Immunotherapy has emerged as a standard-of-care for most human malignancies, including head and neck cancer, but only a limited number of patients exhibit a durable clinical benefit. An urgent medical need is the establishment of accurate response predictors, which is handicapped by the growing body of molecular, cellular and clinical variables that modify the complex nature of an effective anti-tumor immune response.
- Head and Neck Cancer
1. Introduction
Head and neck cancers (HNCs) are among the most frequent and destructive human cancers worldwide, causing considerable morbidity and mortality [1][2]. Head and neck squamous cell carcinomas (HNSCCs) account for the majority of HNC, are unexpectedly heterogeneous in nature, and tobacco use, extensive alcohol consumption and infection with high-risk human papillomavirus (HPV), in particular HPV16, are the main etiological risk factors [3][4][5]. As for many other solid cancers, HNSCC pathogenesis resembles a tightly orchestrated balance between immune effector response and tolerance, and cancer cells evade the host immune surveillance by a broad range of cellular and molecular mechanisms [6][7][8]. Hence, the tumor immune microenvironment (TIME) of individual HNSCCs is rather heterogeneous and characterized by a broad spectrum of qualitative and quantitative differences in immune cell populations [9].
Despite continuous improvement in conventional treatments, consisting of surgery, radio- and chemotherapy, a substantial proportion of HNSCC patients suffer from locoregional relapse or distant metastasis [3][10]. For patients with recurrent or metastatic disease (R/M-HNSCC) the armamentarium of systemic anti-cancer modalities and innovative local approaches continues to grow, but the overall survival remains dismal and is still unsatisfactory [11][12]. In the past decade, immunotherapy based on immune checkpoint inhibition (ICI) has become an essential pillar for cancer treatment and now represents the standard of care for most human cancers, including HNSCC [3][13]. Activation of immune checkpoint cascades such as those controlled by cytotoxic T lymphcytes associated protein 4 (CTLA-4) or programmed cell death protein 1 (PD-1) and its ligand (PD-L1) results in inactivation of tumor-specific T cells and immune evasion. The underlying concept of ICI is that treatment with anti-PD-(L)1 or anti-CTLA-4 antibodies reinvigorates cytotoxic immune cells to target cancer cells [14][15][16].In randomized phase III trials two monoclonal antibodies (nivolumab and pembrolizumab), targeting PD-1 demonstrated longer overall survival in comparison with standard chemotherapy in pretreated R/M-HNSCC [17][18].Furthermore, pembrolizumab demonstrated superiority relative to standard first-line cytotoxic treatment for R/M-HNSCC, either as single-agent therapy or in combination with chemotherapy for tumors with PD-L1 expression [19].However, a major limitation is the low overall response rate of ICI therapy and many patients have experienced minimal or no clinical benefit [13][20]. Due to the relatively poor response rate, potential risk for hyper-progressive disease, and high degree of immune-related adverse events (irAEs), an urgent medical demand exists for reliable cellular or molecular biomarkers (Figure 1) to support treatment-decision making and a better stratification of cancer patients at higher risk for intrinsic or acquired treatment failure, who might benefit from new strategies of combination therapies [21][22].
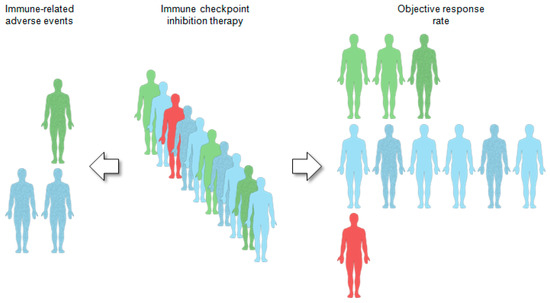
Figure 1. Companion diagnostics for immunotherapy by immune checkpoint inhibition. A limitation of immunotherapy by immune checkpoint inhibition (ICI) is the low response rate and only a small subset of head and neck cancer patients achieves a durable clinical benefit. Main challenge for molecular biomarkers is their predictive value not only to discriminate between responder (green patients) and non-responder (blue patients), but ideally also to assess the risk for a hyper-progressive disease (red patient) under ICI therapy. Establishment of biomarkers that enable early identification of patients at higher risk for severe immune-related adverse events (mottled patients) is another emerging research field of unmet medical need.
2. Immune-Related Mutational and Epigenetic Landscapes
TMB and high microsatellite instability are indirect measures of tumor antigenicity generated by somatic mutations (Figure 3). Somatic mutations in tumor DNA can induce neoantigens production, which can be targeted and recognized by the immune system, particularly after treatment with agents that activate T cells [23]. Those somatic mutations are transcribed and translated, and neoantigen-containing peptides are processed by the antigen-processing machinery and are loaded onto MHC molecules to be presented on the cell surface. However, not all somatic mutations produce peptides which are appropriately processed and loaded onto MHC complexes, and even fewer can be recognized by T cells [7][24][25]. Recent studies have revealed mutational signatures underlying the evolution of cancer and highlighted a strong association of HPV with APOBEC mutational signatures, suggesting impaired antiviral defense as a driving force in distinct cancers, including HNSCC [24][25][26]. Almost all HPV-positive and many HPV-negative HNSCCs share a large fraction of somatic mutations attributable to members of the apolipoprotein B mRNA editing enzyme catalytic subunit-like protein 3 (APOBEC3) family of single-stranded DNA cytosine deaminases [27][28]. Utilizing whole-exome and RNA-seq datasets from The Cancer Genome Atlas (TCGA), Faden et al. [29] observed the highest IFN-γ levels for HNSCC across cancer types with high APOBEC-related mutational burden. Most prominent IFN-γ scores in HNSCC were present in HPV-related tumors and tumor-specific neoantigens were significantly correlated with mutational burden attributed to APOBEC [29]. In another study, a subgroup of APOBEC-enriched, HPV-negative HNSCC with a distinct immunogenic phenotype was identified, which was characterized by higher T-cell inflammation, prominent immune checkpoint expression and enrichment of mutations in immune-evasion pathways [30].
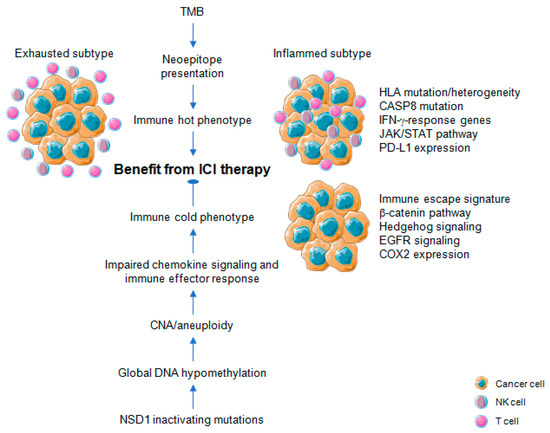
Figure 3. Association of molecular traits related to cancer immune phenotypes and efficacy of immune checkpoint inhibition therapy for head and neck cancer. Tumor mutational burden (TMB) is an indirect measure of tumor antigenicity generated by somatic mutations and neoepitope presentation, causing an immune hot phenotype. The immune hot phenotype emerges as either inflamed or exhausted subtype. An immune cold phenotype is characterized by impaired chemokine and immune effector response, accompanied by specific patterns of copy number alterations (CNA) or aneuploidy. Global DNA hypomethylation promotes chromosomal instability, particularly involving large-scale alterations leading to aneuploidy and has been observed in tumors with NSD1 inactivating mutations. Distinct molecular traits are associated with immune hot or cold phenotypes some of which serve as predictive markers for the efficacy of immune checkpoint inhibition (ICI) therapy.
In contrast to TMB, a high-level of aneuploidy also known as somatic copy number alterations (SCNAs) correlates with markers of immune evasion and with reduced response to immunotherapy (Figure 3). A higher burden of copy number loss in non-responders to CTLA-4 and PD-1 blockade was identified in a cohort of melanoma patients, which was associated with decreased expression of genes in immune-related pathways [31]. Davoli et al. [32] investigated 12 cancer types from TCGA to demonstrate that most highly aneuploid tumors exhibit reduced expression of markers for infiltrating immune cells, especially CD8-positive T cells and NK cells, indicating that aneuploidy restricts cytotoxic immune response during tumorigenesis. Again, tumor aneuploidy inversely correlates with patient survival in two clinical trials of ICI therapy for metastatic melanoma [32]. The effect on treatment response for TMB and aneuploidy was non-redundant, suggesting that both alterations reflect different aspects in the balance of immune surveillance versus tolerance and the potential utility of a combinatorial biomarker to optimize patient care with ICI therapy [31]. In line with this assumption, the combination of TMB and CNA for prognostic risk assessment and prediction of heterogeneous clinical responses to ICI treatment was confirmed for multiple cancers [33][34]. A high level of aneuploidy was also found for an immune cold subtype with least amount of tumor infiltrating lymphocytes (TILs) based on a pan-SCC cohort of TCGA [35]. For primary HNSCC, an inverse correlation between copy number alteration and measures of immune infiltration was evident [36][37], and a lower cytotoxic immune phenotype exhibited a characteristic pattern of copy number loss affecting chemokine signaling and immune effector response [38].
Profound global loss of DNA methylation is a hallmark of many cancers, and global demethylation in cancer promotes chromosomal instability [39][40], particularly involving large-scale alterations leading to aneuploidy [41]. Cancers commonly hijack various epigenetic mechanisms to escape immune restriction, but the impact of DNA methylation on immune evasion and in the context of cancer immunotherapy has been addressed only recently (Figure 3) [42][43][44]. In a pan-cancer analyses of TCGA data, Jung et al. [45] found that genomic hypomethylation correlated not only with aneuploidy but also immune escape signatures independently of the mutational burden, and was associated with increased immunotherapeutic resistance. Moreover, inactivating mutations in the nuclear receptor binding SET domain protein 1 (NSD1) a histone methyltransferase define an intrinsic subtype of HNSCC that features pronounced DNA hypomethylation [46][47][48] and displays an immune cold phenotype characterized by low levels of TILs and low expression of a CD8-positive T cell inflamed gene signature [49][50]. These data indicate NSD1 as a tumor cell-intrinsic driver of an immune cold phenotype by causing epigenetic deregulation with potential implications for immunotherapy (Figure 3).
Reactivation of transposable elements (TEs) including endogenous retroviral (ERV) transcripts is another consequence of profound global loss of DNA methylation in cancer. It results in a state of viral mimicry in which treated cancer cells mount an immune response by turning on viral defense genes and potentially expressing neoantigens [51]. In a pan-cancer analysis with TCGA cohorts, expression of 262 TE subfamilies appear to result from a proximal loss of DNA methylation [52]. TE overexpression in tumor samples with respect to matched normal controls is most prominent in stomach, bladder, and liver cancer as well as HNSCC. At the global level, this overexpression in HNSCC is associated with loss of DNA methylation, particularly at proximal CpG sites, suggesting targeted loss of DNA methylation near TE sites as a major mode of regulation [52]. For HNSCC, tumors with a high ERV expression pattern share prominent immune checkpoint pathway activation and increased immune infiltration with a higher CD8-positive T cell fraction as compared with ERV low expressing counterparts [53]. These data together with recent preclinical studies provide a strong rational for combining epigenetic targeting and immune checkpoint blockade in HNSCC to enhance treatment efficacy. Due to pleiotropic effects on multiple targets, which could limit the risk for treatment resistance, inhibition of epigenetic modifications emerges as promising strategy in combination with ICI [54]. Indeed, increased TE expression and de novo presentation of TE-derived peptides on MHC class I molecules were found upon treatment of cancer cells with a demethylation agent, indicating that therapeutic reactivation of tumor-specific TEs may synergize with immunotherapy. In line with this assumption, the phase IbNIBIT-M4 trial reported that treatment of patients with advanced melanoma using the next-generation DNA hypomethylating agent guadecitabine combined with ipilimumab is safe and tolerable, and shows promising immunomodulatory and antitumor activity [55].However, in an open-label phase II multi-cohort study administration of the oral DNA hypomethylating agent CC-486 combined with durvalumab did not demonstrate robust pharmacodynamic or clinical activity in selected immunologically cold solid tumors consisting of PD-(L)1 inhibitor naïve patients with either advanced microsatellite stable colorectal cancer, platinum resistant ovarian cancer, or estrogen receptor positive, HER2 negative breast cancer [56].
Enhancer of zeste homolog 2 (EZH2), a methyltransferase subunit of the polycomb repressive complex 2 (PRC2) that catalyzes histone H3 methylation on lysine 27 (H3K27), represents another epigenetic target to circumvent ICI resistance in HNSCC [57][58]. EZH2 expression was negatively correlated with components of the antigen-processing machinery pathway in TCGA-HNSC and genetic ablation or pharmacological inhibition of EZH2 resulted in a significant increase of MHC class I expression on HNSCC cells, antigen-specific CD8-positive T cell proliferation, IFN-γ production, and tumor cell cytotoxicity. In a preclinical mouse model, the combination of an EZH2 inhibitor (GSK126) and anti-PD1 antibodies suppressed tumor growth of anti-PD-1-resistant HNSCC [58]. The association of chromatin modification with CD8-positive T cell exclusion in HPV-negative HNSCC was further supported by a study of Vougiouklakis et al. [59]. They identified a couple of protein methyltransferases (PMTs) and demethylases (PDMTs) with inverse expression pattern compared to components of the antigen presentation machinery, CD8-positive T cells and immune-active chemokines. Finally, a phase II trial of pembrolizumab and vorinostat, a pan-HDAC (histone deacetylase) inhibitor, with progressing and incurable head and neck cancers demonstrated activity in R/M-HNSCC, but fewer responses in salivary gland cancer [60]. However, toxicities were higher than reported with pembrolizumab alone and no complete responder was observed.
This entry is adapted from the peer-reviewed paper 10.3390/cancers13051162
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424.
- Bosetti, C.; Carioli, G.; Santucci, C.; Bertuccio, P.; Gallus, S.; Garavello, W.; Negri, E.; La Vecchia, C. Global trends in oral and pharyngeal cancer incidence and mortality. Int. J. Cancer 2020, 147, 1040–1049.
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92.
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The molecular landscape of head and neck cancer. Nat. Rev. Cancer 2018, 18, 269–282.
- Jou, A.; Hess, J. Epidemiology and Molecular Biology of Head and Neck Cancer. Oncol. Res. Treat. 2017, 40, 328–332.
- Ferris, R.L. Immunology and Immunotherapy of Head and Neck Cancer. J. Clin. Oncol. 2015, 33, 3293–3304.
- Chen, D.S.; Mellman, I. Elements of cancer immunity and the cancer-immune set point. Nature 2017, 541, 321–330.
- Oliva, M.; Spreafico, A.; Taberna, M.; Alemany, L.; Coburn, B.; Mesia, R.; Siu, L.L. Immune biomarkers of response to immune-checkpoint inhibitors in head and neck squamous cell carcinoma. Ann. Oncol. 2019, 30, 57–67.
- Cillo, A.R.; Kurten, C.H.L.; Tabib, T.; Qi, Z.; Onkar, S.; Wang, T.; Liu, A.; Duvvuri, U.; Kim, S.; Soose, R.J.; et al. Immune Landscape of Viral- and Carcinogen-Driven Head and Neck Cancer. Immunity 2020, 52, 183–199 e189.
- Hess, J. Predictive Factors for Outcome and Quality of Life in HPV-Positive and HPV-Negative HNSCC. Recent Results Cancer Res. 2017, 206, 233–242.
- Szturz, P.; Vermorken, J.B. Management of recurrent and metastatic oral cavity cancer: Raising the bar a step higher. Oral Oncol. 2020, 101, 104492.
- Ringash, J. Survivorship and Quality of Life in Head and Neck Cancer. J. Clin. Oncol. 2015, 33, 3322–3327.
- Cohen, E.E.W.; Bell, R.B.; Bifulco, C.B.; Burtness, B.; Gillison, M.L.; Harrington, K.J.; Le, Q.T.; Lee, N.Y.; Leidner, R.; Lewis, R.L.; et al. The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of squamous cell carcinoma of the head and neck (HNSCC). J. Immunother. Cancer 2019, 7, 184.
- Fritz, J.M.; Lenardo, M.J. Development of immune checkpoint therapy for cancer. J. Exp. Med. 2019, 216, 1244–1254.
- Wei, S.C.; Duffy, C.R.; Allison, J.P. Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov. 2018, 8, 1069–1086.
- Sanmamed, M.F.; Chen, L. A Paradigm Shift in Cancer Immunotherapy: From Enhancement to Normalization. Cell 2018, 175, 313–326.
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867.
- Cohen, E.E.W.; Soulieres, D.; Le Tourneau, C.; Dinis, J.; Licitra, L.; Ahn, M.J.; Soria, A.; Machiels, J.P.; Mach, N.; Mehra, R.; et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): A randomised, open-label, phase 3 study. Lancet 2019, 393, 156–167.
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulieres, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Baste, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928.
- Hirsch, L.; Zitvogel, L.; Eggermont, A.; Marabelle, A. PD-Loma: A cancer entity with a shared sensitivity to the PD-1/PD-L1 pathway blockade. Br. J. Cancer 2019, 120, 3–5.
- Ribas, A.; Wolchok, J.D. Cancer immunotherapy using checkpoint blockade. Science 2018, 359, 1350–1355.
- Martins, F.; Sofiya, L.; Sykiotis, G.P.; Lamine, F.; Maillard, M.; Fraga, M.; Shabafrouz, K.; Ribi, C.; Cairoli, A.; Guex-Crosier, Y.; et al. Adverse effects of immune-checkpoint inhibitors: Epidemiology, management and surveillance. Nat. Rev. Clin. Oncol. 2019, 16, 563–580.
- Chan, T.A.; Yarchoan, M.; Jaffee, E.; Swanton, C.; Quezada, S.A.; Stenzinger, A.; Peters, S. Development of tumor mutation burden as an immunotherapy biomarker: Utility for the oncology clinic. Ann. Oncol. 2019, 30, 44–56.
- Alexandrov, L.B.; Kim, J.; Haradhvala, N.J.; Huang, M.N.; Tian Ng, A.W.; Wu, Y.; Boot, A.; Covington, K.R.; Gordenin, D.A.; Bergstrom, E.N.; et al. The repertoire of mutational signatures in human cancer. Nature 2020, 578, 94–101.
- Zapatka, M.; Borozan, I.; Brewer, D.S.; Iskar, M.; Grundhoff, A.; Alawi, M.; Desai, N.; Sultmann, H.; Moch, H.; Pathogens, P.; et al. The landscape of viral associations in human cancers. Nat. Genet. 2020, 52, 320–330.
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Borresen-Dale, A.L.; et al. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421.
- Cannataro, V.L.; Gaffney, S.G.; Sasaki, T.; Issaeva, N.; Grewal, N.K.S.; Grandis, J.R.; Yarbrough, W.G.; Burtness, B.; Anderson, K.S.; Townsend, J.P. APOBEC-induced mutations and their cancer effect size in head and neck squamous cell carcinoma. Oncogene 2019, 38, 3475–3487.
- Plath, M.; Gass, J.; Hlevnjak, M.; Li, Q.; Feng, B.; Hostench, X.P.; Bieg, M.; Schroeder, L.; Holzinger, D.; Zapatka, M.; et al. Unraveling most abundant mutational signatures in head and neck cancer. Int. J. Cancer 2021, 148, 115–127.
- Faden, D.L.; Ding, F.; Lin, Y.; Zhai, S.; Kuo, F.; Chan, T.A.; Morris, L.G.; Ferris, R.L. APOBEC mutagenesis is tightly linked to the immune landscape and immunotherapy biomarkers in head and neck squamous cell carcinoma. Oral Oncol. 2019, 96, 140–147.
- Messerschmidt, C.; Obermayer, B.; Klinghammer, K.; Ochsenreither, S.; Treue, D.; Stenzinger, A.; Glimm, H.; Frohling, S.; Kindler, T.; Brandts, C.H.; et al. Distinct immune evasion in APOBEC-enriched, HPV-negative HNSCC. Int. J. Cancer 2020, 147, 2293–2302.
- Roh, W.; Chen, P.L.; Reuben, A.; Spencer, C.N.; Prieto, P.A.; Miller, J.P.; Gopalakrishnan, V.; Wang, F.; Cooper, Z.A.; Reddy, S.M.; et al. Integrated molecular analysis of tumor biopsies on sequential CTLA-4 and PD-1 blockade reveals markers of response and resistance. Sci. Transl. Med. 2017, 9, eaah3560.
- Davoli, T.; Uno, H.; Wooten, E.C.; Elledge, S.J. Tumor aneuploidy correlates with markers of immune evasion and with reduced response to immunotherapy. Science 2017, 355, eaaf8399.
- Ock, C.Y.; Hwang, J.E.; Keam, B.; Kim, S.B.; Shim, J.J.; Jang, H.J.; Park, S.; Sohn, B.H.; Cha, M.; Ajani, J.A.; et al. Genomic landscape associated with potential response to anti-CTLA-4 treatment in cancers. Nat. Commun. 2017, 8, 1050.
- Liu, L.; Bai, X.; Wang, J.; Tang, X.R.; Wu, D.H.; Du, S.S.; Du, X.J.; Zhang, Y.W.; Zhu, H.B.; Fang, Y.; et al. Combination of TMB and CNA Stratifies Prognostic and Predictive Responses to Immunotherapy Across Metastatic Cancer. Clin. Cancer Res. 2019, 25, 7413–7423.
- Li, B.; Cui, Y.; Nambiar, D.K.; Sunwoo, J.B.; Li, R. The Immune Subtypes and Landscape of Squamous Cell Carcinoma. Clin. Cancer Res. 2019, 25, 3528–3537.
- Chen, Y.P.; Wang, Y.Q.; Lv, J.W.; Li, Y.Q.; Chua, M.L.K.; Le, Q.T.; Lee, N.; Colevas, A.D.; Seiwert, T.; Hayes, D.N.; et al. Identification and validation of novel microenvironment-based immune molecular subgroups of head and neck squamous cell carcinoma: Implications for immunotherapy. Ann. Oncol. 2019, 30, 68–75.
- Mandal, R.; Senbabaoglu, Y.; Desrichard, A.; Havel, J.J.; Dalin, M.G.; Riaz, N.; Lee, K.W.; Ganly, I.; Hakimi, A.A.; Chan, T.A.; et al. The head and neck cancer immune landscape and its immunotherapeutic implications. JCI Insight 2016, 1, e89829.
- Feng, B.; Shen, Y.; Pastor Hostench, X.; Bieg, M.; Plath, M.; Ishaque, N.; Eils, R.; Freier, K.; Weichert, W.; Zaoui, K.; et al. Integrative Analysis of Multi-omics Data Identified EGFR and PTGS2 as Key Nodes in a Gene Regulatory Network Related to Immune Phenotypes in Head and Neck Cancer. Clin. Cancer Res. 2020, 26, 3616–3628.
- Chen, R.Z.; Pettersson, U.; Beard, C.; Jackson-Grusby, L.; Jaenisch, R. DNA hypomethylation leads to elevated mutation rates. Nature 1998, 395, 89–93.
- Eden, A.; Gaudet, F.; Waghmare, A.; Jaenisch, R. Chromosomal instability and tumors promoted by DNA hypomethylation. Science 2003, 300, 455.
- Karpf, A.R.; Matsui, S. Genetic disruption of cytosine DNA methyltransferase enzymes induces chromosomal instability in human cancer cells. Cancer Res. 2005, 65, 8635–8639.
- Cao, J.; Yan, Q. Cancer Epigenetics, Tumor Immunity, and Immunotherapy. Trends Cancer 2020, 6, 580–592.
- Villanueva, L.; Alvarez-Errico, D.; Esteller, M. The Contribution of Epigenetics to Cancer Immunotherapy. Trends Immunol. 2020, 41, 676–691.
- Berglund, A.; Mills, M.; Putney, R.M.; Hamaidi, I.; Mule, J.; Kim, S. Methylation of immune synapse genes modulates tumor immunogenicity. J. Clin. Investig. 2020, 130, 974–980.
- Jung, H.; Kim, H.S.; Kim, J.Y.; Sun, J.M.; Ahn, J.S.; Ahn, M.J.; Park, K.; Esteller, M.; Lee, S.H.; Choi, J.K. DNA methylation loss promotes immune evasion of tumours with high mutation and copy number load. Nat. Commun. 2019, 10, 4278.
- Cancer Genome Atlas, N. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature 2015, 517, 576–582.
- Papillon-Cavanagh, S.; Lu, C.; Gayden, T.; Mikael, L.G.; Bechet, D.; Karamboulas, C.; Ailles, L.; Karamchandani, J.; Marchione, D.M.; Garcia, B.A.; et al. Impaired H3K36 methylation defines a subset of head and neck squamous cell carcinomas. Nat. Genet. 2017, 49, 180–185.
- Weinberg, D.N.; Papillon-Cavanagh, S.; Chen, H.; Yue, Y.; Chen, X.; Rajagopalan, K.N.; Horth, C.; McGuire, J.T.; Xu, X.; Nikbakht, H.; et al. The histone mark H3K36me2 recruits DNMT3A and shapes the intergenic DNA methylation landscape. Nature 2019, 573, 281–286.
- Brennan, K.; Shin, J.H.; Tay, J.K.; Prunello, M.; Gentles, A.J.; Sunwoo, J.B.; Gevaert, O. NSD1 inactivation defines an immune cold, DNA hypomethylated subtype in squamous cell carcinoma. Sci. Rep. 2017, 7, 17064.
- Saloura, V.; Izumchenko, E.; Zuo, Z.; Bao, R.; Korzinkin, M.; Ozerov, I.; Zhavoronkov, A.; Sidransky, D.; Bedi, A.; Hoque, M.O.; et al. Immune profiles in primary squamous cell carcinoma of the head and neck. Oral Oncol. 2019, 96, 77–88.
- Jones, P.A.; Ohtani, H.; Chakravarthy, A.; De Carvalho, D.D. Epigenetic therapy in immune-oncology. Nat. Rev. Cancer 2019, 19, 151–161.
- Kong, Y.; Rose, C.M.; Cass, A.A.; Williams, A.G.; Darwish, M.; Lianoglou, S.; Haverty, P.M.; Tong, A.J.; Blanchette, C.; Albert, M.L.; et al. Transposable element expression in tumors is associated with immune infiltration and increased antigenicity. Nat. Commun. 2019, 10, 5228.
- Panda, A.; de Cubas, A.A.; Stein, M.; Riedlinger, G.; Kra, J.; Mayer, T.; Smith, C.C.; Vincent, B.G.; Serody, J.S.; Beckermann, K.E.; et al. Endogenous retrovirus expression is associated with response to immune checkpoint blockade in clear cell renal cell carcinoma. JCI Insight 2018, 3, e121522.
- Zhou, L.; Xu, N.; Shibata, H.; Saloura, V.; Uppaluri, R. Epigenetic modulation of immunotherapy and implications in head and neck cancer. Cancer Metastasis Rev. 2021, 40, 141–152.
- Di Giacomo, A.M.; Covre, A.; Finotello, F.; Rieder, D.; Danielli, R.; Sigalotti, L.; Giannarelli, D.; Petitprez, F.; Lacroix, L.; Valente, M.; et al. Guadecitabine Plus Ipilimumab in Unresectable Melanoma: The NIBIT-M4 Clinical Trial. Clin. Cancer Res. 2019, 25, 7351–7362.
- Taylor, K.; Loo Yau, H.; Chakravarthy, A.; Wang, B.; Shen, S.Y.; Ettayebi, I.; Ishak, C.A.; Bedard, P.L.; Abdul Razak, A.; Hansen, A.R.; et al. An open-label, phase II multicohort study of an oral hypomethylating agent CC-486 and durvalumab in advanced solid tumors. J. Immunother. Cancer 2020, 8, e000883.
- Kim, K.H.; Roberts, C.W. Targeting EZH2 in cancer. Nat. Med. 2016, 22, 128–134.
- Zhou, L.; Mudianto, T.; Ma, X.; Riley, R.; Uppaluri, R. Targeting EZH2 Enhances Antigen Presentation, Antitumor Immunity, and Circumvents Anti-PD-1 Resistance in Head and Neck Cancer. Clin. Cancer Res. 2020, 26, 290–300.
- Vougiouklakis, T.; Bao, R.; Nakamura, Y.; Saloura, V. Protein methyltransferases and demethylases dictate CD8+ T-cell exclusion in squamous cell carcinoma of the head and neck. Oncotarget 2017, 8, 112797–112808.
- Rodriguez, C.P.; Wu, Q.V.; Voutsinas, J.; Fromm, J.R.; Jiang, X.; Pillarisetty, V.G.; Lee, S.M.; Santana-Davila, R.; Goulart, B.; Baik, C.S.; et al. A Phase II Trial of Pembrolizumab and Vorinostat in Recurrent Metastatic Head and Neck Squamous Cell Carcinomas and Salivary Gland Cancer. Clin. Cancer Res. 2020, 26, 837–845.