1. Introduction
Non-valvular atrial fibrillation (AF) is the most common cardiac arrhythmia and its prevalence is growing as consequence of aging [
1]. In Western countries, the lifetime risk of developing AF is about 15% [
2], and 30% of all ischemic strokes are due to AF [
3].
Vitamin K antagonists (VKAs) have shown their ability to decrease ischemic stroke by about 60%; these results were obtained with an increased rate of major bleeding [
4]. In the last decade, direct oral anticoagulants (DOACs) have shown a similar efficacy, but with a lower risk of intracranial hemorrhage (ICH) when compared to VKAs [
5,
6,
7,
8].
Intracranial hemorrhage (ICH) represents the most serious complication of anticoagulant therapy, despite the therapy’s effectiveness.
Cerebral amyloid angiopathy (CAA) is one of the main risk factors for spontaneous ICH [
9], and this risk is highly increased by age and antithrombotic therapies [
10]. Moreover, CAA can be manifested with clinical features simulating TIA or stroke in AF patients [
10], pushing clinicians to rapidly start VKAs or DOACs, increasing the risk of ICH if the diagnosis of CAA is unknown.
2. CAA Is Generally Asymptomatic for Several Years
The main manifestations are lobar cerebral hemorrhage, cognitive decline, transient focal neurological episodes (TFNEs) and pseudotumoral presentations (Table 1).
Lobar cerebral hemorrhages are often accompanied by headache, focal neurological signs, seizures, or alterations in the state of consciousness [
26].
CAA is usually associated with lobar ICH, but not with deep cerebral or cerebellar ICH (
Figure 1), which, instead, are more typical of hypertensive microangiopathy [
9,
27] (
Figure 2).
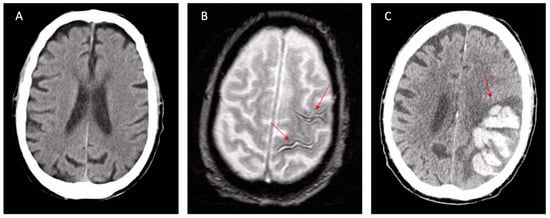
Figure 1. Final diagnoses of probable CAA according to the Boston Criteria 2.0. 84-year-old patient presenting with a TFNE (transient right hemiparesis and loss of speech for several minutes) and first detection of atrial fibrillation. (A) Apparently normal NECT. Oral anticoagulation was started for the secondary prevention of cardioembolism (the TFNE was misinterpreted as cardioembolic TIA). (B) MRI scan 10 days after the presentation showed signal loss in the left pre-central and central sulcus in T2* sequences (arrows), corresponding to “old” superficial siderosis. Oral anticoagulation was not interrupted based on CHA2DS2-VASc/HASBLED calculation. (C) Evolution with parenchymal left hematoma after few days (arrow). Abbreviations: NCET, non-enhanced computed tomography; CAA, cerebral amyloid angiopathy; TFNEs, transient focal neurological episodes; TIA, transient ischemic attack.
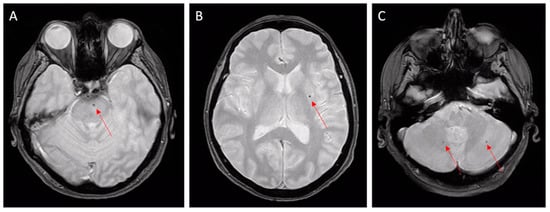
Figure 2. Hypertensive microangiopathy. Brain MRI, axial T2 gradient-echo images. Red arrows show microbleeds in the brain stem (A), left basal ganglia (B), and cerebellum (C). Deep localizations are typical features of hypertensive microbleeds.
Cognitive decline is another clinical presentation and it may overlap with Alzheimer’s disease [
28]. CAA-related cognitive impairment usually precedes the occurrence of ICH [
29].
TNFEs are usually associated with subarachnoid hemorrhages (SAHs) at the cerebral convexity [
15,
28,
30]. These events are described as recurrent and stereotyped episodes of sensory, visual, motor, or phasic focal neurological deficits. They are often indistinguishable from a transient ischemic attack (TIA) and, therefore, they are also defined as TIA-LIKE [
28,
31] or TIA-MIMIC [
29].
TNFEs are usually associated with acute subarachnoid hemorrhages (SAHs) at the cerebral convexity [
15,
28,
30,
32], especially in the central sulcus [
33] or sub-acute/chronic cortical bleeding named cortical superficial siderosis (cSS) [
34]. Their prevalence spreads from 14% of patients diagnosed with probable CAA in a multicenter cohort of 172 patients [
35] to 48% of a recent review and meta-analysis [
36], representing, therefore, a major clinical differential diagnosis.
Noteworthily, TFNEs often occur in patients without pre-existing cognitive deficits [
37].
Finally, other forms are associated with an intense focal cerebral inflammatory reaction (Figure 3).
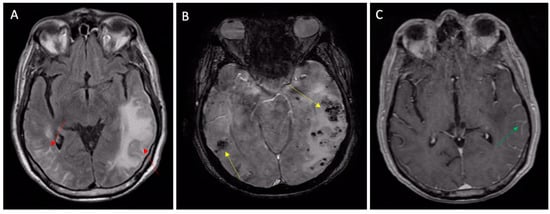
Figure 3. Inflammatory CAA presenting with TIA-MIMIC (transient aphasia). (A) MRI FLAIR sequences showing vasogenic edema (left arrow) and leptomeningeal inflammatory hyperintensities (right arrow); (B) susceptibility-weighted imaging MRI showing subcortical microbleeds (yellow arrows) and (C) leptomeningeal post contrast enhancement (green arrow) on T1 sequences.
These are known as “Cerebral Amyloid Angiopathy-Related Inflammation”, and are characterized by pseudotumoral vasogenic edema [
15] or pseudoarteritic vascular alterations, also named inflammatory angiitis linked to beta-amyloid [
14,
38].
3. Treatment/Management
Currently, no specific treatment can change the course of the disease. Consequent management is often based on the presenting symptoms [
39]. The acute management of patients with CAA-related ICH is similar to other causes of spontaneous ICH. Attention to blood pressure and intracranial pressure is essential. When surgical intervention is performed, the mortality risk is largely unchanged compared to other types of ICH. Intraventricular hemorrhage and an age greater than 75 are associated with a worse prognosis. Moreover, CAA-related ICH is frequently recurrent. Because of this high rate, clinicians typically avoid antiplatelet agents and anticoagulants when a strong indication for anticoagulation is not present [
39]. In the PROGRESS trial, blood pressure control has been associated with mortality benefits, even though CAA does not seem to be largely driven by hypertension, with a risk reduction of 77% for CAA-related ICH when blood pressure was controlled [
40]. For those presenting with inflammatory forms of CAA, the optimal treatment remains to be defined [
41]. Rapid clinical and radiologic responses have been reported using steroids alone or in conjunction with other immunosuppressive drugs, such as cyclophosphamide [
15]. Other immunosuppressive medications have also been associated with benefits, including mofetil, mycophenolate, and methotrexate [
42].
4. Diagnosis of CAA
As stated up above, CAA can behave as a Great Pretender, simulating Alzheimer disease, vascular dementia, TIA or stroke, brain cancer, or brain vasculitis. The clinical features of CAA are, therefore, misleading and may push clinicians toward false diagnoses.
According to Boston Criteria 2.0, CAA should be suspected primarily in patients older than 55 years with a history of single or recurrent lobar hemorrhage and/or superficial siderosis without alternative explanation [
43].
Presentation with cognitive decline or dementia is frequent in elderly people but it is not specific. Patients with gradual decline are more likely associated with microhemorrhages, lobar lacunas, microinfarcts, and chronic leukoencephalopathy [
39]. Stepwise cognitive decline is linked to single or recurrent lobar ICH, while rapidly progressive decline should raise suspicion for cerebral-amyloid-angiopathy-related inflammation [
15].
The suspicion of TFNEs should arise from recurrent and stereotyped neurological deficits in elderly people, including transient episodes of smoothly spreading paresthesia, numbness or weakness, typically lasting from seconds to minutes, and usually resolving over a similar period [
18].
A non-enhanced brain CT scan (NECT) is often carried out on suspicion of dementia or transient neurological deficits. In CAA patients, NECT shows a prevalence of moderate–severe Fazekas score leukopathy in 53% of subjects [
44], a high grade of peri-vascular spaces (PVSs) located in the centrum semiovale and basal ganglia in 56%, and lacunar infarcts in 30%. Notably, these features are relevant but nonspecific, being commonly related to age, hypertension, and diabetes [
45]. Consequentially, a CT scan is simply not useful in the diagnosis of CAA.
A brain MRI is superior to NECT in detecting typical imaging markers of CAA, such as subcortical cerebral microbleeds (CMBs), superficial siderosis, convexity SAH, and lobar hemorrhages [
36] (
Figure 1 and
Figure 2). Gradient-echo T2* sequences and susceptibility-weighted sequences are fundamental in MRI protocols to achieve adequate diagnosis; their absence can lead to misdiagnoses, so they are recommended in the study of cognitive impairment and for the proper differentiation of brain mass effect [
15].
Although the definite diagnosis of CAA is autoptic, clinical criteria have been validated and can assist the clinician in diagnosis. The new released Boston criteria 2.0 were recently proposed in 2022 to better include leptomeningeal and white matter characteristics in the diagnoses of probable and possible CAA [
43]. The Boston criteria 2.0 consist of combined clinical, imaging, and pathological parameters. It is important to note that a CAA diagnosis is an exclusion diagnosis.
5. Differential Diagnosis
Neuroimaging is fundamental to tailoring diagnosis. Gradient-echo (GE) T2*-weighted MRI and susceptibility-weighted (SW) MRI enable the highly accurate detection of CMBs, superficial siderosis, and small superficial hematomas that are hardly detectable using conventional NECT and MRI. However, these small round or linear T2* and SW hypointense lesions, pathologically representing the focal hemosiderin deposition associated with previous microhemorrhages, are also described in multiple conditions. The clinical context and the patient’s history could lead to the correct diagnosis.
A major cause of cerebral hematoma results from bleeding-prone small vessel diseases in hypertensive arteriopathy (including lipohyalinosis and arteriolosclerosis). In these patients, microbleeds are often localized in deep basal ganglia or cerebellar nuclei (Figure 2).
Brain trauma can lead to diffuse axonal injury with a typical subcortical and corpus callosum T2* micro lesion pattern [
46].
Hemodialysis patients have both a high prevalence of CMBs, of 19.3–35%, and much higher incidence of strokes (particularly ICH), than the general population [
47].
Moreover, intravascular lymphoma can mimic inflammatory CAA [
48].
Other important differential diagnoses mimicking CMBs on gradient-echo T2*-weighted MRI and SW MRI are hemorrhagic metastases, multiple cerebral cavernous malformations, radiation-induced vasculopathy, neurocysticercosis [
39], microsusceptibility changes on a brain MRI in critically ill patients on mechanical ventilation/oxygenation [
49], and brain microbleeds after orthotopic liver transplantation [
50].
Remarkably, in critical cardiology care settings, neurological complications mimicking CAA are frequent but generally oblivious. Infective endocarditis is a frequent cause of septic-embolus-related CMBs, superficial siderosis, and lobar hematomas [
51] (
Figure 4).
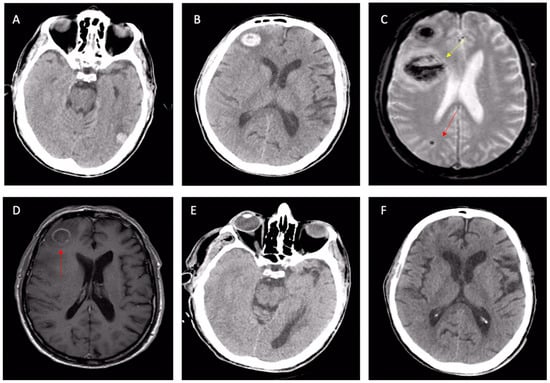
Figure 4. Cerebral involvement from confirmed bacterial endocarditis. (A,B) NECT showing left-temporal and right-frontal atypical hematomas linked with suspected CAA or cavernomas, according to radiologists. Same patient: second-line T2* brain MRI (C) with a further frontal lesion (yellow arrow) and subcortical microbleed (red arrow); the first two lesions are shown with signal loss in T2* sequences. The T1 post-contrast MRI (D) with ring enhancement (red arrow) raised the suspicion of an infective lesion. Control NECT after 3 weeks of antibiotic therapy (E,F): the complete disappearance of both frontal and temporal lesions, confirming cerebral emboli from endocarditis. Abbreviations: NCET, non-enhanced computed tomography; CAA, cerebral amyloid angiopathy.
In this setting, NECT rapidly excludes large hemorrhages in patients with infective endocarditis, but MRI accurately distinguishes the whole spectrum of brain lesions, including small ischemic lesions, microbleeds, superficial siderosis, and microabscesses [
52]. Finally, cerebral microbleeds are common in patients with left-ventricular assist devices [
53,
54], after heart surgery [
55], or after tacrolimus treatment for lung transplantation [
56].
6. Implications of a Missed Diagnosis
Although the diagnosis is quite simple in typical cases of lobar ICH, the major difficulties concern patients with cognitive impairment or TFNEs (
Figure 1 and
Figure 2). Indeed, TFNE patients have symptoms almost indistinguishable from TIA and often have other confounding comorbidities (AF, atherosclerosis, arterial hypertension, diabetes mellitus). Furthermore, a brain CT has a low sensitivity for detecting the typical elements of CAA, such as subcortical microbleeds, superficial siderosis, and chronic hemosiderin stores [
57]. SAH is visible on a brain CT only in the first days after its appearance. A brain MRI is extremely sensitive and specific [
57], but rarely prescribed on suspicion of TIA in real-life settings.
In patients with TFNE and concomitant AF, a misdiagnosis can have catastrophic consequences [
24,
58] (
Figure 1). Indeed, studies have suggested a significant increase in the risk of spontaneous ICH within weeks or months of the clinical onset of CAA [
24], with potentially devastating consequences when anticoagulant therapy is started. Even in patients with previous atraumatic lobar ICH, the risk of spontaneous hemorrhagic recurrence is particularly high [
59], and this risk becomes prohibitive in patients exposed to oral anticoagulant therapy (OAT) [
60].
This entry is adapted from the peer-reviewed paper 10.3390/jcm12247704