Healthcare waste (HCW) disposal includes a multitude of disposal methods, including incineration, landfilling and chemical treatments. These rudimentary methods and their growing use present their own problems that negatively impact both the environment and, in turn, damage public health, thus contributing to a global healthcare crisis.
- waste disposal
- medicine
- global warming
- public health
1. Introduction
Healthcare has become one of the fastest growing global industries in recent years [1]. Worldwide health spending is higher than ever and continues to rise every year. In 2017, global health spending was estimated at USD 7.8 trillion worldwide and was around 10% of the world gross domestic product (GDP) [2]. This increase in spending is due to expanding population numbers and a greater need for healthcare interventions. The global population is increasing and is expected to continue to do so, with it estimated to be around 8.6 billion by 2030 and 9.8 billion by 2050 [3]. Consequently, there would be a need for more healthcare interventions and treatments as the population both expands and lives longer resulting in generation of more healthcare waste (HCW) than ever before.
With aging population, while chronic disease spending is continuing to grow, so too is the cost of having multiple morbid conditions (MMCs). MMCs lead to elevated use of use of primary care and specialist care services as well as increased medication use and elevated hospital admissions [4]. Rapoport et al. [5]. demonstrated that the use of clinician appointments increases by up to 51% with each additional chronic disease. As age increases so too does the likelihood of suffering with a chronic disease [6]. Having one chronic disease also makes it more likely that someone will suffer numerous associated comorbidities leading to further, complicated chronic disease management. This growing epidemic of chronic disease has meant that the HCW disposal practices are being utilised extensively and the HCW disposal industry is growing. Alongside the ongoing growth of chronic disease, both developed and developing countries around the world are carrying out improved contagion practices in order to handle pandemics such as Ebola and COVID-19 and as a result more potentially dangerous medical waste is being produced [7][8]. Infectious diseases are also increasing globally adding to the generation of more waste [9]. At present, around 1.47 billion tonnes of solid waste are produced each year globally and this figure has increased year on year [10]. Of these 1.47 billion tonnes, 5.9 million tonnes are estimated to be a result of HCW [11]. Yet, owing to the sensitive nature and rigorous legislative requirements, only limited studies have explored the HCW streams in detail to put forward optimum methods for their treatment [12].
European Union legislation separates HCW into the following three categories of materials: (i) any HCW that poses a risk of infection; (ii) HCW that is a chemical hazard; and (iii) medicines and medicinally contaminated waste containing a pharmaceutically active agent [13]. Almost 85% of waste generated by healthcare activity is considered ‘non-hazardous waste’ and the remaining 15% is labelled as ‘hazardous’ [14]. While non-hazardous waste may not sound dangerous, the means of safely disposing of this waste can have damaging effects on the environment. The ‘hazardous’ waste can be infectious, toxic or even radioactive [14] and hence comes with a host of disposal and non-disposal issues. As such, not all HCW is created equally and different categories of waste require different disposal methods. Globally, the volume of HCW generated (per kg/bed/day) ranges enormously depending on the region and country (Table 1).
Table 1. HCW generated (kg/bed/day) per country.
| Region | Country | HCW Generated (kg/bed/day) |
References |
|---|---|---|---|
| Europe | Ireland | 7.7 | [15] |
| UK | 3.3 | [16] | |
| Bulgaria | 2 | [16] | |
| Italy | 4 | [17] | |
| France | 3.3 | [16] | |
| Germany | 3.6 | [18] | |
| Greece | 3.6 | [19] | |
| Netherlands | 1.7 | [18] | |
| Norway | 3.9 | [16] | |
| Spain | 4.4 | [16] | |
| Latvia | 1.18 | [20] | |
| America | USA | 8.4 | [16] |
| Canada | 8.2 | [21] | |
| Argentina | 3 | [22] | |
| Brazil | 2.94 | [21] | |
| Ecuador | 2.09 | [23] | |
| El Salvador | 1.85 | [24] | |
| Asia | Bangladesh | 1.24 | [25] |
| China | 4.03 | [26] | |
| India | 1.55 | [25] | |
| Indonesia | 0.75 | [27] | |
| Iran | 3.04 | [25] | |
| Japan | 2.15 | [17][28] | |
| Jordan | 2.69 | [17] | |
| Korea | 2.4 | [29] | |
| Laos | 0.51 | [30] | |
| Malaysia | 1.9 | [25] | |
| Pakistan | 2.07 | [16] | |
| Palestine | 2.02 | [31] | |
| Thailand | 2.05 | [32] | |
| Turkey | 4.55 | [17] | |
| Nepal | 0.5 | [25] | |
| Lebanon | 5.7 | [33] | |
| Kazakhstan | 5.34 | [20] | |
| Vietnam | 1.57 | [25] | |
| Africa | Algeria | 0.96 | [34] |
| Cameroon | 0.55 | [35] | |
| Egypt | 1.03 | [36] | |
| Ethiopia | 1.1 | [37] | |
| Mauritius | 0.44 | [28] | |
| Morocco | 0.53 | [38] | |
| Sudan | 0.87 | [39] | |
| Tanzania | 0.75 | [17] |
This increasing volume of HCW means a surge in use of HCW disposal practices such as landfilling, composting and the most preferred method: incineration [29] as well as other routes such as source reduction and reprocessing and recycling. HCW disposal practices have been associated with a wide range of problems. These problems, while potentially very dangerous for the environment, have an even greater, more widespread effect on people [41]. When proper disposal techniques are carried out correctly, such as incineration, there is risk of emission of pollutants like acid gases, oxides of nitrogen, metals, particulate matter and sulphur [42]. These pollutants have had notable negative effects on human health effecting the respiratory system, the endocrine system and have led to higher incidences of chronic diseases and cancers [43]. However, a range of factors like HCW type, classification, mechanism of segregation and waste management techniques impact the emissions from incineration of HCW [44][45]. Thus, it is essential to ensure that incinerators are operated as per advanced technological and legislation (such as European Community (EC) guidelines [46] to have clean and safe processes [47]. While, when HCW is not disposed of in the correct or proper manner due to a wide range of potential factors, such as lack of facilities or equipment, lack of education and training or a lack of regulation, it has additional disastrous effects on the environment and in turn, on human health [48]. Additionally, waste disposal within healthcare does not only concern hospitals and healthcare settings such as pharmacies, it also involves the patient as a key contributor. Bashaar et al. [49] have demonstrated that many adults dispose of unused or expired medications in unsafe and unofficial manners, leading to unsafe pharmaceutical compounds ending up in the environment and then eventually to the general public which has health repercussions.
At present, every method of HCW disposal comes with disadvantages that not only pose a threat to the environment but also a threat to human health and wellbeing often via the environment. Efforts have been made in recent years to improve this counterproductivity in which HCW could be potentially harmful to human life. These efforts have led to a push for “greener” and “safer” means of HCW disposal such as autoclaving, microwaving and steam augor but even green methods come with a range of potential challenges as many are not suitable for large volumes of waste or are not widely available [50], moreover these methods tend to be supportive to conventional techniques than being their replacement. Such as a steam autoclave can sterilize bacteria in clinical solid waste but cannot be considered as an alternative technology to incineration due to the re-growth risk of the bacteria [51]. They have also led to further education for healthcare professionals and personnel on waste management and “green hospital” initiatives. Although attempts have been made to improve the process of HCW disposal, serious problems and safety issues related to public health still very much exist [52]. The growing global population, the increase in lifespan, and the global crisis in chronic disease mean not only is more HCW being produced than ever before but there is an even greater need to better manage it. Current methods of HCW disposal are limited in managing the global HCW problem. In order for substantial progress to be made on this, a more in-depth understanding of why this issue exists and the barriers to the design or innovation on improved HCW disposal technologies must first be explored. The true scope of just how damaging HCW disposal methods can be is not widely understood. It still remains an immense problem with disastrous global consequences to both health and well-being not to mention the damaging environmental effects. It is therefore critical for this problem to be better understood in order for global change to occur.
2. Currently Utilised Methods of HCW Treatment and Disposal
There are numerous methods of HCW treatment and disposal available globally, despite this, the most widely utilised method is still incineration with landfilling following closely behind [53]. Various irradiation methods such as microwaving and various methods of thermal treatment such as autoclaving and steam treatment are much more environmentally friendly than the most commonly employed methods, but they are not suitable for mass, large scale treatment of waste and generally are not even available in many countries globally [54]. While greener methods technically do exist, they are unsuitable and unrealistic for numerous reasons including their lack of ability to treat large volumes, their need to exclude volatile materials and the steep, expensive price tag that comes along with them. Some of the greener methods also include prior steps before use and as such only carry out partial waste disposal [55]. Zimmermann [56] also highlight that the use of greener techniques such as microwave must be considered in the context of other treatment options.
The currently used methods of HCW treatment and disposal can be broken down into three main categories (Figure 1): treatments involving 1. Thermal processes, 2. Chemical processes and 3. Irradiation processes [57]. Other methods of HCW treatment that do not include any of the three categories are: landfilling, safe reuse after reprocessing and recycling. The method/process employed depends on numerous factors including: the type of HCW, the equipment and facilities available, operations and maintenance availability, physical space available skillset of employees, regulatory requirements, public acceptability, costing, volume and type of waste [13] The following section outlines the various uses, limitations and strengths of each of the methods.
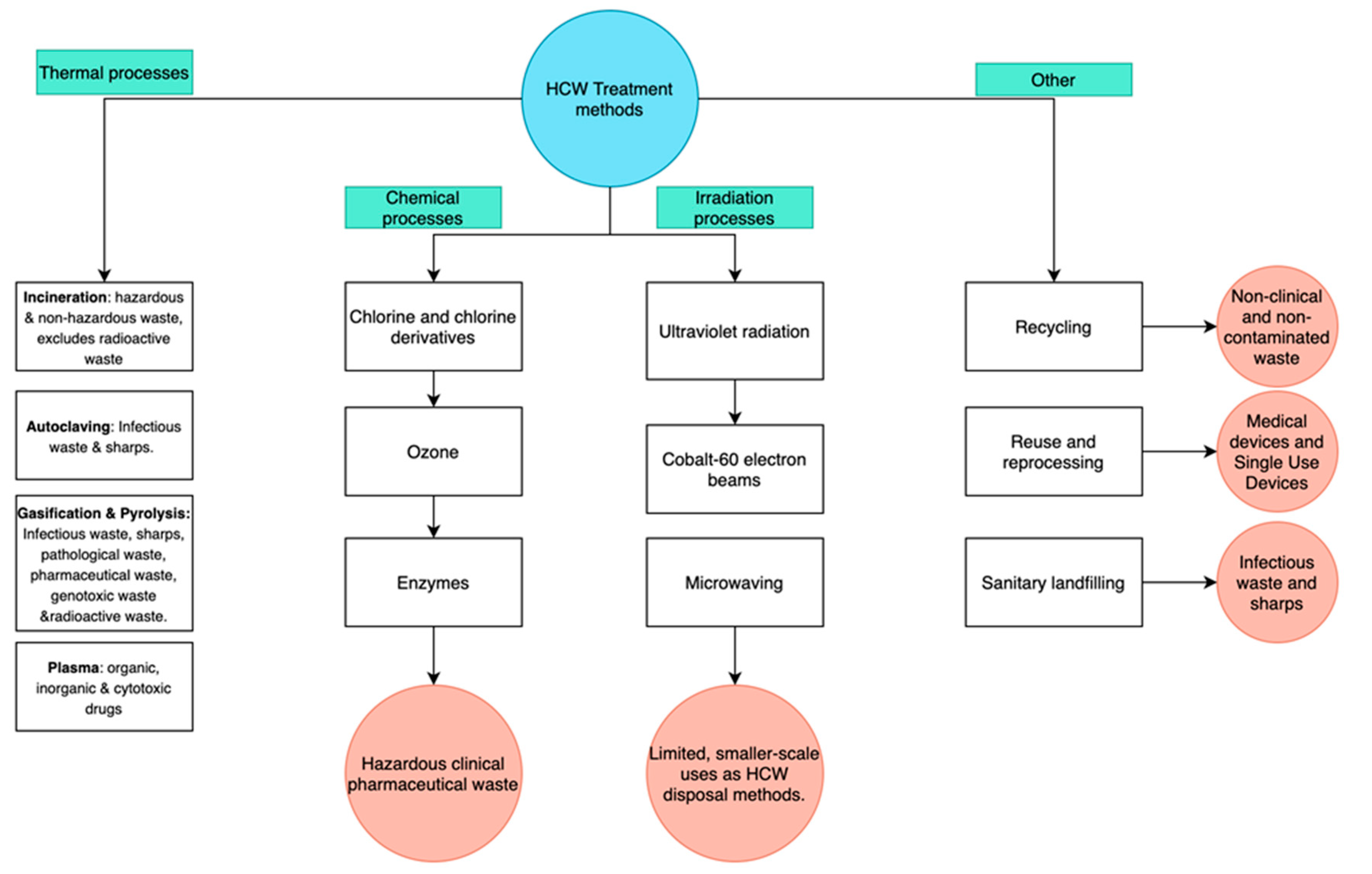
Figure 1. Categories of HCW methods.
This entry is adapted from the peer-reviewed paper 10.3390/healthcare9030284
References
- Yeoh, E.; Othman, K.; Ahmad, H. Understanding medical tourists: Word-of-mouth and viral marketing as potent marketing tools. Tour. Manag. 2013, 34, 196–201.
- Global Spending on Health: A World in Transition-WHO. Available online: (accessed on 10 July 2020).
- Wilson, D.C.; Rodic, L.; Modak, P.; Soos, R.; Carpintero, A.; Velis, K.; Simonett, O. Global Waste Management Outlook. UNEP United Nations Environment Programme. Available online: (accessed on 10 July 2020).
- McPhail, S.M. Multimorbidity in chronic disease: Impact on health care resources and costs. Risk Manag. Healthc. Policy 2016, 9, 143–156.
- Rapoport, J.; Jacobs, P.; Bell, N.R.; Klarenbach, S. Refining the measurement of the economic burden of chronic diseases in Canada. Chronic. Dis. Can. 2004, 20, 1–643.
- Raghupathi, W.; Raghupathi, V. An empirical study of chronic diseases in the United states: A visual analytics approach. Int. J. Environ. Res. Public Health 2018, 15, 431.
- Edmunds, K.L.; Elrahman, S.A.; Bell, D.J.; Brainard, J.; Dervisevic, S.; Fedha, T.P.; Few, R.; Howard, G.; Lake, I.; Maes, P.; et al. Recommendations for dealing with waste contaminated with Ebola virus: A Hazard Analysis of Critical Control Points approach. Bull. World Health Organ. 2016, 94, 424–432.
- Peng, J.; Wu, X.; Wang, R.; Li, C.; Zhang, Q.; Wei, D. Medical waste management practice during the 2019-2020 novel coronavirus pandemic: Experience in a general hospital. Am. J. Infect. Control 2020, 48, 918–921.
- Lafferty, K.D.; Mordecai, E.A. The rise and fall of infectious disease in a warmer world. F1000Research 2016, 5.
- Zaman, A. A comprehensive study of the environmental and economic benefits of resource recovery from global waste management systems. J. Clean. Prod. 2016, 124, 41–50.
- Voudrias, E.A. Healthcare waste management from the point of view of circular economy. Waste Manag. 2018, 75, 1–2.
- Vlachokostas, C.; Michailidou, A.V.; Achillas, C. Multi-Criteria Decision Analysis towards promoting Waste-to-Energy Management Strategies: A critical review. Renew. Sustain. Energy Rev. 2020, 138, 110563.
- Management of Solid Health-Care Waste at Primary Healthcare Centres: A Decision Making Guide, 1st ed.; World Health Organisation: Geneva, Switzerland, 2005; ISBN 9241592745.
- Healthcare Waste-WHO. Available online: (accessed on 11 August 2020).
- Reducing Waste in Irish Healthcare Facilities- Environmental Protection Agency. Available online: (accessed on 14 January 2021).
- Windfeld, E.S.; Brooks, M.S. Medical waste management—A review. J. Envrion. Manag. 2015, 163, 98–108.
- Eker, H.H.; Bilgili, M.S. Statistical analysis of waste generation in healthcare services: A case study. Waste Manag. Res. 2011, 29, 791–796.
- Farzadkia, M.; Emamjomeh, M.M.; Golbaz, S.; Sajadi, H.S. An investigation in hospital solid waste management in Iran. Glob. NEST J. 2015, 17, 771–783.
- Komilis, D.; Fouki, A.; Papadopoulos, D. Hazardous medical waste generation rates of different categories of health-care facilities. Waste Manag. 2012, 32, 1434–1441.
- Gusca, J.; Kalnins, S.A.; Blumberga, D.; Bozhko, L.; Khabdullina, Z.; Khabdullin, A. Assessment method of healthcare waste generation in Latvia and Kazakhstan. Energy Procedia 2015, 72, 175–179.
- Hossain, S.; Santhanam, A.; Nik Norulaini, N.A.; Mohd Omar, M.K. Clinical solid waste management practices and its impact on human health and environment—A review. Waste Manag. 2011, 31, 754–766.
- Pruss, A.; Giroult, E.; Rushbrook, P. Safe Management of Wastes from Health-Care Activities; World Health Organization: Geneva, Switzerland, 1999.
- Diaz, L.F.; Eggerth, L.L.; Enkhtsetseg, S. Anejo de Residuos de Establecimientos de Salud en Guayaquil, Ecuador; Pan American Health Organization: Quito, Equador, 2001.
- Johnson, M.K.; Gonzalez, L.M.; Duenas, L.; Gamero, M.; Relyea, G.; Luque, E.L.; Caniza, A.M. Improving waste segregation while reducing costs in a tertiary-care hospital in a lower-middle income country in Central America. Waste Manag. Res. 2013, 31, 733–738.
- Rabeie, O.L.; Miranzadeh, M.B.; Fallah, S.H.; Dehqan, S.; Moulana, Z.; Amouei, A.; Mohammadi, A.A.; Asgharnia, H.A.; Babaei, M. Determination of Hospital Waste Composition and Management in Amol City, Iran. Health Scope 2012, 1, 127–131.
- Yong, Z.; Gang, X.; Guanxing, W.; Tao, Z.; Dawei, J. Medical waste management in China: A case study of Nanjing. Waste Manag. 2009, 29, 1376–1382.
- Ananth, A.P.; Prashanthini, V.; Visvanathan, C. Healthcare waste management in Asia. Waste Manag. 2010, 30, 154–161.
- Mohee, R. Medical wastes characterization in healthcare institutions of Mauritius. Waste Manag. 2005, 25, 575–581.
- Jang, Y.C.; Lee, C.; Yoon, O.S.; Kim, H. Medical waste management in Korea. J. Envrion. Manag. 2006, 80, 107–115.
- Phengxay, S.; Okumura, J.; Miyoshi, M.; Sakisaka, K.; Kuroiwa, C. Health-care waste management in Lao PDR: A case study. Waste Manag. Res. 2005, 23, 571–581.
- Eleyan, D.; Al-Khatib Issam, A.; Garfield, J. System dynamics model for hospital waste characterization and generation in developing countries. Waste Manag. Res. 2013, 31, 986–995.
- Suwannee, A. Study on waste from hospital and clinics in Phitsanulok. Online J. Health Allied Sci. 2002, 1, 6–14.
- Maamari, O.; Brandam, C.; Lteif, R.; Salameh, D. Health care waste generation rates and patterns: The case of Lebanon. Waste Mang. 2015, 43, 550–554.
- Bendjoudi, Z.; Taleb, F.; Abdelmalek, F.; Addou, A. Healthcare waste management in Algeria and Mostaganem department. Waste Manag. 2009, 29, 1383–1387.
- Manga, E.V.; Forton, O.T.; Mofor, A.L.; Woodard, R. Health care waste management in Cameroon: A case study from the Southwestern Region. Resour. Conserv. Recycl. 2011, 57, 108–116.
- Abd El-Salam, M.M. Hospital waste management in El-Beheira Governorate, Egypt. J. Envrion. Manag. 2010, 91, 618–629.
- Tesfahun, E.; Kumie, A.; Beyene, A. Developing models for the prediction of hospital healthcare waste generation rate. Waste Manag. Res. 2015, 34, 219–220.
- Mbarki, A.; Kabbachi, B.; Ezaidi, A.; Benssaou, M. Medical waste management: A case study of the souss-massa-draa region, morocco. J. Environ. Prot. 2013, 4, 914–919.
- Suhair, A.; Gayoum, S. Management of hospital solid waste in Khartoum State. Environ. Monit. Assess. 2013, 185, 8567–8582.
- Minoglou, M.; Gerassimidou, S.; Komilis, D. Healthcare Waste Generation Worldwide and Its Dependence on Socio-Economic and Environmental Factors. Sustainability 2017, 9, 220.
- Khobragade, D. Health Care Waste: Avoiding Hazards to Living and Non-Living Environment by Efficient Management. Fortune J. Health Sci. 2019, 2, 14–29.
- Sharma, R.; Sharma, M.; Sharma, R.; Sharma, V. The impact of incinerators on human health and environment. Rev. Envrion. Health 2013, 28, 67–72.
- Darbre, P. Overview of air pollution and endocrine disorders. Int. J. Gen. Med. 2018, 11, 191–207.
- Thakur, V.; Ramesh, A. Healthcare waste management research: A structured analysis and review (2005–2014). Waste Manag. Res. 2015, 33, 855–870.
- Alvim-Ferraz, M.C.M.; Afonso, S.A.V. Incineration of healthcare wastes: Management of atmospheric emissions through waste segregation. Waste Manag. 2005, 25, 638–648.
- EC. Directive 2000/76/EC of the European Parliament and of the Council of December 4th 2000 on the Incineration of Waste. Off. J. Eur. Communities 2000, 43, 91–111. Available online: (accessed on 17 December 2020).
- James, R. Incineration: Why this may be the most environmentally sound method of renal healthcare waste disposal. J. Ren. Care 2010, 36, 161–169.
- Tudor, T.L.; Noonan, C.L.; Jenkin, L.E.T. Healthcare waste management: A case study from the National Health Service in Cornwall, United Kingdom. Waste Manag. 2005, 25, 606–615.
- Bashaar, M.; Thawani, V.; Hassali, M.A.; Saleem, F. Disposal practices of unused and expired pharmaceuticals among general public in Kabul. BMC Public Health 2017, 17, 45.
- Azmal, M.; Kalhor, R.; Dehcheshmeh, N.F.; Goharinezhad, S.; Heidari, Z.; Farzianpour, F. Going toward Green Hospital by Sustainable Healthcare Waste Management: Segregation, Treatment and Safe Disposal. Health 2014, 6, 2632–2640.
- Hossain, M.; Balakrishnan, V.; Rahman, N.N.N.A.; Sarker, M.; Islam, Z.; Kadir, M.O.A. Treatment of clinical solid waste using a steam autoclave as a possible alternative technology to incineration. Int. J. Environ. Res. Public Health 2012, 9, 855–867.
- Padmanabhan, K.; Barik, D. Health hazards of medical waste and its disposal. Energy Toxic Org. Waste Heat Power Gener. 2019, 99–118.
- Chauhan, A.; Singh, A. Healthcare waste management: A state-of-the-art literature review. Int. J. Environ. Waste Manag. 2016, 18, 120–144.
- Marincovic, N.; Vitale, K.; Holcer, N.; Dzakula, A.; Pavic, T. Management of Hazardous medical waste in Croatia. Waste Manag. 2008, 28, 1049–1056.
- Tudor, T.L.; Townend, W.K.; Cheeseman, C.R.; Edgar, J.E. An overview of arisings and large-scale treatment technologies for healthcare waste in the United Kingdom. Waste Manag. Res. 2009, 27, 374–383.
- Zimmermann, K. Microwave as an emerging technology for the treatment of biohazardous waste: A mini-review. Waste Manag. Res. 2017, 35, 471–479.
- Oliveira, E.A.; Nogueira, N.G.P.; Innocentini, M.D.M.; Pisani, R. Microwave inactivation of Bacillus atrophaeus spores in healthcare waste. Waste Manag. 2010, 30, 2327–2335.