Artificial intelligence may support the management of non-insulin-treated type 2 diabetes by moving care from reactive follow-up to anticipatory clinical decision-making. Its potential applications include early detection of metabolic deterioration, identification of therapeutic inertia, interpretation of glycemic data, risk stratification, remote monitoring, and personalized follow-up intensity. Rather than replacing clinical judgment, artificial intelligence may help clinicians recognize hidden trajectories and intervene before clinical deterioration becomes evident.
- type 2 diabetes
- artificial intelligence
- non-insulin therapy
- therapeutic inertia
- anticipatory care
- clinical decision support
- digital health
- personalized medicine
- glucose monitoring
- metabolic deterioration
1. Introduction
Type 2 diabetes mellitus (T2D) is a highly prevalent, heterogeneous, and progressive chronic disease. In many patients, the longest part of the disease course occurs before insulin initiation, during a phase managed with lifestyle intervention and non-insulin glucose-lowering therapies [1][2][3][4][5]. This phase is clinically decisive because metabolic deterioration, treatment failure, therapeutic inertia, and cardiometabolic risk progression may remain partially hidden until deterioration has already become established [5][6][7][8].
Routine care is still frequently based on intermittent visits, periodic laboratory assessment, and retrospective interpretation of glycated hemoglobin. Although HbA1c remains essential for evaluating medium-term glycemic exposure, it does not fully capture short-term glucose fluctuations, post-prandial excursions, glycemic variability, adherence patterns, behavioral changes, or the dynamic interaction between metabolic control and cardiometabolic risk [3][4][9][10][11][12].
Artificial intelligence (AI) may help address this gap by integrating multidimensional clinical, biochemical, behavioral, digital, and glycemic data into dynamic risk-assessment frameworks [13][14][15]. In non-insulin-treated T2D, the most relevant role of AI is not autonomous therapeutic decision-making, but earlier recognition of clinically meaningful patterns that may otherwise remain unnoticed [1][15][16][17][18].
2. From Reactive Management to Anticipatory Care
Reactive management remains common in routine diabetes care. Patients are assessed at predefined intervals, laboratory results are reviewed, and treatment is often intensified only after glycemic failure has become evident. This approach is operationally simple, but it may be poorly aligned with the progressive and dynamic nature of T2D [5][7][8].
Anticipatory care proposes a different logic. Instead of waiting for failure to become visible, it aims to detect early signals of unfavorable trajectory and to adapt follow-up, education, and therapy before the patient crosses a clinically meaningful threshold [1][15][16][17][18]. This does not imply overtreatment. It means using available information more intelligently to distinguish stable patients from those who are beginning to drift.
In this framework, the clinical question changes from “What is the current HbA1c?” to “Where is this patient going, and how soon do we need to act?” AI may support this transition by connecting longitudinal data fragments, detecting deviations from previous stability, and highlighting patients who require earlier reassessment [13][14][15][16][17][18].
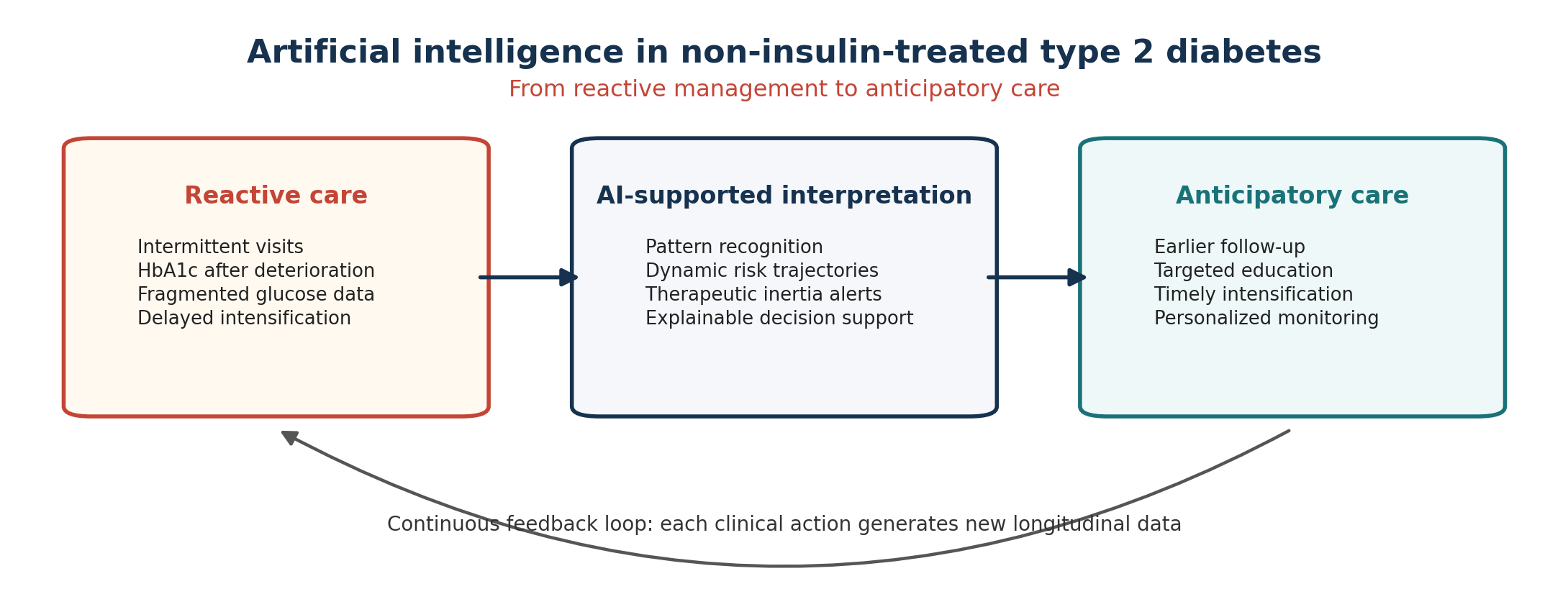
Figure 1. AI-supported transition from reactive management to anticipatory care in non-insulin-treated type 2 diabetes.
3. Why Non-Insulin-Treated T2D Is a Key Scenario for AI
The use of AI in diabetes has often focused on insulin-treated disease, automated insulin delivery, sensor-augmented systems, and closed-loop algorithms. This emphasis is understandable because insulin therapy requires frequent short-term decisions and carries an immediate risk of hypoglycemia [3][13][15]. However, it may underestimate the potential value of AI in the much larger population of patients with T2D who are not treated with insulin [1][15].
In non-insulin-treated T2D, the central clinical problem is usually not minute-by-minute dose adjustment, but timely recognition of progressive loss of control, insufficient response to therapy, increasing cardiometabolic risk, and the need for treatment intensification [4][5][6][7][8]. These processes are gradual, multifactorial, and difficult to capture through isolated clinical encounters.
Non-insulin-treated T2D is therefore an ideal scenario for AI-supported interpretation: it is common, longitudinal, data-rich, heterogeneous, and exposed to therapeutic inertia [6][7][8][15][18].
4. Clinical Applications
Potential applications of AI in non-insulin-treated T2D include interpretation of structured self-monitoring of blood glucose, intermittent or professional continuous glucose monitoring, detection of post-prandial excursions, recognition of glycemic variability, prediction of loss of control, and identification of patients who may require treatment intensification [9][10][11][12][13][14][15].
A clinically important application is the reduction of therapeutic inertia. Therapeutic inertia refers to delayed treatment intensification despite evidence that goals are not being achieved, and it remains one of the most persistent barriers in diabetes care [7][8]. AI-based tools may help identify patients with repeated borderline HbA1c values, rising fasting glucose, weight gain, declining adherence, or worsening renal function before failure becomes obvious [16][17][18].
AI may also help personalize follow-up intensity. Patients with stable multidimensional profiles may continue routine monitoring, whereas patients showing early unfavorable trends could be prioritized for earlier contact, laboratory reassessment, targeted education, or therapeutic review [1][15][16][17][18].
5. Integration with Cardiometabolic Medicine
T2D is not only a disorder of glucose metabolism. Cardiovascular disease, chronic kidney disease, obesity, dyslipidemia, hypertension, and metabolic liver disease frequently coexist and interact. AI-supported models may help integrate HbA1c, body weight, blood pressure, lipid profile, kidney function, albuminuria, medication history, comorbidities, and adherence into a more complete clinical phenotype [5][6][17].
This multidimensional interpretation may be particularly useful when the patient’s main vulnerability is not simply hyperglycemia but broader cardiometabolic risk. Predictive models have already been explored for diabetic complications, poor glycemic control, and chronic kidney disease risk in real-world diabetes populations [16][17].
In everyday practice, the goal should not be to generate opaque risk scores, but to produce concise, explainable, and actionable information that helps clinicians decide who should be reviewed earlier and why [15][19][20].
6. Limitations and Implementation Barriers
Despite its potential, AI in diabetes care faces important limitations. Many models are developed using retrospective datasets, selected populations, or highly structured data sources, and therefore require external validation before clinical implementation [19][20]. Data quality is a major challenge because relevant information is often incomplete, inconsistently coded, or distributed across disconnected systems [19][20].
Missing data are not merely a technical inconvenience. In real-world diabetes care, missing values may reflect social vulnerability, lower digital literacy, fragmented follow-up, reduced access to care, or lower patient engagement. If this missingness is ignored, AI tools may reinforce existing inequalities rather than reduce them [19][20].
Explainability is essential. A model that identifies a patient as high risk without clarifying whether the risk is driven by rising glucose values, weight gain, kidney function decline, reduced adherence, or previous treatment failure may be difficult to trust and difficult to translate into action [19][20]. AI outputs should remain consultative and clinician-governed, not autonomous directives.
7. Practical Implications for Diabetologists
For diabetologists, AI should be understood as an extension of clinical observation rather than a competing intelligence. Its practical value lies in improving timing, prioritization, and precision: identifying who is drifting, who should be recalled earlier, who may fail current therapy, who requires more intensive monitoring, and who may need treatment intensification before prolonged deterioration occurs [1][15][16][17][18].
This approach may be especially useful in healthcare systems characterized by high outpatient volumes, limited visit time, and increasing data availability. Properly designed AI tools could reduce information fragmentation and help transform routine clinical data into actionable trajectories [13][14][15][19].
However, the diabetologist remains essential for interpreting context, evaluating competing risks, discussing patient preferences, and deciding whether a predicted risk requires action. AI can help clinicians see earlier, but it cannot replace clinical responsibility [19][20].
8. Conclusions
Artificial intelligence may become a clinically relevant tool in non-insulin-treated T2D by supporting the transition from reactive management to anticipatory care. Its greatest value lies in identifying hidden trajectories, predicting metabolic deterioration, reducing therapeutic inertia, improving glycemic data interpretation, and personalizing follow-up intensity [1][13][14][15][16][17][18].
Successful implementation will require clinically validated, explainable, equitable, interoperable, and workflow-compatible tools. The success of AI should not be judged only by predictive accuracy, but by its ability to improve clinical timing, reduce inertia, support safer decisions, and enhance the quality of medical reasoning [19][20].
In non-insulin-treated T2D, AI should be understood less as a new therapeutic actor and more as a new way of reading clinical time.
Table 1. Selected AI applications in non-insulin-treated T2D.
|
Clinical area |
Data sources |
AI function |
Potential benefit |
|
Glycemic interpretation |
HbA1c, SMBG, CGM, meals, activity |
Pattern recognition; variability analysis |
Earlier identification of hidden instability |
|
Therapeutic inertia |
HbA1c trends, medications, visits, adherence |
Trajectory detection; risk alerts |
More timely clinical reassessment |
|
Remote follow-up |
Glucose, weight, BP, activity, symptoms |
Alert prioritization; adaptive monitoring |
Earlier contact for deteriorating patients |
|
Progression prediction |
Longitudinal clinical, renal, and metabolic data |
Dynamic risk modeling |
Prediction of loss of control or complications |
|
Generative AI support |
Clinical notes, education material, patient-reported data |
Summarization; communication support |
Reduced administrative burden under clinician supervision |
This entry is adapted from: doi:10.20944/preprints202606.0090.v1
References
- Labate AM, Cimino E, Giacomelli L, Ettori S, Oladeji OA, Agosti B. Artificial Intelligence in Non-Insulin-Treated Type 2 Diabetes: From Reactive Management to Anticipatory Care. Preprints. 2026. doi:10.20944/preprints202606.0090.v1.
- International Diabetes Federation. IDF Diabetes Atlas, 11th ed. Brussels: International Diabetes Federation; 2025.
- American Diabetes Association Professional Practice Committee. Diabetes Technology: Standards of Care in Diabetes-2026. Diabetes Care. 2026;49(Suppl 1):S150-S182.
- American Diabetes Association Professional Practice Committee. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes-2026. Diabetes Care. 2026;49(Suppl 1):S183-S206.
- Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM, et al. Management of Hyperglycemia in Type 2 Diabetes: A Consensus Report by the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2022;45:2753-2786.
- Chung WK, Erion K, Florez JC, Hattersley AT, Hivert MF, Lee CG, et al. Precision medicine in diabetes: A consensus report from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia. 2020;63:1671-1693.
- Khunti K, Gomes MB, Pocock S, Shestakova MV, Pintat S, Fenici P, et al. Therapeutic inertia in the treatment of hyperglycaemia in patients with type 2 diabetes: A systematic review. Diabetes Obes Metab. 2018;20:427-437.
- Khunti S, Khunti K, Seidu S. Therapeutic inertia in type 2 diabetes: Prevalence, causes, consequences and methods to overcome inertia. Ther Adv Endocrinol Metab. 2019;10:2042018819844694.
- Battelino T, Danne T, Bergenstal RM, Amiel SA, Beck R, Biester T, et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care. 2019;42:1593-1603.
- Young LA, Buse JB, Weaver MA, Vu MB, Mitchell CM, Blakeney T, et al. Glucose self-monitoring in non-insulin-treated patients with type 2 diabetes in primary care settings: A randomized trial. JAMA Intern Med. 2017;177:920-929.
- Shields S, Thomas S, Kerr D, et al. Continuous glucose monitoring among adults with type 2 diabetes receiving non-insulin or basal insulin therapy in primary care. Sci Rep. 2024;14:31990.
- Aronson R, Brown RE, Abitbol A, Goldenberg RM, Yale JF. Continuous glucose monitoring in non-insulin-treated type 2 diabetes: Evidence and practical considerations. Diabetes Obes Metab. 2025.
- Contreras I, Vehi J. Artificial Intelligence for Diabetes Management and Decision Support: Literature Review. J Med Internet Res. 2018;20:e10775.
- Dankwa-Mullan I, Rivo M, Sepulveda M, Park Y, Snowdon J, Rhee K. Transforming Diabetes Care Through Artificial Intelligence: The Future Is Here. Popul Health Manag. 2019;22:229-242.
- Mackenzie SC, Sainsbury CAR, Wake DJ. Diabetes and artificial intelligence beyond the closed loop: A review of the landscape, promise and challenges. Diabetologia. 2024;67:223-235.
- Fan Y, Li X, Zhang L, Zeng X, Yang X, Yang Y, et al. Machine Learning Approaches to Predict Risks of Diabetic Complications and Poor Glycemic Control. Front Endocrinol (Lausanne). 2021;12:734747.
- Ravizza S, Huschto T, Adamov A, Boehm L, Buesser A, Floether FF, et al. Predicting the early risk of chronic kidney disease in patients with diabetes using real-world data. Nat Med. 2019;25:57-59.
- Musacchio N, Zilich R, Masi D, Baccetti F, et al. A transparent machine learning algorithm uncovers HbA1c patterns associated with therapeutic inertia in patients with type 2 diabetes and failure of metformin monotherapy. Int J Med Inform. 2024;190:105550.
- Rajkomar A, Dean J, Kohane I. Machine Learning in Medicine. N Engl J Med. 2019;380:1347-1358.
- Wiens J, Saria S, Sendak M, Ghassemi M, Liu VX, Doshi-Velez F, et al. Do no harm: A roadmap for responsible machine learning for health care. Nat Med. 2019;25:1337-1340.