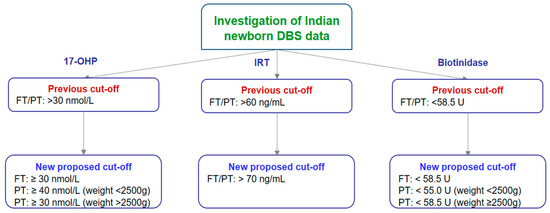
Neonatal deaths, which usually occur in the first week after delivery, account for nearly 75 percent of all deaths of children under 5 years of age. Prematurity, birth difficulties, infections, and birth defects are responsible for about 40 percent of these deaths. Although mortality rates have declined since 2000, access to quality healthcare remains a major problem for mothers and infants worldwide. In perspective, the present study aimed to establish clear biological reference intervals for 17α-hydroxyprogesterone (17-OHP), immunoreactive trypsinogen (IRT), and biotinidase in Indian neonates. The statistical analysis of data from up to 3200 dried blood spot (DBS) samples of Indian newborns provided valuable information for the new cut-off values in newborn screening (NBS) programs. We applied correlation analysis to fix the relationship for NBS parameters such as 17-OHP, IRT, and biotinidase. This study provided important information about the distribution and comparison of key cut-offs for biomarkers considering body weights and gestational age in the Indian newborn population for the first time, which can help healthcare experts make easier treatment decisions.
- 17α-hydroxyprogesterone
- biological reference interval
- biotinidase
- immunoreactive trypsinogen
1. Introduction
2. Materials and Methods
2.1. Collection and Analysis of 17-OHP, IRT, and Biotinidase Samples
2.2. Statistical Analysis
3. Results
3.1. Cut-Off Establishment for 17-OHP, IRT, and Biotinidase in Indian Newborns
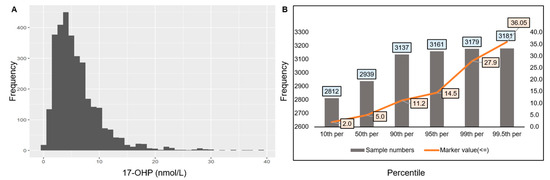
3.1.1. Cut-Off Establishment for 17-OHP
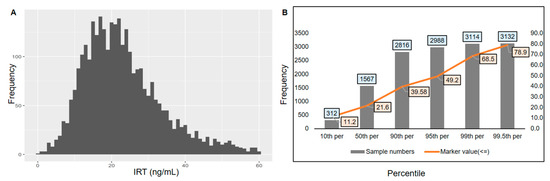
3.1.2. Cut-Off Establishment for IRT
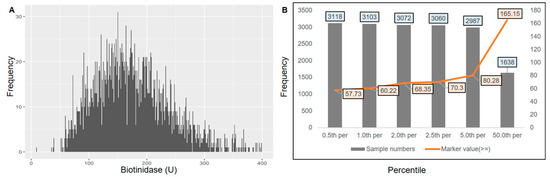
3.1.3. Cut-Off Establishment for Biotinidase
4. Discussion
5. Conclusions
This entry is adapted from: https://www.mdpi.com/2673-8430/4/3/21
References
- FDA-NIH Biomarker Working Group. Diagnostic Biomarker. In BEST (Biomarkers, Endpoints, and Other Tools) Resource; Food and Drug Administration: Silver Spring, MD, USA, 2020.
- Bodaghi, A.; Fattahi, N.; Ramazani, A. Biomarkers: Promising and Valuable Tools towards Diagnosis, Prognosis and Treatment of COVID-19 and Other Diseases. Heliyon 2023, 9, e13323.
- Ahmad, A.; Imran, M.; Ahsan, H. Biomarkers as Biomedical Bioindicators: Approaches and Techniques for the Detection, Analysis, and Validation of Novel Biomarkers of Diseases. Pharmaceutics 2023, 15, 1630.
- Rosa-Mangeret, F.; Benski, A.-C.; Golaz, A.; Zala, P.Z.; Kyokan, M.; Wagner, N.; Muhe, L.M.; Pfister, R.E. 2.5 Million Annual Deaths—Are Neonates in Low- and Middle-Income Countries Too Small to Be Seen? A Bottom-Up Overview on Neonatal Morbi-Mortality. Trop. Med. Infect. Dis. 2022, 7, 64.
- Marsden, D.; Bedrosian, C.L.; Vockley, J. Impact of Newborn Screening on the Reported Incidence and Clinical Outcomes Associated with Medium- and Long-Chain Fatty Acid Oxidation Disorders. Genet. Med. 2021, 23, 816–829.
- Rocha, J.C.; MacDonald, A. Dietary Intervention in the Management of Phenylketonuria: Current Perspectives. Pediatr. Health Med. Ther. 2016, 7, 155–163.
- Widaman, K.F. Phenylketonuria in Children and Mothers: Genes, Environments, Behavior. Curr. Dir. Psychol. Sci. 2009, 18, 48–52.
- Behrman, R.E.; Butler, A.S.; Healthy Outcomes (Eds.) Mortality and Acute Complications in Preterm Infants. In Preterm Birth: Causes, Consequences, and Prevention; National Academies Press: Washington, DC, USA, 2007.
- Pitt, J.J. Newborn Screening. Clin. Biochem. Rev. 2010, 31, 57.
- Crump, C. Preterm Birth and Mortality in Adulthood: A Systematic Review. J. Perinatol. 2020, 40, 833–843.
- Levy-Shraga, Y.; Pinhas-Hamiel, O. High 17-Hydroxyprogesterone Level in Newborn Screening Test for Congenital Adrenal Hyperplasia. BMJ Case Rep. 2016, bcr2015213939.
- Burdea, L.; Mendez, M.D. 21-Hydroxylase Deficiency. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024.
- Jha, S.; Turcu, A.F. Non-Classic Congenital Adrenal Hyperplasia: What Do Endocrinologists Need to Know? Endocrinol. Metab. Clin. N. Am. 2021, 50, 151–165.
- Momodu, I.I.; Lee, B.; Singh, G. Congenital Adrenal Hyperplasia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024.
- Wróbel, T.M.; Jørgensen, F.S.; Pandey, A.V.; Grudzińska, A.; Sharma, K.; Yakubu, J.; Björkling, F. Non-Steroidal CYP17A1 Inhibitors: Discovery and Assessment. J. Med. Chem. 2023, 66, 6542–6566.
- Newborn Screening for Cystic Fibrosis: Do We Need a Second IRT?—PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2065957/ (accessed on 14 August 2024).
- Ooi, C.Y.; Sutherland, R.; Castellani, C.; Keenan, K.; Boland, M.; Reisman, J.; Bjornson, C.; Chilvers, M.A.; van Wylick, R.; Kent, S.; et al. Immunoreactive Trypsinogen Levels in Newborn Screened Infants with an Inconclusive Diagnosis of Cystic Fibrosis. BMC Pediatr. 2019, 19, 369.
- Morrison, C.B.; Markovetz, M.R.; Ehre, C. Mucus, Mucins and Cystic Fibrosis. Pediatr. Pulmonol. 2019, 54, S84–S96.
- Canda, E.; Kalkan Uçar, S.; Çoker, M. Biotinidase Deficiency: Prevalence, Impact And Management Strategies. Pediatr. Health Med. Ther. 2020, 11, 127–133.
- Hymes, J.; Wolf, B. Biotinidase and Its Roles in Biotin Metabolism. Clin. Chim. Acta 1996, 255, 1–11.
- Tong, L. Structure and Function of Biotin-Dependent Carboxylases. Cell. Mol. Life Sci. 2012, 70, 863–891.
- Tippabathani, J.; Seenappa, V.; Murugan, A.; Phani, N.M.; Hampe, M.H.; Appaswamy, G.; Sadashiv Gambhir, P. Neonatal Screening for Congenital Adrenal Hyperplasia in Indian Newborns with Reflex Genetic Analysis of 21-Hydroxylase Deficiency. Int. J. Neonatal Screen 2023, 9, 9.
- Chen, H.-F.; Rose, A.M.; Waisbren, S.; Ahmad, A.; Prosser, L.A. Newborn Screening and Treatment of Phenylketonuria: Projected Health Outcomes and Cost-Effectiveness. Children 2021, 8, 381.
- Held, P.K.; Bird, I.M.; Heather, N.L. Newborn Screening for Congenital Adrenal Hyperplasia: Review of Factors Affecting Screening Accuracy. Int. J. Neonatal Screen 2020, 6, 67.
- Bereket, A. Editorial: Neonatal Screening for Congenital Adrenal Hyperplasia in Turkey. J. Clin. Res. Pediatr. Endocrinol. 2019, 11, 1–3.
- Kaye, C.I.; The Committee on Genetics. Newborn Screening Fact Sheets. Pediatrics 2006, 118, e934–e963.
- Torresani, T.; Grüters, A.; Scherz, R.; Burckhardt, J.J.; Harras, A.; Zachmann, M. Improving the Efficacy of Newborn Screening for Congenital Adrenal Hyperplasia by Adjusting the Cut-off Level of 17α-Hydroxyprogesterone to Gestational Age. Screening 1994, 3, 77–84.
- Hemmilä, I.; Dakubu, S.; Mukkala, V.-M.; Siitari, H.; Lövgren, T. Europium as a Label in Time-Resolved Immunofluorometric Assays. Anal. Biochem. 1984, 137, 335–343.
- Rock, M.J.; Mischler, E.H.; Farrell, P.M.; Bruns, W.T.; Hassemer, D.J.; Laessig, R.H. Immunoreactive Trypsinogen Screening for Cystic Fibrosis: Characterization of Infants with a False-Positive Screening Test. Pediatr. Pulmonol. 1989, 6, 42–48.
- Kirby, L.T.; Applegarth, D.A.; Davidson, A.G.; Wong, L.T.; Hardwick, D.F. Use of a Dried Blood Spot in Immunoreactive-Trypsin Assay for Detection of Cystic Fibrosis in Infants. Clin. Chem. 1981, 27, 678–680. Available online: https://academic.oup.com/clinchem/article-abstract/27/5/678/5666531 (accessed on 14 August 2024).
- Hart, P.S.; Hymes, J.; Wolf, B. Biochemical and Immunologic Characterization of Serum Biotinidase in Partial Biotinidase. Pediatr. Res. 1992, 31, 261–265.
- Wolf, B.; Heard, G.S.; Jefferson, L.G.; Proud, V.K.; Nance, W.E.; Weissbecker, K.A. Clinical Findings in Four Children with Biotinidase Deficiency Detected through a Statewide Neonatal Screening Program. N. Engl. J. Med. 1985, 313, 16–19.
- Yau, M.; Khattab, A.; Yuen, T.; New, M. Congenital Adrenal Hyperplasia. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000.
- Nimkarn, S.; Gangishetti, P.K.; Yau, M.; New, M.I. 21-Hydroxylase-Deficient Congenital Adrenal Hyperplasia. In GeneReviews®; Adam, M.P., Feldman, J., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.W., Amemiya, A., Eds.; University of Washington, Seattle: Seattle, WA, USA, 1993.
- Southern, K.W.; Mérelle, M.M.E.; Dankert-Roelse, J.E.; Nagelkerke, A. Newborn Screening for Cystic Fibrosis. Cochrane Database Syst. Rev. 2009, CD001402.
- Patadia, C.; Desai, D. A Child Born Late: Neonatal and Paediatric Compilations Related to Post-Dated Pregnancy. preprint 2023.
- Latif, S.; Aiken, C. Prolonged Pregnancy: Balancing Risks and Interventions for Post-Term Gestations. Obstet. Gynaecol. Reprod. Med. 2024, 34, 127–133.
- Neggers, Y.H. Gestational Age and Pregnancy Outcomes. In Pregnancy and Birth Outcomes; Intech: London, UK, 2018; ISBN 978-1-78923-243-1.
- Akanmode, A.M.; Mahdy, H. Macrosomia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024.
- Fallah, S.; Chen, X.-K.; Lefebvre, D.; Kurji, J.; Hader, J.; Leeb, K. Babies Admitted to NICU/ICU: Province of Birth and Mode of Delivery Matter. Healthc. Q. 2011, 14, 16–20.
- Woldeamanuel, G.G.; Geta, T.G.; Mohammed, T.P.; Shuba, M.B.; Bafa, T.A. Effect of Nutritional Status of Pregnant Women on Birth Weight of Newborns at Butajira Referral Hospital, Butajira, Ethiopia. SAGE Open Med. 2019, 7, 2050312119827096.
- Seghieri, G.; Anichini, R.; De Bellis, A.; Alviggi, L.; Franconi, F.; Breschi, M.C. Relationship between Gestational Diabetes Mellitus and Low Maternal Birth Weight. Diabetes Care 2002, 25, 1761–1765.
- Lewandowska, M. Maternal Obesity and Risk of Low Birth Weight, Fetal Growth Restriction, and Macrosomia: Multiple Analyses. Nutrients 2021, 13, 1213.
- Ornoy, A.; Becker, M.; Weinstein-Fudim, L.; Ergaz, Z. Diabetes during Pregnancy: A Maternal Disease Complicating the Course of Pregnancy with Long-Term Deleterious Effects on the Offspring. A Clinical Review. Int. J. Mol. Sci. 2021, 22, 2965.
- Honour, J.W. 17-Hydroxyprogesterone in Children, Adolescents and Adults. Ann. Clin. Biochem. 2014, 51, 424–440.
- Reddy, N.A.; Sharma, S.; Das, M.; Kapoor, A.; Maskey, U. Devastating Salt-Wasting Crisis in a Four-Month-Old Male Child with Congenital Adrenal Hyperplasia, Highlighting the Essence of Neonatal Screening. Clin. Case Rep. 2022, 10, e6010.
- Waugh, N.; Royle, P.; Craigie, I.; Ho, V.; Pandit, L.; Ewings, P.; Adler, A.; Helms, P.; Sheldon, C. Screening for Cystic Fibrosis-Related Diabetes: A Systematic Review. Health Technol. Assess. 2012, 16, 1–179.
- Farrell, P.M.; Rosenstein, B.J.; White, T.B.; Accurso, F.J.; Castellani, C.; Cutting, G.R.; Durie, P.R.; Legrys, V.A.; Massie, J.; Parad, R.B.; et al. Guidelines for Diagnosis of Cystic Fibrosis in Newborns through Older Adults: Cystic Fibrosis Foundation Consensus Report. J. Pediatr. 2008, 153, S4–S14.
- Cowan, T.M.; Blitzer, M.G.; Wolf, B. Technical Standards and Guidelines for the Diagnosis of Biotinidase Deficiency. Genet. Med. 2010, 12, 464–470.
- Saleem, H.; Simpson, B. Biotinidase Deficiency. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024.
- Kannan, B.; Navamani, H.K.; Jayaseelan, V.P.; Arumugam, P. A Rare Biotinidase Deficiency in the Pediatrics Population: Genotype–Phenotype Analysis. J. Pediatr. Genet. 2022, 12, 1–15.