Borrelia burgdorferi sensu lato (B. burgdorferi s.l.), which is predominantly spread by ticks, is the cause of Lyme disease (LD), also known as Lyme borreliosis, one of the zoonotic diseases affecting people. In recent years, LD has become more prevalent worldwide, even in countries with no prior records. The aptamer is an advanced technology with the potential for Borrelia antigen detection. Notably, combining the latest technology with the aptamer could enhance test sensitivity and detection limits and reduce the time required to complete the assay. Furthermore, the test can function alone or complement the conventional serological test practiced in most laboratories. In summary, a fast and convenient assay may facilitate the diagnosis of the fever-like symptom possibly caused by Lyme Borrelia infection.
1. Introduction
Lyme disease (LD), or Lyme borreliosis, is caused by a bacterial infection from
Borrelia burgdorferi sensu lato (
B. burgdorferi s.l.). This vector-borne zoonotic disease is primarily spread by ticks from the genus
Ixodes. The typical clinical manifestation of early infection is erythema migrans (EM) rash at the site, which occurs in >80% of patients in both Europe and the United States [
1]. LD symptoms may range from asymptomatic to severe and develop into encephalitis and arthritis without prompt treatment. Other non-specific symptoms include fever, malaise, and myalgia; hence they are often misdiagnosed or left untreated. Currently, LD is prevalent in the United States and Europe [
1], but diagnosing LD has become challenging as clinical manifestations vary between
B. burgdorferi genospecies and disease progression differs between patients [
2,
3,
4]. For example, rheumatological manifestations of LD are common in North America, while neurological manifestations are customary in Europe. In addition, acrodermatitis chronica atrophicans and lymphocytomas, usually caused by
Borrelia afzelii or
Borrelia garinii, are common in Europe and Asia but extremely rare in the United States [
5,
6]. In the United States, the new species
Borrelia mayonii was recognized in the Upper Midwest region [
7].
2. Current Guidelines for LD Diagnostic Test
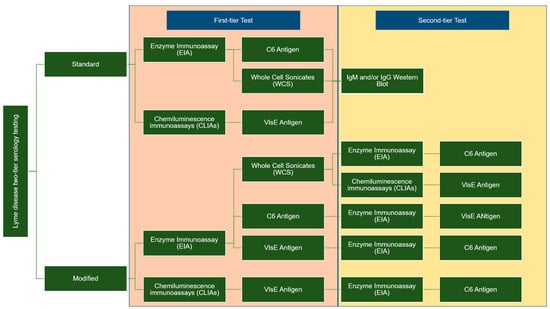
Two types of enzyme immunoassay, known as standard or modified, two-tiered serology testing (STTT/MTTT), are used to detect immunoglobulin (IgM or IgG). These methods differ in terms of the second confirmation assay; the STT uses western blotting, whereas the second enzyme immunoassay (EIA) is utilized for MTT when the sample is positive or ambiguous.
Figure 1 summarises the difference between the two-tier STTT and MTTT testing [
29,
30,
31,
32].
Figure 1. Differences between STTT and MTTT: Two-tier testing methods for LD diagnosis.
The STTT sensitivity for LD is less than 50% in early localized infections, whereas the sensitivity can reach up to 100% in the late stages of the disease. The MTTT is consistent and more sensitive in early localized LD than STTT and demonstrated similar sensitivity in detecting late infections and specificities to STTT [
33]. The two-tier testing is sufficient to rule in LD among patients who have tested positive in the early stages, but the tool has low predictive value to rule out LD, which necessitates retesting after 30 days [
34]. Nevertheless, LD sensitivity in recovering patients treated at stage 1 remained low after 30 days. Resultantly, the diagnosis and treatment of early localized LD solely depend on the clinical symptoms of individuals with a history of exposure to black-legged ticks.
Early LD can be difficult to diagnose, as some individuals with localized
B. burgdorferi infections do not have an EM rash and may exhibit symptoms similar to those of other diseases. As both STTT and MTTT cannot distinguish between active and past infection,
B. burgdorferi antibodies can persist for months to years after the initial infection [
35]. Despite the higher sensitivity than STTT, MTTT sensitivity is still <90%. Thus, patients with early localized LD should be treated based on their clinical presentation rather than serologic data [
33].
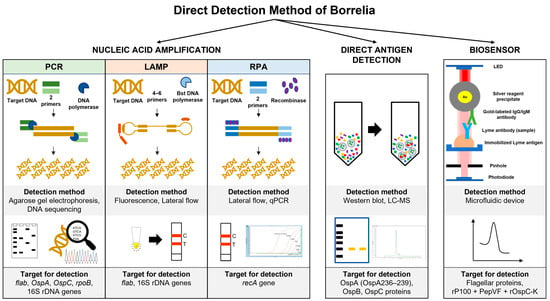
3. Direct Detection Method of Borrelia
3.1. Nucleic Acid Amplification
Most commercial kits are developed to target and conserve the genomic sequences of Borrelia species using two-step PCR (nested PCR). Borrelia species can be directly detected in patients’ samples, such as synovial fluids, cerebrospinal fluid (CSF), and blood, using polymerase chain reaction (PCR). The PCR assay targets several genes located on the genome sequence or linear plasmid of Borrelia species, such as flagellin B (
flab), outer surface protein A (
OspA),
OspC rpoB, and 16S rDNA [
38,
39,
40]. These target genes are also useful for phylogenetic analysis of Borrelia from ticks. Nevertheless, this method demonstrates various sensitivity ranges (4–100%) with 93–100% specificity [
41]. Furthermore, the sensitivity ranges between 5 and 50% for EM skin biopsies compared to the CSF samples [
42,
43]. The low DNA recovery in patients’ samples, particularly for younger patients with limited samples, reflects the unsatisfactory sensitivity of the assay.
Several PCR protocols have been established to enhance the sensitivity of the detection method in combination with the enrichment step. For instance, the loop-mediated isothermal amplification (LAMP) assay targets the 16S rRNA and has higher sensitivity (0.2 to 0.02 pg of DNA) in detecting
B. burgdorferi s.l. isolated from field-collected ticks compared to conventional and nested PCR [
44].
monitoring using the conventional photometer [
46].
Recombinase polymerase amplification (RPA) is another example of an isothermal amplification method that utilizes the recombinase protein to unwind the double-stranded DNA molecules and the strand-displacing activity to amplify DNA targets. This process takes 20–30 min from 37 °C to 42 °C [
47]. The detection limit of the RPA assay targeting the
recA gene is five copies, while the sensitivity is 50 femtograms of
B. burgdorferi genomic DNA [
48].
Even though the PCR sensitivity is high, this assay cannot differentiate between live and dead bacteria within the samples. The positive PCR result is unable to distinguish live bacteria in patients with persistent arthritis after antibiotic therapy [
49]. In addition, PCR sensitivity is also highly variable depending on the type of starting materials, DNA extraction methods, target gene location, and PCR amplification method [
50,
51,
52,
53,
54]. Thus, further evaluation of the PCR assay is still required to improve the assay sensitivity, and the method must be standardized to provide unambiguous diagnostic results.
3.2. Direct Antigen Detection
Borrelia antigen detection is a dependable, quick, accurate, and sensitive method for early LD diagnosis and improved patient care before acquiring disseminated LD. These assays are performed using Borrelia polyclonal antibodies, with the shed surface antigens detectable in the urine, blood, and various organs of infected hosts [
55]. Nonetheless, the assay sensitivity, specificity, and accuracy in detecting several antigenic moieties (31 kDa, 34 kDa, 39 kDa, and 93 kDa) are reportedly low in invalidated clinical samples [
56]. The assay can be enhanced by performing high-speed centrifugation to separate Borrelia membrane proteins from the rest of the serum proteins.
B. burgdorferi cells that have been broken will release membrane vesicles containing membrane proteins into the blood. Precisely, high-speed centrifugation contributes to a low protein detection limit at approximately 4.0 fmol of ospA/mg of serum protein [
57].
Hydrogel microparticles are widely used in biomedical research, such as being incorporated with chemical bait to mediate small target molecule sequestration and entrapment. This method helps concentrate the target molecules in the solution and eliminate other molecules through sieving. For instance, Douglas et al. reported that Acid Black 48 dye effectively acts as bait to concentrate the
B. burgdorferi OspA and OspB proteins at a limit of detection (LOD) of 700 pg/mL in 10 mL of urine [
58].
3.3. Biosensor
Several single multiplexed assays have been developed to replace the second tier of serology assays. For example, the mChip-Ld assay targeted three Borrelia antigens (VlsE, PepVF, and OspC) and showed a sensitivity range between 80% and 100% in sample patients with early Lyme disease and Lyme arthritis, respectively [
36]. Several biosensor applications have been developed to detect Borrelia antigen, including field-effect transistors (FETs) and microfluidics [
63,
64]. The attachment of
B. Burgdorferi flagellar antibodies (p41) to nanotubes effectively detected antigens in buffer (1 ng/mL) using atomic force microscopy [
63,
64]. The assay utilized the turnoff voltage measurement following antigen exposure, which involves shifting the threshold voltage towards the more negative region. Furthermore, the device is highly selective for the target antigen on the flagellar protein. In a different study, the PPO triplex test (rP100 + PepVF + rOspC-K)-based microfluidic diagnostic device (mChip-Ld) was developed for antibody detection during early and late LD stages. The assay recorded 84% sensitivity and 92% specificity, comparable to the lab-based C6 peptide ELISA [
64].
Figure 2 summarises the method used for direct detection of genetic material and soluble antigens of Borrelia.
Figure 2. Direct detection method of Borrelia using isolated genetic material and soluble antigen in various samples. The biosensor detection diagram was modified from [
54], which is open access under the Creative Commons Attribution 4.0 International license.
4. Aptamer for Borrelia Antigen Detection
The aptamer is a single-stranded nucleic acid (RNA or DNA) that can bind with various target molecules, including surface proteins, viruses, bacteria, nanoparticles, and small analytes. The aptamer can bind to target molecules with low nanomolar and picomolar affinity and distinguish the target molecule from other similar molecular structures or functional groups [
65]. Furthermore, the aptamer can form a compatible tertiary structure that fits into the binding pocket of the target molecules through hydrogen bonds and hydrophobic interaction.
The use of aptamers as diagnostic tools has been widely explored in managing infectious diseases. Xenobiotic nucleic acid (XNA) is a new aptamer variety that has been extensively studied due to its intrinsic resistance to cellular nucleases [
66]. The direct evolution of specialized XNA polymerase has promoted the enzymatic production and enrichment of XNA libraries to synthesize XNA sequences from DNA templates before being transcribed into the DNA [
67,
68,
69]. Aptamer detection has been applied to various targets of infectious diseases, such as SARS-CoV, SARS-CoV-2,
Mycobacterium tuberculosis (
M. tb), and melioidosis [
70,
71]. Several aptamers targeting tick-borne diseases have been developed, such as surface protein E of the tick-borne encephalitis virus (TBEV) and the
B. burgdorferi outer surface protein (ospA, ospC, and BmpA) associated with LD [
72].
There are several advantages to the application of aptamers as a diagnostic tool, such as ease of chemical synthesis and modification, low manufacturing costs, thermal stability, and minimum batch-to-batch variation for mass production. Despite the susceptibility to nuclease degradation, the sugar ring, nucleotide bases, and phosphodiester bond modification can improve aptamer structural stability in the nuclease environment and enhance the binding affinity to the target molecules [
73]. The aptamer can be modified at the 3′ or 5′ end with functional groups (thiol, amine, carboxyl) or biomolecules (biotin, fluorophore) for capturing and detection purposes [
74,
75,
76].
Regarding the detection of Borrelia antigen, the aptamer can be used to detect the presence of soluble proteins released by the bacteria or whole bacteria in the collected samples. Until now, various samples have been tested to detect the presence of Borrelia directly or indirectly from blood serum, cerebrospinal fluid (CSF), urine, skin biopsy, and synovial fluid [
77,
78,
79]. This bacteria’s antigen is often shed into the body fluids, which can later be detected using the aptamer. Interestingly, aptamers can function as reporters and capture agents for direct detection. Several surface proteins of Borrelia have potentially been used, such as OspA, OspC, flagellin, BBK32, PepVF, VlsE, BmpA, DbpA, and DbpB [
64,
80,
81].
This entry is adapted from the peer-reviewed paper 10.3390/biomedicines11102818