Circulating tumor cells are cancer cells that detach from the primary tumor and enter the bloodstream. These cancer cells in the blood stream eventually result in secondary tumor growth referred to as metastasis. Research on circulating tumor cells is crucial because they can provide valuable insights into cancer progression and treatment response that enhances the patient outcomes. Findings from circulating-tumor-cell-based research can also shed light on cancer metastasis, drug resistance, and tumor evolution, ultimately benefiting the research community by advancing our understanding of cancer biology and guiding the development of innovative treatments.
1. Background
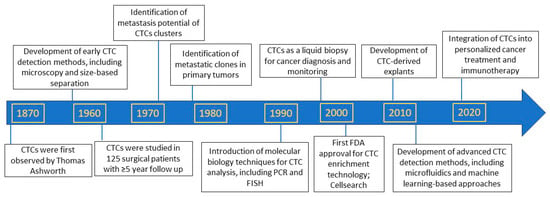
Preliminary observations of circulating tumor cells (CTCs) date back to the early 19th century, and Thomas Ashworth is credited for proposing their potential role in cancer metastasis. Ashworth observed that cancer patients’ blood contained tumor cells and suggested that these cells could migrate through the bloodstream to establish secondary tumors in distant organs. This observation formed the basis for the subsequent identification and characterization of circulating tumor cells (CTCs) as ‘micrometastatic seeds’ or ‘seeds of metastasis’. No significant breakthroughs were made for approximately a century following the initial discovery of circulating cancer cells. Nonetheless, the research community began paying attention to these circulating cancer cells in the late 1950s, and since then, CTC-based studies have undergone a fascinating evolution that continues to the present day (Figure 1). We now know that single CTCs can be sequenced, and large next-generation sequencing (NGS) data from multi-center studies can be generated to explore the process and progression of cancer from locoregional disease to widespread metastasis. The basic understanding is that CTCs are extravasated from the primary tumor into the bloodstream through a complex process, where they act as surrogates reflecting the characteristics of the tumor itself. The rarity of CTCs within the vasculature engendered uncertainty regarding their potential in mediating metastasis; however, it is now well established that even a single CTC possesses tumorigenic capacity and can serve as a metastatic source.
Figure 1. Important milestones in circulating-tumor-cell-based research [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18].
2. Discovery of Circulating Tumor Cells as Precursors of Metastasis
The discovery of CTCs as precursors of metastasis has been a transformative journey spanning over a century. In 1889, Stephen Paget first proposed the “seed and soil” hypothesis, suggesting that cancer cells travel through the bloodstream and grow in distant organs [
19]. The fundamental idea of the “seed and soil’ hypothesis was a metaphor comparing cancer cell migration to plant germination. Similar to the fact that seeds dispersed by a plant can only thrive in congenial soil, cancer cells traveling through the vasculature require a receptive environment to germinate and grow in distant organs. Although the hypothesis sufficiently illustrated the concept of distant growth, it initially lacked consideration [
20]. It was not until the mid-20th century that observational and experimental evidence emerged, demonstrating that cancer cells from primary tumors could spread to secondary sites through the circulation. Ashworth’s initial observation of epithelial cells in the blood of a dying cancer patient in 1869 suggested the basis for primary tumor-derived circulating cells [
1]. Following Ashworth’s observation, various studies reported tumor cells in the postmortem blood of patients with different cancers. A few studies also reported tumor cells in the blood collected from patients a few hours prior to death [
2]. The first study on CTCs in 125 surgical patients having different cancers with a long follow up of 5 years was evidenced in the year 1959 [
3]. Later, similar studies were conducted by several investigators to observe the dissemination of CTCs during and after operative procedures [
4,
5]. Fidler and Kripke experimentally demonstrated that metastasis results from pre-existing variant cells within a malignant tumor. They showed that clones derived in vitro from a parent culture of murine malignant melanoma cells varied greatly in their ability to produce metastatic colonies in the lungs upon intravenous inoculation into syngeneic mice. This study was a breakthrough in demonstrating the heterogenous nature of primary tumor and clonal selection during metastasis [
6]. Moving forward, the limited number of CTCs in the patients’ blood stalled the studies to demonstrate their metastasis initiating ability or tumorigenic potential. Firstly, and most importantly, the extensive availability of cells is imperative for their functional and biological characterization. The scarcity of CTCs in the bloodstream historically presented both opportunities and challenges for researchers. Scientific community shifted their focus on enrichment of CTCs and to date different antibody-based positive and negative enrichment technologies [
7] and microfluidics-based isolation methods (
Table 1) are available. Further milestones uncovering the metastasis initiating potential of CTCs are evidenced due to the availability of better CTC enrichment technologies. The growth of xenograft tumors upon implantation of CTCs enriched from the peripheral blood of human patients, coupled with the association of high CTC numbers in circulation with disease recurrence in patients, provided conclusive evidence that CTCs are indeed the seeds of metastasis [
8,
21,
22,
23,
24,
25,
26,
27]. Further, to assess the utility of CTCs in forecasting patient outcomes and evaluating their predictive value as biomarkers, numerous studies have been conducted that involve detecting and enumerating CTCs in cancer patients, followed by tracking their clinical progress [
9,
10]. This has enabled researchers to explore the relationship between CTCs and patient prognosis, and to determine the accuracy of CTCs as indicators of disease progression.
3. Circulating Tumor Cells as Biomarkers to Predict Patient Prognosis
Development of the CellSearch system in the early 2000s and the U.S. Food and Drug Administration approval in 2004 enabled the detection, enumeration, and characterization of CTCs in numerous clinical trials involving breast, prostate, and colorectal cancer patients [
11,
41]. Since then, numerous studies have consistently shown that CTCs are associated with poor prognosis and can predict disease recurrence. This technology advancement elevated liquid biopsy in cancer research wherein CTCs from the peripheral blood of patients with different cancer types were analyzed to predict the prognostic effect. For example, a seminal study in breast cancer patients found that high CTC counts were linked to decreased overall survival [
42]. Similarly, in colorectal cancer, high CTC counts have been linked to worse overall survival [
43,
44]. Clinical utility of CTCs as disease prognosticators were shown in both castration resistant and sensitive prostate cancer patients [
45]. Likewise, positive CTC counts were shown to be common in advance gastric cancer patients who presented with diffused histologic tumor types and distant metastases. Further, the study also showed that progression-free survival of CTC-positive patients was significantly shorter than that of CTC-negative patients indicating the independent prognostic potential of CTCs in gastric cancer [
46]. The major drawback of the Cellsearch system is the enrichment of CTCs based on the expression of epithelial cellular adhesion molecule (EpCAM) [
23]. In certain cancers like non-small-cell lung cancer (NSCLC), EpCAM expression will be low due to epithelial to mesenchymal transition, and the Cellsearch system may not be the suitable platform to enrich and enumerate CTCs. Owing to the limitations of the Cellsearch system, the detection and analysis of CTCs have become more sophisticated with advancements in non-epitope-dependent technologies like microfluidics and filtration methods. Several groups including ours utilized non-epitope-dependent technologies to study the biomarker potential of CTCs in predicting prognosis of cancer patients. Using a size-based microfiltration method, one study demonstrated the prognosis of head and neck squamous cell carcinoma patients in correlation to CTC numbers [
47]. Similarly, the prognostic value of CTCs was demonstrated in NSCLC patients and screening subjects [
48,
49,
50]. Additionally, C-X-C chemokine receptor type 4 (CXCR4) expression on circulating pan-cytokeratin-positive cells was shown to be associated with survival in patients with advanced non-small-cell lung cancer [
51]. Another major advantage of non-epitope-dependent technologies is the identification of multi-phenotypic subtypes of CTCs and CTC clusters or microemboli [
48,
49]. For instance, CTC clusters are shown to be more aggressive phenotypes than individual CTCs [
52]. CTC clusters are defined as two or more group of tumor cells with an intact nucleus [
25]. Although less abundant in circulation, CTC clusters possess higher metastatic potential and elevated expression of epithelial-to-mesenchymal transition markers and stemness genes compared to individual CTCs [
11,
53,
54,
55]. There are two types of CTC clusters: homotypic and heterotypic. Homotypic clustering occurs through adhesion molecule interactions (e.g., CD44, cadherin, desmoglein, ICAM1, and desmocollin), which stabilizes clusters and activates downstream pathways that enhance invasiveness and migration [
54,
56,
57,
58]. Patients with elevated individual CTC counts exhibit significantly poorer overall survival, and this association is further exacerbated in patients with higher CTC cluster levels [
48,
59,
60]. On the other hand, CTC heterotypic clusters are characterized as tumor cells forming clusters with other cell types such as leukocytes, neutrophils, fibroblasts, platelets, and myeloid derived suppressor cells [
61,
62,
63,
64,
65]. Patients with CTC–leukocyte clusters have shown worse overall survival compared to patients without CTC–leukocyte clusters [
66]. CTCs clustered with neutrophils and fibroblasts have been shown to have higher cell division and invasion and migration, respectively [
61,
62]. Platelets clustered with CTCs are believed to aid them in escaping from immune surveillance [
67]. Furthermore, analysis of CTCs has also revealed insights into tumor biology, such as the presence of putative cancer stem cells and circulating tumor microemboli [
68]. Overall, the use of CTCs as biomarkers has the potential to revolutionize personalized cancer care, and ongoing research is exploring new frontiers in CTC analysis, including their potential use as liquid biopsies and predictors of cancer relapse.
4. Circulating Tumor Cells as Biomarkers to Predict Anti-Cancer Therapy Responses
CTCs have potential uses beyond cancer diagnosis and prognosis. CTCs may serve as a means to monitor cancer minimal residual disease after treatment. CTCs offer a non-invasive way to assess cancer progression and treatment response, potentially reducing the need for invasive biopsies. As outlined below, a variety of neoadjuvant or adjuvant anti-cancer therapies have been tailored based on the expression and mutational analysis performed in CTCs (Figure 2). Even the response to tailored treatment strategy has been shown to corelate with CTCs at baseline, during therapy and post-therapy.
Figure 2. Anti-cancer treatment strategies based on CTC expression and mutational analysis. Created using Biorender (
https://biorender.com accessed on 3 January 2024).
5. Molecular and Genetic Characterization of Circulating Tumor Cells beyond Enumeration to Identify Actionable Mutations
The analysis of CTCs has evolved beyond mere enumeration, with advances in technologies enabling molecular and genetic characterization. This allows for the detection of specific genetic mutations, the expression of surface proteins, and analysis of gene transcripts in CTCs. Thanks to cut-ting-edge technologies, we can now analyze CTCs at the genetic, transcriptomic, and proteomic levels, which has helped bridge the knowledge gap in understanding the metastasis process and tailor precision medicine.
6. Real World Evidence by Circulating-Tumor-Cell-Based Clinical Trials
CTCs have emerged as a promising biomarker for cancer diagnosis and monitoring. Several clinical trials have investigated the clinical utility of CTCs in various cancer types to accumulate real world data or evidence. Accumulated findings suggest that CTC-based clinical trials may lead to improved cancer diagnosis and treatment strategies and CTC-based biomarkers may help optimize cancer treatment and improve patient outcomes.
This entry is adapted from the peer-reviewed paper 10.3390/cancers16040816