To report a rare case of acute coronary syndrome (ACS) with triple-vessel disease, in which the electrocardiographic (ECG) presentation was complicated by multivessel involvement and collateral circulation(CC). This report aims to elucidate the unique underlying pathophysiology—the "collateral steal" phenomenon—and highlight the diagnostic challenges in such complex presentations. A 59-year-old male presented with acute chest pain lasting 5.5 hours. The ECG demonstrated anterior ST-segment elevation (V1-V5) with inferior pathological Q waves, suggestive of acute anterior ST-segment elevation myocardial infarction (STEMI) and a prior inferior infarction. Coronary angiography confirmed triple-vessel disease: severe stenosis in the left anterior descending (LAD) and left circumflex arteries, along with a subtotal occlusive thrombus in the mid segment of the right coronary artery (RCA) (TIMI flow grade 1).CC from the LAD to the RCA territory was observed. Primary percutaneous coronary intervention (PCI) was performed on the RCA. Symptoms were promptly relieved following balloon angioplasty, accompanied by reversal of the collateral flow. Subsequent stenting of both the RCA and LAD was successfully completed. Follow-up ECG showed complete resolution of the ST-segment elevation with evolving T-wave changes. This case illustrates a rare manifestation where acute RCA occlusion, in the setting of multivessel disease, precipitated acute severe anterior wall ischemia via a "collateral steal" mechanism. The absence of acute ST-segment elevation in the territory of the old inferior infarction, likely due to myocardial scar and collateral protection, underscores the complexity of ECG interpretation in multivessel acute coronary events and carries significant implications for clinical diagnosis.
- STEMI
- Acute Coronary Syndrome
- Triple-Vessel Disease
- Collateral Circulation
- Coronary Steal Phenomenon
- Electrocardiogram
- Percutaneous Coronary Intervention
1. Introduction
ECG remains the cornerstone for the rapid diagnosis of ACS. Anterior ST-segment elevation (STE) on ECG is classically recognized as the characteristic signature of acute LAD coronary artery occlusion. However, this canonical ECG pattern can be profoundly misleading in complex clinical scenarios involving multivessel coronary artery disease and well-developed CC.
A pivotal pathophysiological mechanism underlying this diagnostic pitfall is the collateral steal phenomenon: when the donor vessel (e.g., RCA) that provides collateral blood flow to a chronically stenotic recipient vessel (e.g., LAD) undergoes acute thrombotic occlusion, the reversal of collateral perfusion leads to ischemic ECG changes in the territory of the recipient vessel (anterior STE), rather than the territory corresponding to the culprit occluded artery. This atypical presentation creates a critical diagnostic dilemma in clinical practice.
Notably, the diagnostic accuracy of ECG for ACS is frequently challenged in patients with multivessel disease, prior myocardial infarction, or extensive collaterals. Beyond classic STEMI, a spectrum of STEMI-equivalent ECG patterns (e.g., De Winter pattern, Aslanger sign) [1][2] has been increasingly recognized as indicators of acute coronary occlusion requiring urgent reperfusion therapy. The conventional STEMI/non-STEMI classification system is inherently limited in identifying acute coronary occlusion accompanied by CC, underscoring the necessity of prompt coronary angiography for definitive diagnosis [3].
Herein, we report the case of a 59-year-old male patient presenting with anterior STE on ECG, mimicking acute LAD occlusion, whereas the culprit lesion was identified as acute RCA occlusion. This case elucidates the key role of collateral steal in generating misleading ECG findings in complex ACS. We emphasize the importance of maintaining high vigilance for atypical ECG patterns in multivessel disease and advocate for early coronary angiography to accurately identify the culprit vessel and guide optimal therapeutic decision-making.
2. Case Presentation
A 59-year-old man presented with a 1-year history of recurrent chest pain, acutely aggravated over the past 5.5 hours, accompanied by diaphoresis and pain radiating to the left shoulder, left upper limb, and back. There was no associated syncope or presyncope. He has a history of smoking, drinking and hypertension.Blood pressure was 128/78 mmHg. Troponin I level was normal. On admission ECG showed sinus rhythm with upward convex ST-segment elevation (2–9 mm) in leads V1–V5 and inferior leads, with pathological Q waves inferiorly (Figure 1). A preliminary diagnosis was acute anterior STEMI and old inferior myocardial infarction. Coronary angiography demonstrated 95% stenosis in the proximal LAD with TIMI grade 3 flow and collaterals from the LAD to the RCA.Approximately 80% stenosis in the mid-to-distal left circumflex artery.The mid RCA had partial thrombotic occlusion (TIMI grade 1 flow) with competitive flow in the posterolateral branch. After balloon angioplasty of the mid RCA, chest pain relieved and collaterals from the posterior descending artery (PDA) to the LAD emerged. Stents were placed in the RCA and LAD (Figure 2,Video). Peak troponin T level was 3246.00 pg/mL (reference, 0–14.1). Follow-up ECG showed complete resolution of anterior ST-segment elevation and T-wave evolution in anterior leads. Subsequent continuous ECG monitoring showed complete normalization of ST-segments in the anterior leads, with significant T-wave evolution in the anterior leads accompanied by sequential T-wave changes in other leads, over a 26-month follow-up period (Figure 3).
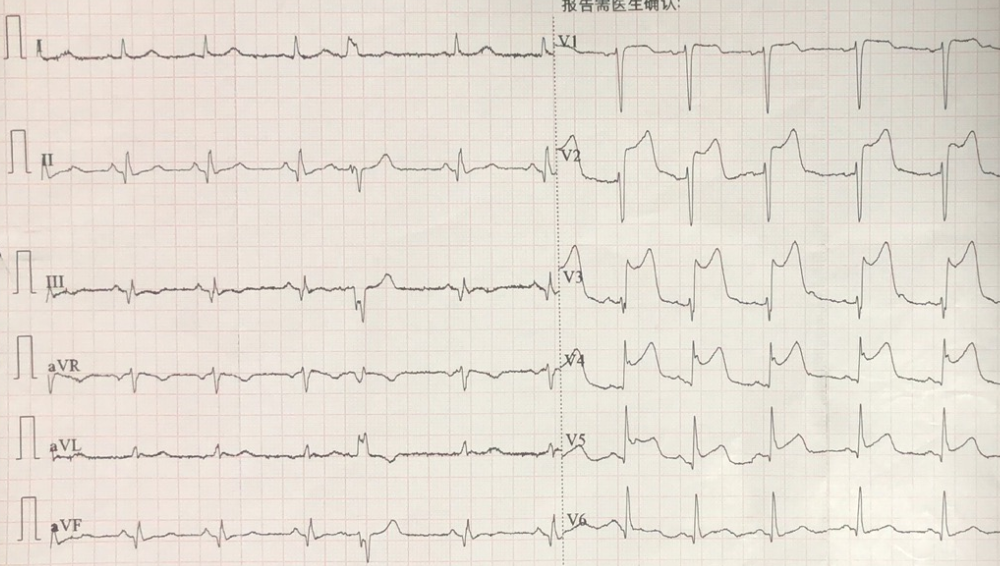
Figure 1. Initial ECG (anterior STEMI) prompted cath lab activation.
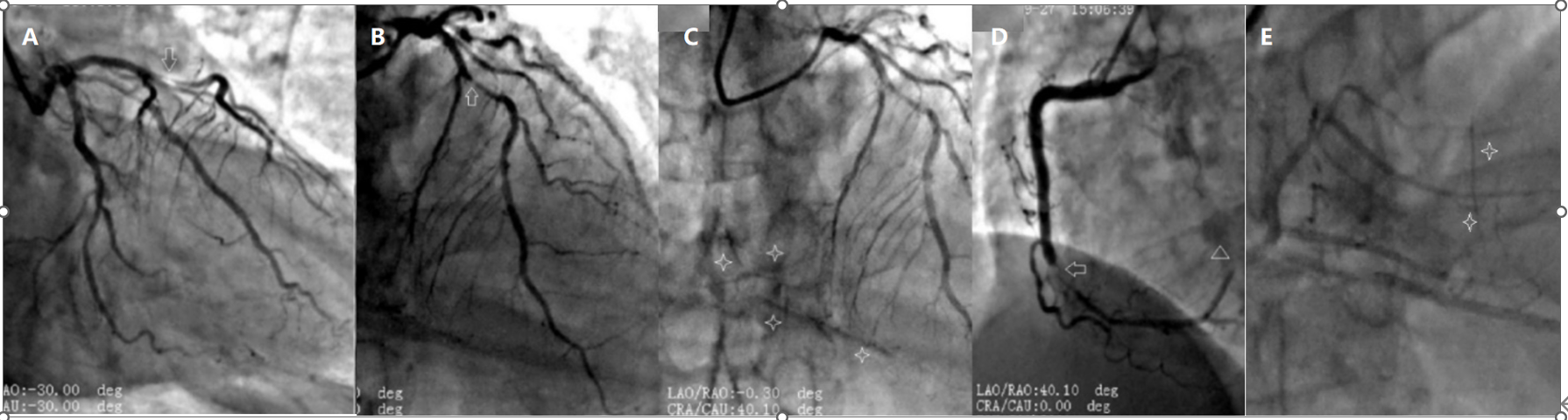
Figure 2. CAG shows: severe proximal LAD stenosis (A,B, arrows); subtotal mid RCA occlusion (D, arrow); CC from the LAD to the RCA is visible (C, four-pointed star), along with competitive flow in the left posterior lateral branch (D, triangle),Post-stent angiography of the right coronary artery demonstrating CC from the RCA to the LAD (E,four-pointed star).
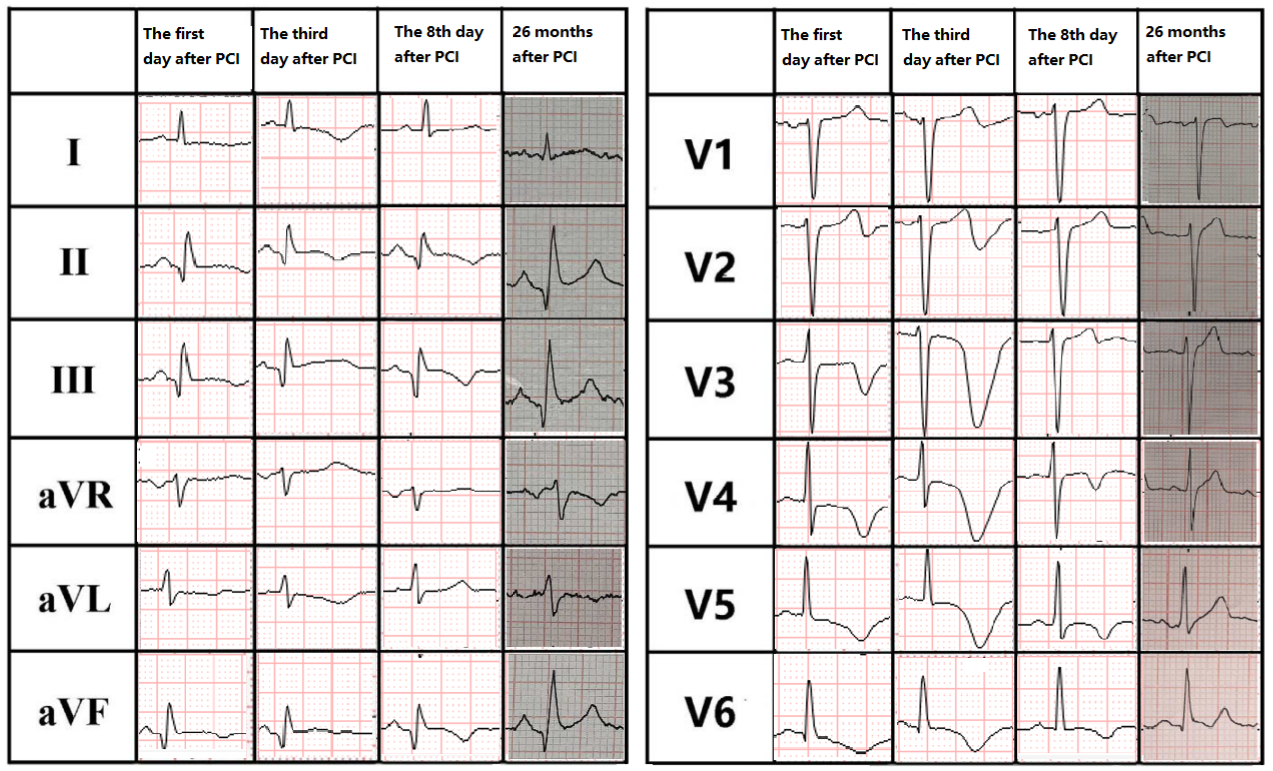
Figure 3. ECGs obtained on day 1, day 3, day 8, and at 26 months after PCI.
3. Discussion
Based on the clinical presentation and electrocardiographic features, the diagnosis was acute anterior STEMI, initially implicating the LAD artery. An old inferior myocardial infarction was also present. Coronary angiography revealed a subtotal occlusion with thrombus in the mid- RCA, identified as the acute culprit lesion. Despite severe proximal LAD stenosis, the LAD supplied coronary flow to the RCA, with a significantly better TIMI flow than the RCA. Chest pain resolved immediately after RCA revascularization, confirming it as the true culprit vessel.
Explanation for Electrocardiographic Changes
Initial RCA occlusion likely occurred due to pre-existing severe stenosis. As the LAD was not yet significantly stenosed, it presumably supplied collaterals to the inferior wall. Subsequent spontaneous RCA thrombolysis allowed recanalization, but pathological inferior Q waves persisted.
Disease progression and lack of risk-factor control led to severe LAD stenosis. This reversed the pressure gradient, causing the recanalized RCA to supply the LAD territory via collaterals.
The current acute event involved RCA re-occlusion. This caused another collateral flow reversal, forcing the severely stenosed LAD to supply the occluded RCA, creating anterior wall ischemia manifesting as ECG changes mimicking anterior STEMI. Concurrently, pre-existing inferior wall fibrosis and altered hemodynamics from collaterals modified the typical inferior RCA occlusion pattern, explaining absent ST-segment elevation in inferior leads.
During intervention, RCA flow restoration immediately relieved symptoms as the RCA resumed supplying the LAD territory.
After PCI restored antegrade flow in both vessels,CC was no longer angiographically visible.
Simultaneous acute coronary events in two major arteries are rare. This represents an unusual "two-vessel acute coronary syndrome," distinct from common etiologies like embolism or spasm [4][5]. The lesion location is similar to a previously reported case [6][6], with shared features of anterior ST-segment elevation and atypical inferior de Winter pattern T-waves (dWp). However, critical differences exist: this case had RCA subtotal occlusion with LAD collateral supply, whereas the reported case had total RCA occlusion without collaterals, leading to variations in ECG patterns and clinical outcomes.
Electrocardiographic manifestations during simultaneous LAD and RCA involvement are highly variable, depending on ischemic location and severity. ECG may show simultaneous anterior and inferior ST-segment elevation, or ST elevation from one vessel with a dWp from the other [7]. In multi-vessel ACS, the complex pathophysiology and the correlation between vessel occlusion and ECG ST-segment deviations are often unclear.
Simultaneous bilateral coronary artery events typically present as critical conditions [6] and are prone to severe complications like cardiogenic shock. Clinical data are limited, and specific management guidelines are lacking. Rapid restoration of culprit vessel flow to TIMI grade 3, preventing no-reflow, and stabilizing hemodynamics are imperative.
For STEMI complicated by cardiogenic shock, routine PCI of non-infarct-related arteries is not recommended as it may increase mortality or renal failure risk. Multivessel PCI decisions for unstable non-culprit lesions should be based on anatomical and clinical context, especially when the true culprit is unclear [8]. In ACS with collaterals, collateral flow can reduce infarct size and mortality but also alter surface ECG presentation. Atypical symptoms and ECG patterns may delay diagnosis, which is particularly hazardous in multi-vessel occlusion where the culprit lesion is difficult to identify, potentially delaying reperfusion [9][10]. Therefore, accurate diagnosis and management require integrating ECG findings with cardiac biomarkers, clinical timeline, and coronary anatomy.
4. Conclusion
It is critical to highlight the distinctiveness of acute coronary events involving both coronary arteries simultaneously and the complexity of ECG interpretation in the context of multivessel disease with CC involvement—these factors can easily lead to misidentification of the culprit vessel and subsequent clinical decision-making errors. Timely performance of coronary angiography and evidence-based clinical judgment are the cornerstones of management.
Video: PCI Imaging in "The Mystery of Anterior ST-Segment Elevation"
References
- Barros I, Narvaez A, Navarro A, Cardona C, Senior J. Aslanger Pattern: A Sign of an Acute Coronary Occlusion. Cureus. 2025 May 26;17(5):e84818. doi: 10.7759/cureus.84818. PMID: 40568275; PMCID: PMC12188695.
- Escabi-Mendoza J, Diaz-Rodriguez PE, Silva-Cantillo RD. Shark Fin Occlusive Myocardial Infarction ECG Pattern Post-cardiac Arrest Misinterpreted As Ventricular Tachycardia. Cureus. 2023 May 8;15(5):e38708. doi: 10.7759/cureus.38708. PMID: 37292562; PMCID: PMC10246928.
- Meyers HP, Bracey A, Lee D, Lichtenheld A, Li WJ, Singer DD, Kane JA, Dodd KW, Meyers KE, Thode HC, Shroff GR, Singer AJ, Smith SW. Comparison of the ST-Elevation Myocardial Infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI. J Emerg Med. 2021 Mar;60(3):273-284. doi: 10.1016/j.jemermed.2020.10.026. Epub 2020 Dec 9. PMID: 33308915.
- Guarnieri G, Mele D, Briguglia D, Medda M, Conte E, Bartorelli A, Andreini D. A STEMI Complicated by Cardiogenic Shock Due to Simultaneous Acute Thrombosis of Two Coronary Vessels in the 'Deadly Double Infarct Syndrome': A Case Report and Discussion of Literature. J Clin Med. 2024 Dec 10;13(24):7511. doi: 10.3390/jcm13247511. PMID: 39768439; PMCID: PMC11677721.
- Yamawaki M, Onuma Y, Nakano M, Muramatsu T, Nakatani S, Ishibashi Y, Ishimori H, Hirano K, Ito Y, Tsukahara R, Muramatsu T. Simultaneous occlusion of left anterior descending and left circumflex arteries by very late stent thrombosis: vascular response to drug-eluting stents assessed by intravascular ultrasound. Heart Vessels. 2015 Nov;30(6):824-9. doi: 10.1007/s00380-014-0545-0. Epub 2014 Jul 17. PMID: 25031154.
- Ahmed M, Abdul A. Simultaneous double coronary thrombosis in a 47-year-old male patient with acute myocardial infarction. Am J Case Rep. 2013 Oct 23;14:430-4. doi: 10.12659/AJCR.889556. PMID: 24175009; PMCID: PMC3809984.
- Tu CM, Hsueg CH, Chu KM, Cheng SM, Tsao TP. Simultaneous thromboses of double coronary arteries in a young male with antithrombin III deficiency. Am J Emerg Med. 2009 Nov;27(9):1169.e3-6. doi: 10.1016/j.ajem.2008.12.006. PMID: 19931780.
- 8、 Rao SV, O'Donoghue ML, Ruel M, Rab T, Tamis-Holland JE, Alexander JH, Baber U, Baker H, Cohen MG, Cruz-Ruiz M, Davis LL, de Lemos JA, DeWald TA, Elgendy IY, Feldman DN, Goyal A, Isiadinso I, Menon V, Morrow DA, Mukherjee D, Platz E, Promes SB, Sandner S, Sandoval Y, Schunder R, Shah B, Stopyra JP, Talbot AW, Taub PR, Williams MS. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025 Apr;151(13):e771-e862. doi: 10.1161/CIR.0000000000001309. Epub 2025 Feb 27. Erratum in: Circulation. 2025 Apr;151(13):e865. doi: 10.1161/CIR.0000000000001328. Erratum in: Circulation. 2025 Jun 24;151(25):e1098. doi: 10.1161/CIR.0000000000001346. PMID: 40014670.
- La Cognata O, Trimarchi G, Lo Savio A, Virga V, Andò G, de Gregorio C. Kounis syndrome in a patient with multivessel coronary artery disease and DRESS. Clin Case Rep. 2023 Mar 20;11(3):e7121. doi: 10.1002/ccr3.7121. PMID: 36950673; PMCID: PMC10025948.
- Traupe T, Gloekler S, de Marchi SF, Werner GS, Seiler C. Assessment of the human coronary collateral circulation. Circulation. 2010 Sep 21;122(12):1210-20. doi: 10.1161/CIRCULATIONAHA.109.930651. PMID: 20855668.