5. Discussion
This study presents the first scoping review of occupational therapy interventions to address older adults’ falls using technology. The objectives defined focused on exploring the literature about the topic to determine the type of studies conducted, where these studies have usually been published, and the approaches and strategies used to reduce fall risk by occupational therapists using technology.
The results show that this is an emerging area, which began to be researched in the year 2012 [
58]. In a review by Chase and colleagues on home modification, only telecare was mentioned as a possible strategy by occupational therapists, but occupational therapists did not specifically develop that study. However, previous studies focused on the use of technology. For example, the iStoppFalls project focused on the use of exergames to reduce falls in older adults; this project was conducted from 2011 to 2014 to motivate and enhance the use of physical activity by community-dwelling adults aged more than sixty-five years by engaging with three purpose-built exergames to reduce falls [
43,
70].
The present review shows a trend toward carrying out studies with a qualitative approach [
63,
69] and mixed-methods studies [
65,
66], reinforcing the idea that is important to understand the perceptions and opinions of the older adults or occupational therapists and other health professionals under study to find out about their experiences with using the technology. This type of research helps us to understand the acceptance or not of technology and to determine how to improve or adapt it to make it useful in older people’s day-to-day lives [
71].
Regarding the place of publication, similar numbers of studies have been carried out in the USA [
58,
59,
60,
61] and Europe [
62,
63,
64,
65,
66,
67], even though progressive aging of the population is more apparent in Europe, and considering that previous European projects such as Prevent IT, Farseeing, and iStoppFalls, which are an essential background to fall prevention and the use of technology, were developed in Europe [
43,
44,
45].
Compared with other reviews about falls and occupational therapy [
41,
69], the present scoping review results are of a lower research quality, because it was not possible to find any controlled trials to demonstrate the effectiveness of the interventions developed alongside technology. The types of studies included descriptive studies [
61], case studies [
59,
60], experimental studies [
68], and qualitative studies [
63,
69], which are not considered to give a high level of evidence. Instead, some controlled trials were carried out in the field of falls and occupational therapy, for example, the one by Monaco and colleagues [
39].
As for the participant sample sizes and characteristics, the samples used were relatively small, except for one case [
61]. This is linked to the level of evidence mentioned above and the types of study used. The types of participant included older adults, occupational therapists, and/or informal caregivers.
Only one of the types of software developed, obstacle tool digitalization [
65], was tested in older adults, occupational therapists, and informal caregivers. The aim was to make it accessible for everybody, which is an essential factor to keep in mind in software development, according to the accessible software development model [
72], the philosophy of design for all [
73], and the inclusive perspective of the occupational therapy [
74], as this helps to break the digital divide, particularly among older adults [
74].
The studies included an extensive range of ages from 50 [
67] to 98 years old [
63], although older persons are classified as those aged 65 or more years. This reflects the perspective of preventing falls in people nearing retirement and the importance of active, healthy aging throughout life [
75,
76]. The life expectancy in Europe and USA, the main places of publication, is approximately 82 years old [
74]. Life expectancy at age sixty is higher in women than men [
77], and as can be seen in the results, females made up the highest percentage of participants in the studies, with 60–68% of participants being older women [
67,
69].
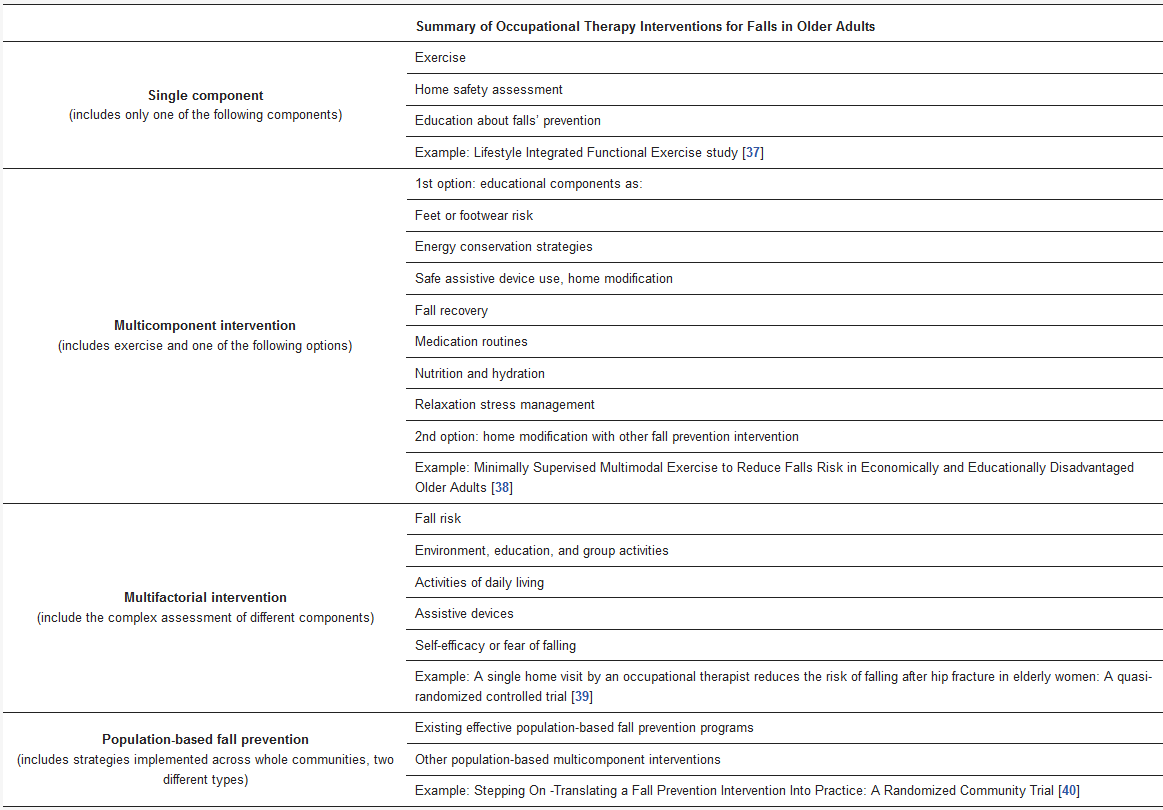
Regarding the type of intervention used to address falls in older adults through occupational therapy, only single-component interventions were used [
36], even though different authors have suggested that multifactorial programs help to prevent and reduce falls because of their complexity [
30]. None of the studies included an interprofessional team, despite its importance. The effectiveness of the multifactorial programs is also due to the use of an interprofessional team for fall prevention and treatment [
33].
In terms of multifactorial programs [
30], these involved exercise, as was done in two studies included in this review [
63,
68]; individualized and comprehensive fall risk assessment about the environment of an older adult, as done in a few studies mentioned in this review [
59,
64,
65,
66,
69]; and education on fall prevention, as done in two studies [
60,
68]. Furthermore, any intervention includes occupational therapy home visits [
78], which can be an essential aspect to include, especially in the cases of home modification [
59,
64,
65,
66,
69] and assistive technology [
58,
60,
61,
62]. The studies that integrated aging in place focused on assistive technology and home modifications because these factors are widely acknowledged as being the primary and preferred interventions during ageing [
79,
80]. Understanding how older people’s needs contribute to improving their quality of life, which is affected after a fall, is necessary [
13,
14,
15,
16,
18,
19].
A previous systematic review explored the cost-effectiveness of several occupational therapy interventions for older people, concluding that they are useful and cost-effective compared with standard care or other therapies [
81]. In this way, socioeconomic impact is one of the consequences of falls [
28]. However, the results were not focused on aspects related to socioeconomic impact.
Our results reinforce the idea that home modifications, assistive technology, and educational interventions can address extrinsic factors, particularly environmental factors, and exercise can address intrinsic factors. This is in accordance with previous studies about the use of occupational therapy interventions to address fall risk [
24,
82,
83,
84,
85].
Although, as mentioned above, some examples of assistive technology used to prevent falls in older adults include video-monitoring, health monitoring, electronic sensors, and fall detectors [
42] these were not included in the studies mentioned in this review. Moreover, regarding fall interventions globally, there is more focus on exercise options and an extensive range of technologies from virtual reality [
86] to wearables [
87] that were not included in these studies. Primarily, virtual reality interventions are used in occupational therapy, for example, in children [
86].
As a result of this review, it is suggested that researchers in this field perform more studies that include the latest technology in the field of falls, so that more studies with a higher level of evidence exist. Interprofessional and multifactorial interventions should be integrated.