Olfactory dysfunction affects approximately 20% of the population globally, with incidence increasing over the age of 60. The pathophysiology is complex, not yet fully understood, and depends on many factors, including the underlying cause. Despite this, the present literature on olfaction is limited due to significant heterogeneity in methodological approaches. This has resulted in limited effective treatments available for olfactory dysfunction. Medications for olfactory dysfunction can be administered locally (directly to the olfactory epithelium) or systemically (orally or intravenously). There are various methods for local drug delivery to the olfactory epithelium (nasal drops, nasal sprays, atomisers, pressured meter-dosed inhalers, rinses, and exhalation delivery systems).
1. Introduction
Topical drug delivery devices can be categorised into “high volume” devices that deliver at least 50 mL into the nostrils (e.g., squeeze bottles and squirt system) and “low volume” devices, such as nasal sprays or nasal drops.
When delivering medications topically for olfactory dysfunction, the medications need to reach the olfactory epithelium in the olfactory cleft. This is challenging, as the olfactory epithelium is only a few millimetres wide and approximately 7 cm away from the nasal vestibule on average [
6]. Along the pathway from the vestibule to the olfactory epithelium lie several intranasal structures that can obstruct medication delivery. To treat olfactory loss in CRS, topical medications applied need to directly target the olfactory cleft, thus improving intrinsic olfactory function. The medications also need to reduce sinonasal tissue inflammation, thus alleviating obstructive olfactory dysfunction and increasing the delivery of other medications directly to the olfactory cleft. Thus, the main challenge is ensuring that the delivery method can deliver medication to this small area to maximise its therapeutic effect.
Several established methods of administering medication to olfactory cleft have been developed, such as nasal sprays, nasal drops using various sitting/lying positions, rinses, atomisers, and directly applying medication with endoscopic guidance.
2. Nasal Sprays
Nasal sprays have been used for many decades and are the most common way of administering drugs to the olfactory epithelium. They function by aerosolising the drug and transporting it to the nasal epithelium. The most common types of spray pumps are pressurised metred-dose (pMDIs) or pressurised aerosols, single- and duo-dose spray devices. They both deliver similar doses of medication per spray—around 100 mL (range 25–200 mL) per spray.
The characteristics of a device/spray that contains the drug have significant implications in terms of effects, as droplet size and spray angle play a significant role in effective delivery [
7]. For example, larger droplet size and a wider spray angle increase the deposition in the nasal vestibule. Current data on the effect of positioning, sniffing, inhaling, or blowing prior to drug administration on the olfactory cleft are not conclusive. Benninger et al. conducted a systematic review to create guidance for patients to optimise drug delivery of intranasal corticosteroid sprays for allergic and nonallergic rhinitis [
8]. These guidelines include holding the head in the neutral position, clearing the nose of any mucus, inserting the nozzle into the nostril, and spraying laterally—away from the septum to avoid the potential for epistaxis. Following application, the authors recommend gently inhaling and breathing out through the nose to maximise delivery [
8].
However, no such guidance exists for the use of intranasal sprays for olfactory dysfunction. Previous studies demonstrated that most of the liquid delivered using intranasal sprays only reaches the ventral part of the nasal cavity, the largest portion being deposited on the anterior surface of the inferior turbinate [
9,
10,
11], limiting its therapeutic effect. Heilmnann et al. found that two-thirds of patients being treated with local application of corticosteroids via nasal sprays experienced little to no improvement in olfactory dysfunction compared to systemic corticosteroids [
12]. They suggested that it could be due to the drug not effectively reaching the olfactory cleft or that local steroids are not as effective as systemic steroids.
Compared to other methods of intranasal drug delivery, nasal sprays are easy to use and have a reduced cost. However, the ability of nasal sprays to reach proximal areas of the sinonasal mucosa is limited, such as sinus cavities in CRS patients after endoscopic sinus surgery (ESS). Muenkaew et al. conducted a randomised trial comparing sinonasal corticosteroid distribution using nasal sprays and nasal irrigations in 40 CRS patients. They found that nasal sprays were inferior to irrigations in reaching the maxillary and anterior ethmoid sinuses when analysed with fluorescein dye during ESS. Both methods had limited fluorescein staining of the frontal and sphenoid sinuses [
13].
3. Nasal Drops with Various Head Positions
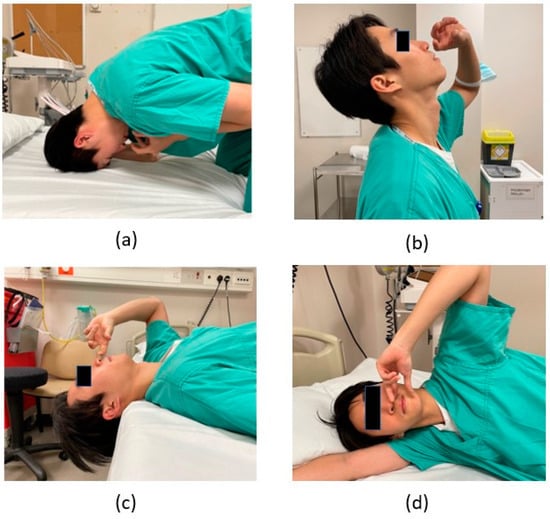
Nasal drops are another common method of delivering topical drugs intranasally, utilising various positions and gravity to transport liquid to the olfactory epithelium. There are several different head positions to improve the use of nasal drops, such as the head back position (HBP), lying head back position (LHB or Mygind), the head down and forward position (HDF), and the Kateiki position. These positions have been demonstrated in
Figure 1. However, some of these head positions may be uncomfortable for the patient, which may decrease compliance [
14,
15] and the effectiveness of the drug.
Figure 1. Various positions to apply medication into the nose. (a) Head down and forward position (HDF); (b) Head back position (HBP); (c) Lying head back (LHB); (d) Kateiki.
Of the mentioned head positions, the HBP is the simplest to perform but has been shown to have a nasal drop distribution primarily to the nasal floor, reducing its effectiveness. The LHB and HDF positions have better distribution, with medication reaching the middle meatus and sphenopalatine area [
15,
16,
17]. The Kateiki position is a method of intranasal steroids that Japanese researchers first described in research with cadaveric heads, with Kateiki meaning ‘comfortable’ [
16,
17,
18]. In this position, subjects lie on their sides with their heads tilted and chins turned upwards—a link to a video demonstrating how to perform the Kateiki position can be found in the
Supplementary Material. It has been shown in research conducted that this comfortable position can effectively deliver topical treatments to the olfactory epithelium [
18]. Mori et al. found that nasal drops reached the olfactory cleft in 96% of the decongested cases and 75% of the cases that had not been decongested. They hypothesised that this might indicate more effective therapies using these methods [
18]. Milk et al. compared the LHB position and the Kateiki position, showing that both positions were effective in delivering nasal drops onto the olfactory cleft [
19].
When deciding which position to use for the administration of nasal drops, it is important to consider patient preference to ensure compliance.
4. Rinses/Irrigation
Nasal irrigation/rinses are delivery methods of drugs dissolved in either hypotonic, isotonic, or hypertonic solution into the nose using plastic bottles or syringes. Commonly available products for nasal irrigation include the Neilmed® Sinus Rinse™ system.
No studies have been conducted on analysing the efficacy of irrigation systems in delivering medication specifically to the olfactory cleft. Previous studies suggested that corticosteroid nasal irrigation does not increase the quality of life or grant additional benefits when compared to nasal saline irrigation. These studies were limited by design, heterogeneity of surgical practice, short follow-up, and underpowered analyses [
20,
21]. Harvey et al. found that in diffuse or patchy chronic rhinosinusitis, the use of nasal irrigation compared with simple nasal spray had greater improvement in nasal blockage, less inflammation, lower overall symptoms on questionnaires, and greater radiological disease suppression. Furthermore, no patients reported medication-associated reactions [
22]. Other studies did not report any symptoms of adrenal suppression after 6 months of corticosteroid nasal irrigation unless used with other corticosteroid preparations, such as pulmonary inhalers [
23].
Therefore, high-volume nasal irrigation appears to improve nasal symptoms when compared to conventional nasal sprays. However, they do pose a potential risk of adrenal axis suppression in at-risk patient populations. In addition, studies have shown that patients receiving corticosteroids via nasal saline irrigation post-ESS experienced facial pain/pressure, delayed nasal drainage, and ear symptoms.
5. Atomisers
Intranasal Mucosal Atomisation Devices (MAD) atomise medications into particles with a size as small as 30 to 100 μm, increasing the surface area for absorption [
24].
There is conflicting evidence on the effectiveness of atomisers in comparison with nasal drops. A study reported that using the MAD in the LHB position is more effective in delivering medication all around the sinuses and the olfactory cleft compared with the HDF position [
25]. However, Cannaday et al. showed that using nasal drops in the Vertex to Floor (VF) position was more effective in delivering medication to the olfactory cleft than the atomiser (Wolf-Tory MADomizer) [
26].
6. The Exhalation Delivery System (OptiNose)
This is a new drug delivery technology that uses exhaled breath to deliver powder or liquid medications. The device prevents potential lung toxicity by avoiding lung deposition. It consists of a mouthpiece and a sealing nosepiece to be placed into a single nostril. The user then exhales through the mouthpiece, which elevates the soft palate and transfers pressure from the mouth to the nose. The air travelling from the mouth enters the device via the mouthpiece, and this way, the powder or liquid can travel around the nasal cavity. The positive pressure created in the nose by the OptiNose device expands the nose that is tightened by inflammation versus sniffing, which is a negative pressure system [
27,
28].
The OptiNose device has been shown to deposit drugs deeper, more broadly, and posteriorly where polyps originate, with less drip out when compared to conventional sprays [
29]. Multiple studies have shown that steroids delivered via OptiNose were an effective way of treating nasal polyps and improved nasal blockage, discomfort, rhinitis, and sense of smell [
30,
31,
32]. However, these studies did not investigate delivery to the olfactory cleft specifically.
7. Direct Administration under Endoscopic Guidance
Topical medications can be applied directly to the olfactory epithelium using endoscopic guidance. Medications such as platelet-rich plasma (PRP) can be injected directly into the olfactory epithelium or impregnated into dissolvable matrices/sponges such as Gelfoam [
33].
The benefits of adopting such a method are that the clinician can ensure the therapeutic medication will interact directly with the olfactory epithelium. However, this requires patients to attend hospital appointments for an experienced clinician to apply this into their nose. Therefore, it may not be suitable for medications that require frequent/daily applications to exert the desired therapeutic effect for olfactory dysfunction.
This entry is adapted from the peer-reviewed paper 10.3390/jcm12237387