acceptable. While for inhalant allergy 3 years of immunotherapy is enough, in the majority, to produce long-term benefits, as yet there is insufficient evidence to establish when true tolerance, with carry-over beyond the end of treatment, has been achieved for food allergy[45].
Conclusions
Knowledge about the ontogeny of allergic sensitisation and how it evolves into allergic disease has highlighted potential strategies for prevention. Prior to allergic sensitisation changes to the environment of the mother before and during pregnancy and lactation constitute primary prophylaxis. The optimised environment for the best infant outcomes includes avoidance of obesity, cigarette smoke, caesarean section delivery and antibiotics; a healthy balanced diet and breast feeding. Secondary prophylaxis commences with the first signs of allergy and includes early weaning onto common allergenic foods; extended breast feeding; normal immunisations; a healthy weaning diet; and avoidance of antibiotics unless clinically necessary. Tertiary prophylaxis after allergic disease has become manifest focuses on combinations of allergen avoidance; allergen immunotherapy; regular preventive pharmacotherapy; weight loss in obese subjects; and a healthy diet.
This entry is adapted from the peer-reviewed paper 10.3390/jcm9051483
References
- J Warner; The early life origins of asthma and related allergic disorders. Archives of Disease in Childhood 2004, 89, 97-102, 10.1136/adc.2002.013029.
- Warner J.O.. Developmental origins of asthma and related allergic disorders; Gluckman P., Hanson M., Eds.; Cambridge Univ: England, 2006; pp. 349–369 .
- Catherine A. Jones; Gillian H.S. Vance; Lynsey L. Power; Sylvia L.F. Pender; Thomas T. Macdonald; John O. Warner; Costimulatory molecules in the developing human gastrointestinal tract: A pathway for fetal allergen priming. Journal of Allergy and Clinical Immunology 2001, 108, 235-241, 10.1067/mai.2001.117178.
- Catherine A Jones; Jill A Warner; John O Warner; Fetal swallowing of IgE. The Lancet 1998, 351, 1859, 10.1016/s0140-6736(05)78805-x.
- Jenmalm, M.C. Björksten, B.; Cord blood levels of immune-globulin-G subclass antibodies to food and inhalant allergens in relation to maternal atopy and the development of atopic disease during the first 8 years of life. Clin. Exp. Allergy 2000, 30, 34-40, .
- Joel Dore; Hervé M. Blottière; The influence of diet on the gut microbiota and its consequences for health. Current Opinion in Biotechnology 2015, 32, 195-199, 10.1016/j.copbio.2015.01.002.
- Lieke Van Den Elsen; Johan Garssen; Remy Burcelin; Valerie Verhasselt; Shaping the Gut Microbiota by Breastfeeding: The Gateway to Allergy Prevention?. Frontiers in Pediatrics 2019, 7, 47, 10.3389/fped.2019.00047.
- Harm Wopereis; Raish Oozeer; Karen Knipping; Clara Belzer; Jan Knol; The first thousand days - intestinal microbiology of early life: establishing a symbiosis. Pediatric Allergy and Immunology 2014, 25, 428-438, 10.1111/pai.12232.
- G. H. S. Vance; Kate Grimshaw; R. Briggs; S. A. Lewis; M. A. Mullee; C. A. Thornton; J O Warner; Serum ovalbumin-specific immunoglobulin G responses during pregnancy reflect maternal intake of dietary egg and relate to the development of allergy in early infancy. Clinical & Experimental Allergy 2004, 34, 1855-1861, 10.1111/j.1365-2222.2004.02111.x.
- Glovsky, M,M. Ghekiere, L. Rejzek, E.; Effect of maternal immunotherapy on immediate skin test reactivity, specific Rye-1 IgG & IgE antibody and total IgE of the children. Ann. Allergy. 1991, 67, 21-24, .
- Niki Mitselou; Jenny Hallberg; Olof Stephansson; Catarina Almqvist; Erik Melén; Jonas F Ludvigsson; Cesarean delivery, preterm birth, and risk of food allergy: Nationwide Swedish cohort study of more than 1 million children. Journal of Allergy and Clinical Immunology 2018, 142, 1510-1514.e2, 10.1016/j.jaci.2018.06.044.
- Annemarie G. Hirsch; Jonathan Pollak; Thomas A. Glass; Melissa N. Poulsen; Lisa Bailey-Davis; Jacob Mowery; Brian S. Schwartz; Early-life antibiotic use and subsequent diagnosis of food allergy and allergic diseases.. Clinical & Experimental Allergy 2016, 47, 236-244, 10.1111/cea.12807.
- Noel T. Mueller; Guangyun Mao; W L Bennet; S K Hourigan; Maria Gloria Dominguez-Bello; Lawrence J. Appel; Xiaobin Wang; Does vaginal delivery mitigate or strengthen the intergenerational association of overweight and obesity? Findings from the Boston Birth Cohort.. International Journal of Obesity 2016, 41, 497-501, 10.1038/ijo.2016.219.
- Christoph Grüber; Margriet Van Stuijvenberg; Fabio Mosca; Guido Moro; Gaetano Chirico; Christian P. Braegger; Josef Riedler; Gunther Boehm; Ulrich Wahn; Reduced occurrence of early atopic dermatitis because of immunoactive prebiotics among low-atopy-risk infants. Journal of Allergy and Clinical Immunology 2010, 126, 791-797, 10.1016/j.jaci.2010.07.022.
- John O. Warner; Early life nutrition and allergy. Early Human Development 2007, 83, 777-783, 10.1016/j.earlhumdev.2007.09.005.
- Luis Garcia‐Marcos; Jose A. Castro‐Rodriguez Md; G. Weinmayr; D. B. Panagiotakos; K. N. Priftis; G. Nagel; Influence of Mediterranean diet on asthma in children: A systematic review and meta-analysis. Pediatric Allergy and Immunology 2013, 24, 330-338, 10.1111/pai.12071.
- P. Bager; J. Wohlfahrt; T. Westergaard; Caesarean delivery and risk of atopy and allergic disesase: meta-analyses. Clinical & Experimental Allergy 2008, 38, 634-642, 10.1111/j.1365-2222.2008.02939.x.
- Margaret Dennin; Peter A. Lio; Filaggrin and childhood eczema. Archives of Disease in Childhood 2017, 102, 1101-1102, 10.1136/archdischild-2017-313010.
- William H. I. McLean; Filaggrin failure – from ichthyosis vulgaris to atopic eczema and beyond. British Journal of Dermatology 2016, 175, 4-7, 10.1111/bjd.14997.
- Strid J, Hourihane J, Kimber I, Callard R, Strobel S.; Epicutaneous exposure to peanut protein prevents oral tolerance and enhances allergic sensitisation. Clin Exp Allergy 2005, 35, 757-766, .
- Levin M.E.; Warner J.O.; The Atopic Dance. Current Allergy and Clinical Immunology 2017, 30, 146-149, .
- Graham Roberts; Kate Grimshaw; K Kirsten Beyer; Robert Boyle; Gideon Lack; Moira Austin; Vanessa García-Larsen; Linus Grabenhenrich; Susanne Halken; Thomas Keil; et al. Can dietary strategies in early life prevent childhood food allergy? A report from two iFAAM workshops. Clinical & Experimental Allergy 2019, 49, 1567-1577, 10.1111/cea.13515.
- Jacobsen L., Niggemann B., Dreborg S., Ferdousi H.A., et al; Specific immunotherapy has long-term preventive effect of seasonaland perennial asthma: 10-year follow-up on the PAT study. Allergy 2007, 62, 943–948 , .
- G. B. Pajno; G. Barberio; L. Morabito; Fr. De Luca; S. Parmiani; Prevention of new sensitizations in asthmatic children monosensitized to house dust mite by specific immunotherapy. A six-year follow-up study.. Clinical & Experimental Allergy 2001, 31, 1392-1397, 10.1046/j.1365-2222.2001.01161.x.
- G. Moscato; Occupational Allergic Airway Disease. Current Otorhinolaryngology Reports 2017, 5, 220-228, 10.1007/s40136-017-0170-4.
- Diego G. Peroni; Giulia Nuzzi; Irene Trambusti; Maria Elisa Di Cicco; Pasquale Comberiati; Microbiome Composition and Its Impact on the Development of Allergic Diseases. Frontiers in Immunology 2020, 11, null, 10.3389/fimmu.2020.00700.
- C. Grüber; J. Warner; D. Hill; V. Bauchau; the EPAAC Study Group*; Early atopic disease and early childhood immunization - is there a link?. Allergy 2008, 63, 1464-1472, 10.1111/j.1398-9995.2008.01696.x.
- Warner J.O.; The significance of late reactions following bronchial challenge with house dust mite. Arch. Dis. Child 1976, 51, 905-911, .
- P O'byrne; Asthma pathogenesis and allergen-induced late responses.. Journal of Allergy and Clinical Immunology 1998, 102, S85–S89, .
- Peter C Gøtzsche; Helle Krogh Johansen; House dust mite control measures for asthma.. The Cochrane database of systematic reviews 2008, null, CD001187, 10.1002/14651858.CD001187.pub3.
- Diego G. Peroni; Attilio L. Boner; G Vallone; I Antolini; John O. Warner; Effective allergen avoidance at high altitude reduces allergen-induced bronchial hyperresponsiveness.. American Journal of Respiratory and Critical Care Medicine 1994, 149, 1442-1446, 10.1164/ajrccm.149.6.8004296.
- Robert J. Boyle; Christophe Pedroletti; Magnus Wickman; Leif Bjermer; Erkka Valovirta; Ronald Dahl; Andrea Von Berg; Olof Zetterström; John O. Warner; 4A Study Group; et al. Nocturnal temperature controlled laminar airflow for treating atopic asthma: a randomised controlled trial.. Thorax 2011, 67, 215-221, 10.1136/thoraxjnl-2011-200665.
- John O. Warner; Use of temperature-controlled laminar airflow in the management of atopic asthma: clinical evidence and experience. Therapeutic Advances in Respiratory Disease 2017, 11, 181-188, 10.1177/1753465817690505.
- British Thoracic Society/Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma. 2016
- Jan Brozek; Jean Bousquet; Carlos E Baena Cagnani; Sergio Bonini; G. Canonica; Thomas B. Casale; Roy Gerth Van Wijk; Ken Ohta; Torsten. Zuberbier; Holger Schünemann; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 Revision. Journal of Allergy and Clinical Immunology 2010, 126, 466-476, 10.1016/j.jaci.2010.06.047.
- L. Noimark; J. Gardner; J. O. Warner; Parents’ attitudes when purchasing products for children with nut allergy: A UK perspective. Pediatric Allergy and Immunology 2009, 20, 500-504, 10.1111/j.1399-3038.2008.00796.x.
- Yi-Qian Sun; Ben Michael Brumpton; Arnulf Langhammer; Yue Chen; Kirsti Kvaløy; Xiao-Mei Mai; Adiposity and asthma in adults: a bidirectional Mendelian randomisation analysis of The HUNT Study. Thorax 2019, 75, 202-208, 10.1136/thoraxjnl-2019-213678.
- M. E. Jensen; Peter Gibson; Clare Collins; J. M. Hilton; Lisa G. Wood; Diet-induced weight loss in obese children with asthma: a randomized controlled trial. Clinical & Experimental Allergy 2013, 43, 775-784, 10.1111/cea.12115.
- Beda Muehleisen; Richard L. Gallo; Vitamin D in allergic disease: Shedding light on a complex problem. Journal of Allergy and Clinical Immunology 2013, 131, 324-329, 10.1016/j.jaci.2012.12.1562.
- L. Noon; PROPHYLACTIC INOCULATION AGAINST HAY FEVER. The Lancet 1911, 177, 1572-1573, 10.1016/s0140-6736(00)78276-6.
- Freeman J.; Further observations on the treatment of hayfever by hypodermic innoculations of pollen vaccine. Lancet 1911, 2, 814-817, .
- Michael J. Abramson; Robert Puy; John M Weiner; Injection allergen immunotherapy for asthma. Cochrane Database of Systematic Reviews 2010, Issue 8, CD001186, 10.1002/14651858.cd001186.pub2.
- S R Durham; Samantha Walker; Eva-Maria Varga; Mikila Jacobson; Fiona O'brien; Wendy Noble; Stephen J Till; Qutayba A. Hamid; Kayhan T Nouri-Aria; Long-Term Clinical Efficacy of Grass-Pollen Immunotherapy. New England Journal of Medicine 1999, 341, 468-475, 10.1056/NEJM199908123410702.
- Oliver Pfaar; Ioana Agache; Frédéric De Blay; Sergio Bonini; Adam M. Chaker; Stephen R. Durham; Radoslaw Gawlik; Peter W. Hellings; Marek Jutel; Jörg Kleine-Tebbe; et al. Perspectives in allergen immunotherapy: 2019 and beyond.. Allergy 2019, 74, 3-25, 10.1111/all.14077.
- Feuille E., Nowak-Wegrzn A.; Allergen specific immunotherapeis for food allergy. Asthma Immunol. Res. 2018, 10, 189-206, .