The development of a dynamic consent medical blockchain system called DynamiChain, based on a ruleset management algorithm for handling health examination data.
- blockchain
- security management
- dynamic consent
1. Introduction
As part of the fourth industrial revolution in recent years, the advancement in blockchain technology has brought back the original theorem regarding smart contracts. Such algorithms based on computer protocols were designed to automatically facilitate, verify, and enforce the negotiation and implementation of digital contracts within an authority distributed architecture [1,2,3]. Smart contracts are being applied to a wide range of fields, mainly from the digital economy to healthcare, and the Internet of Things (IoT) [4]. To date, there is still a trend to use mainstream blockchain platforms, such as Bitcoin and Ethereum, when developing such platforms [5,6].
However, smart contract-related core technology is still in its infancy, and major technical challenges regarding security breach and privacy issues still exist. For example, blockchain cannot guarantee transactional privacy, since the values of all transactions and balances for each public key are publicly visible [7,8]. Moreover, a user’s Bitcoin transactions can be linked to reveal user’s information [9]. Similarly, each client can be uniquely identified by a set of nodes it connects [10]. “DAO Attack” that occurred in June 2016 [11,12,13] might be one of the most well-known blockchain targeted attacks. It was a severe incident that resulted in a loss amounting to more than $50 million Ether (approximately worth more than 8.5 billion dollars at that time) being transferred to an unauthorized account. This type of security breach is particularly sensitive in the medical industry, where personal health or medical information is being transferred within the network. In addition, contemporary blockchain-converged solutions do not consider restricted medical data regulations that are still obstacles in many countries worldwide.
In addition, current medical systems lack evidence-based data sharing policy, making it difficult for data providers to control their data based on their desired settings or policies. Some of the core values that blockchain technology aims to achieve, which are distributed authority, and consensus-based security, could play a vital role in providing these data providers with the rights they have over their own health data. This implies a crucial need for a system or solution that is suitable for the healthcare sector.
2. Proposed System
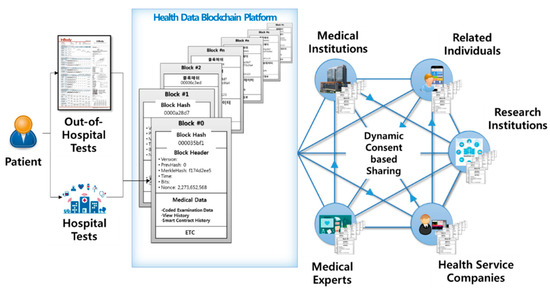
2.1. Overall System Architecture
2.2. Specific System Functions
| Function Classification | Function Contents |
|---|---|
| Data Provider’s App | Basic account functions (log in, create account, etc.) My examination history ledger My examination data (raw data and statistical data) Dynamic consent rule settings |
| Data Utilizer’s App | Basic account functions Input health examination results data function Data provider list management Data providers’ examination history management ledger Data providers’ examination data sharing usage history management ledger Request for data provider data function Data provider data request management function (applicable and non-applicable) |
| Blockchain System | Health examination data hash storage function Sync smart contract with real-time dynamic consent function settings Smart contract and blockchain ledger |
| Blockchain Admin Web | Channel management Peer node management User account management Blockchain data sharing history ledger management |
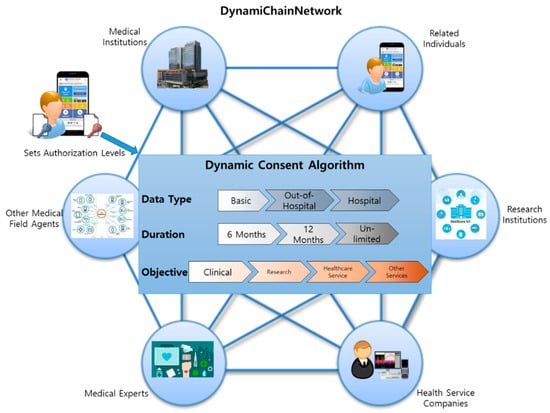
2.3. Dynamic Consent Algorithm
| Classification | Contents |
|---|---|
| Basic | Serial number, Sex, Age, Smoking Status, Drinking Status, Height, Weight, Waist |
| Out-of-hospital-level tests | Body Water, Protein, Minerals, Body Fat Amount, Weight, Bones and Muscle Amount, BMI, Body Fat Ratio, InBody Score, Abdomen Fat Ratio, Internal Organ Fat Level, Fat-free Mass, Basal Metabolism, Obesity Index, Recommended Calorie Amount, Body Parts’ Muscle Analysis (Right Arm, Left Arm, Body, Right Leg, Left Leg), Body Parts’ Fat Analysis (Right Arm, Left Arm, Body, Right Leg, Left Leg), Body Parts’ Body Water Analysis (Right Arm, Left Arm, Body, Right Leg, Left Leg), Body Parts’ Cell Water Analysis (Right Arm, Left Arm, Body, Right Leg, Left Leg), Body Parts’ Cell-free Water Analysis (Right Arm, Left Arm, Body, Right Leg, Left Leg), Cell-free Water Ratio, Phase Angle |
| Hospital-level tests | Cholesterol, Triglycerides, HDL Cholesterol, LDL Cholesterol, Diastatic Hemoglobin, Diastatic Hemoglobin Before Meal, Protein in Urine, Serum Creatinine, AST, ALT, Gamma GTP, Serial Number, Examination Date, Examined Institution, Sight (Left, Right), Blood Pressure (Systolic, Diastolic) |
2.4. Restricted Medical Data Policy Applied Work Flow Specifications
Some countries worldwide, including South Korea, still prohibit healthcare data to be stored outside certified medical institutions. Considering this, the proposed system only saves hash values of the health examination data and stores actual medical data separately in another database. Medical data’s multiple hash values are stored in the blockchain ledger so that data utilizers could read the data providers’ data based on set rules. Encoding–decoding access key to the actual medical data is, by default, managed by the data provider, unless the data provider delegates his or her authority to medical institutions where the actual database is stored. Using this mechanism, we balanced the data co-ownership ecosystem while preserving data integrity in a practical situation. This service process is shown in Figure 3. The hospital generates health an examination data of a data provider than the hash management system encrypts the data with the data provider’s public key and stores them with the hash value of the data. The data provider then confirms the data itself and dynamic consent rule in real-time and modifies the setting of the rules if necessary. The data utilizer requests for the data of the data provider, and the hospital confirms the request. The hospital allows access to actual data transmission after the endorsement process. Finally, data utilizer read the requested data through hash value comparison.
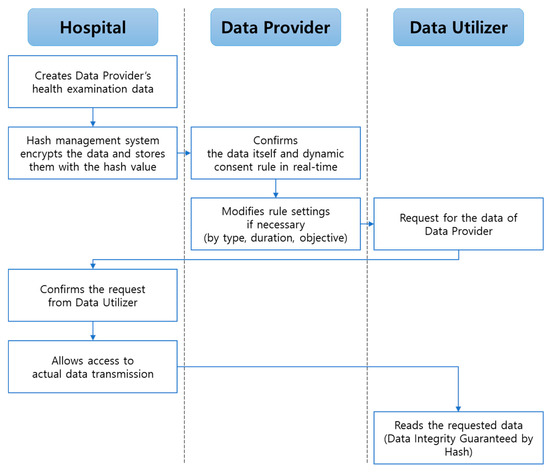
Hospital type data are created when data providers visit the hospital for a health examination. For each data, our proposed system stores encoded data, and accordingly, it has the data provider public key. Data providers have access to their own physical data and can set or change their dynamic consent rule in real-time. When other data utilizers (e.g., companies and research institutions) request for the allowed data providers’ medical data, the data source hospital confirms this request before transmitting the actual medical data to the requested data utilizer. Thereafter, the data utilizers could read the requested data. This is the key process that not only overcomes the issue of restricted health data sharing policies for some countries, but also guarantees data integrity. Note that out-hospital-data types are free from this scenario.
This entry is adapted from the peer-reviewed paper 10.3390/app11041612