1. Introduction
The increasing prevalence of type 2 diabetes mellitus is one of the most important problems for public health worldwide, especially in developed countries. According to data collected and published by Khan et al., 462 million individuals have been affected by type 2 diabetes mellitus in 2017 (6.28% of the world’s population) [
1]. Diabetes mellitus is a significant risk factor for the development of atherosclerosis [
2], near such risk factors as dyslipidemia [
3], arterial hypertension [
4], poor physical activity [
5], tobacco smoking [
6] and obesity [
7]. Diabetes also significantly increases the risk of cardiovascular events. In a seven-year follow-up study, the risk of a first heart attack was found to be 20.2% for people with diabetes and 3.5% for people without diabetes [
8].
As a result of atherosclerosis, to which diabetes predisposes, ischemic heart disease, stenosis of the carotid and vertebral arteries, chronic ischemia of the lower limbs, chronic intestinal ischemia, or narrowing of the renal arteries may develop, among others [
9]. Chronic lower extremity ischemia is a manifestation of peripheral arterial disease (PAD) affecting arteries responsible for blood supply of lower limb. It may result from stenosis (narrowing) or occlusion (complete blockage) of vascular lumen [
10]. Atherosclerosis is responsible for approximately 95% of cases and other factors such as vasculitis, as well as genetic and traumatic causes for approximately 5% [
11].
The prevalence of lifestyle diseases in the population, including the clinically evident consequences of atherosclerosis, increases with age. In view of the progressive aging of the population in highly developed countries, the importance of geriatric problems, such as the frailty syndrome (Frailty), for healthcare systems is increasing [
12]. Frailty is a geriatric syndrome that results from a multi-system reduction in reserves, deterioration of the ability to adapt to stressful situations, and thus an increased risk of such adverse phenomena as infections, falls, deterioration of cognitive abilities, dependence on other people or institutions [
13,
14].
2. Pathology and Epidemiology of PAD
Atherosclerosis is a chronic inflammatory disease, and processes such as endothelial dysfunction, oxidative stress, oxidative modification of low-density lipoproteins, intimal lipid deposition, smooth muscle cells proliferation, foam cells formation, apoptosis and necrosis, and local and systemic inflammatory response are involved in pathogenesis of atherosclerosis [
34]. Atherosclerosis is a pathological process involving the wall of arteries, which leads to plaque formation, narrowing of lumen of the vessel and chronic ischemia of the supplied organ. It may result in clinical manifestation of such diseases as coronary heart disease, stroke and peripheral arterial disease (PAD) [
35]. It is worth noting that the lack of mobility, which is an important element in the development of Frailty, is associated with an additional contribution to the reduction of blood flow dynamics in the lower extremities. It is noteworthy that diabetes is not only a risk factor for occurrence atherosclerosis but also for acceleration its development [
36]. Diabetes affects the function of endothelial cells, smooth muscle, and platelets, contributing to plaque instability, rupture, and cardiovascular events [
37].
Hyperglycemia and insulin resistance are two significant factors responsible for promoting of cardiovascular diseases development in patients with diabetes mellitus through such biochemical mechanisms as increased aldose reductase substrate conversion, formation of advanced glycation end-products, activation of protein kinase C, protein modification by N-acetylglucosamine, activation of the transcription factor NFAT, activation of NLRP3 inflammasome and peptidylarginine deaminase 4, and NETosis activation [
38]. NETosis is a form of neutrophil cells death which participates in immune response against pathogens. During NETosis, neutrophils release neutrophil extracellular traps (NETs), which can capture and kill pathogens [
39]. Reactive oxygen species and cellular death are associated with the majority of biochemical alterations promoting development of cardiovascular disease in the course of diabetes [
40].
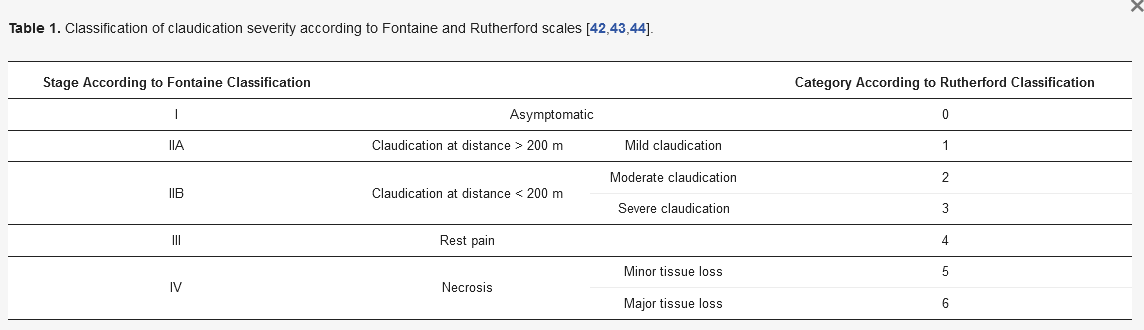
A typical symptom for chronic lower extremity ischemia is intermittent claudication, which is characterized by limb (especially calf) pain associated with walking and relieved by rest [
41]. There are two scales widely used in clinical practice to describe the severity of claudication: the Fontaine classification and the Rutherford classification, presented in [
42,
43,
44]. Scales such as, among others, Bollinger’s angiographic classification, Graziani’s morphologic categorization and Society for Vascular Surgery WIfI (wound, ischemia, foot infection) classification are also used to assess the severity of the disease [
45]. The most severe form of peripheral arterial disease affecting lower limb is critical limb ischemia (CLI) characterized by rest pain, ulcer and tissue necrosis. It may be complicated by infection. In some cases, amputation may be necessary [
46].
Table 1. Classification of claudication severity according to Fontaine and Rutherford scales [
42,
43,
44].
The prevalence of PAD on the European continent has been estimated at 5.3% (40 million subjects) [
47], while that in the European Union (EU) has been estimated at 3.4% (17 million patients) [
48]. It is estimated that prevalence of PAD among non-EU citizens on the European continent is 9.2% [
49]. Song et al. performed meta-analysis of 118 papers. It has been assessed that 236.62 million people globally aged 25 years and older were living with peripheral arterial disease in 2015, meaning that the global prevalence of peripheral arterial disease in this population is 5.56% [
50]. The PANDORA study, in which 10,287 people from six European countries were enrolled, showed significant differences in PAD prevalence between individual countries: Greece (28.0%), Italy (22.9%), France (12.2%), Switzerland (12.2%), The Netherlands (8.1%) and Belgium (7.0%) [
51].
Olinic et al. distinguished the following risk factors for the progression of PAD: tobacco use, physical inactivity, unhealthy diet, harmful use of alcohol, hypertension, diabetes, dyslipidemia, obesity, poverty, low educational status, advancing age, gender, genetic disposition, stress, depression, inflammation, lower glomerular filtration rate, higher interleukin-6 levels, presence of coronary artery calcification, long-term air pollution, infection disease [
49]. Fowkes et al. performed a systematic review and analysis to assess risk factors for peripheral arterial disease. According to the results of this study the most strongly correlating with PAD risk factors in high-income countries were smoking (current smoker) (OR 2.72, 95% CI: 2.39–3.09), history of other cardiovascular disease such as coronary heart disease or stroke (OR 2.55, 95% CI: 2.16–3.02), smoking in the past (OR 2.03, 95% CI: 1.71–2.41) and diabetes (OR 1.88, 95% CI: 1.66–2.14) [
47].
It should be emphasized that the clinical course of peripheral arterial disease in patients with diabetes and those without diabetes shows some differences. In patients living with diabetes, arteries below the knee (such as popliteal, anterior tibial, peroneal and posterior tibial) are more commonly involved [
52]. Patients with diabetes show symmetrical, multi-segmental stenosis [
53]. These facts are reflected in the difference in the effectiveness of reperfusion therapy between people with and without diabetes. It has been shown that patients living with diabetes present a higher rate of binary restenosis (54.4% vs. 31.5%) and amputation (24.4% vs. 1.5%) at 2 years following peripheral transluminal angioplasty [
54]. DeRubertis et al. performed a retrospective analysis of medical history of 291 patients suffering from lower limb ischemia treated by percutaneous intervention. In this study, it is documented that diabetes is associated with reduced effectiveness of primary intervention (patency after 6, 12 and 18 months in patients with diabetes vs. patients without diabetes 82 ± 2%, 53 ± 4%, and 49 ± 4% vs. 88 ± 2%, 71 ± 4%, and 58 ± 4% respectively) with no significant difference in the effectiveness of secondary intervention [
55].
The occurrence of suboptimal blood glucose levels is associated with a greater likelihood of developing cardiovascular complications, including peripheral arterial disease. Zhang et al. conducted a meta-analysis of 26 prospective cohort studies. According to the results of this study, the relative risk for the emergence of peripheral arterial disease associated with a 1% increase in glycated hemoglobin is 1.29 (95% CI: 1.18–1.40) [
56].
A meta-analysis published in 2017 including 21 studies confirmed that diabetes is a strong factor increasing mortality among patients with PAD (OR 1.89, 95% CI: 1.51–2.35). Taking into consideration only patients with critical limb ischemia, the influence of diabetes on mortality was even stronger (OR 2.38, 95% CI: 1.22–4.63) [
57].