Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Surgery
Inflatable video-assisted mediastinoscopic transhiatal esophagectomy (IVMTE) has emerged as a promising treatment option for esophageal cancer because it does not require one-lung ventilation, reduces postoperative complications, and expands surgical indications. This technique also provides surgical opportunities for patients with impaired pulmonary function or thoracic lesions.
- inflatable video-assisted mediastinoscopic transhiatal esophagectomy
- esophagectomy
1. Introduction
Esophageal cancer is the seventh most common malignant tumor worldwide and the sixth leading cause of cancer-related deaths among patients with cancer [1,2]. It has a relatively high incidence in China, with nearly 90% of its pathological types being squamous cell carcinoma [3,4]. However, esophageal cancer has a relatively poor prognosis, with a 5-year survival rate of <40% [5]. Surgery is still considered the primary option for potentially curative treatment [6,7].
In recent years, with the advancement of minimally invasive techniques, laparoscopic esophagectomy has been widely used, which can shorten the postoperative rehabilitation time and reduce the probability of complications compared to traditional thoracotomy [8]. In comparison to transthoracic approaches, such as video-assisted thoracoscopic esophagectomy (VATE), which relies heavily on one-lung ventilation, the video-assisted mediastinoscopic transhiatal esophagectomy (IVMTE) procedure reaches the middle and upper esophagus via the cervical approach, eliminating the need for chest wall incisions and one-lung ventilation. This surgical method significantly reduces postoperative pain and the impact on cardiovascular function, ultimately accelerating patients’ recovery [9]. Consequently, this minimally invasive transmediastinal approach has become a viable alternative to the traditional transthoracic esophagectomy [10,11]. In 1947, Lewis et al. firstly proposed transhiatal esophagectomy [12]. In 1990, Buess first reported on esophagectomy via mediastinoscopy, which improved the safety of the surgical procedure by providing direct vision [13]. Nevertheless, achieving systematic lymph node dissection remains challenging because of limited operating space. Subsequently, mediastinoscopy has been performed for esophageal cancer resection, and carbon dioxide is used to enlarge the space by creating a pneumomediastinum [14]. Fujiwara et al. proposed IVMTE in 2015, making this surgical approach mature and progressively promoted after gradual evolution and improvement [15]. However, the tunneled surgical approach also brings difficulties to operation, and whether an anatomical structure can be clearly exposed and lymph nodes can be thoroughly dissected under mediastinoscopy has once been questioned [16,17].
2. Indications for IVMTE of Esophageal Cancer
IVMTE is less invasive than video-assisted thoracoscopic esophagectomy (VATE) because it avoids one-lung ventilation and chest trauma. This is a viable option for patients who cannot tolerate thoracotomy or thoracoscopic surgery. Indications for IVMTE include advanced age, severe pleural adhesions from a prior chest surgery, pleurisy, and past pulmonary tuberculosis. It is also recommended for patients with emphysema who have an FEV1 < 70% and vital capacity < 80% [18]. Additionally, it is suitable for patients with confirmed esophageal cancer who can be treated with R0 resection after preoperative evaluation. Some researchers suggest that IVMTE can be used for early esophageal cancer (T1–2 stage, tumor diameter < 2 cm, well-differentiated, and no lymph node metastasis), whereas others believe that it can be expanded to mid-stage esophageal cancer (no more than T3N1M0 stage) [19]. A study conducted by Daiko et al. found that surgical indications for patients with impaired lung function and a high Charlson Comorbidity Index (CCI ≥ 3) were viable as long as they could tolerate two-lung ventilation [20]. Additionally, for older patients, surgical indications for esophageal cancer should be evaluated based on the patient’s physical condition, life expectancy, tumor stage, and personal preferences [21]. When assessing the risk of postoperative complications, scoring systems, such as the estimation of physiological ability and surgical stress (E-PASS), the controlling nutritional status (CONUT), and the risk calculators provided by the Japanese National Clinical Database, should be used appropriately [22]. For patients with esophageal cancer and impaired organ function, non-thoracic esophagectomy, such as mediastinoscopy, is a better option for minimizing surgical trauma and replacing traditional transthoracic esophagectomy [23,24]. Additionally, it is crucial to preserve the bronchial artery, thoracic duct, and azygos vein arch.
3. Contraindications for IVMTE of Esophageal Cancer
Contraindications for IVMTE include (1) no definite pathological diagnosis made preoperatively; (2) severe organ dysfunction; (3) presence of distant metastasis; (4) no organ replacement in the digestive tract; and (5) when performing IVMTE, it is important to avoid factors that may hinder exposure and mobilization due to limited operating space. These factors include severe spinal deformity, stage T4 tumors, large primary tumors, significant lymphadenopathy, distant lymph node metastasis, and tissue swelling and adhesions resulting from preoperative adjuvant chemotherapy or radiotherapy. This has been mentioned in previous relevant literature [25,26]. Some investigators have suggested that IVMTE may be a viable option if CT examination determines that the tumor is resectable, regardless of whether prior treatment has been administered [27,28]. The indications and contraindications for IVMTE of esophageal cancer are summarized in Table 1.
Table 1. Indications and contraindications for IVMTE of esophageal cancer.
| IVMTE | VATE | |
|---|---|---|
| Indications | Advanced age | Any age |
| Severe pleural adhesion | Except severe pleural adhesion | |
| Emphysema with FEV1 < 70% and vital capacity < 80% | Sufficient lung function to tolerate one-lung ventilation | |
| Histopathology confirms esophageal cancer that can be treated with R0 resection | ||
| Contraindications | No definite pathological diagnosis | |
| Severe organ dysfunction | ||
| Presence of distant metastasis | ||
| Absence of replacement organs for the digestive tract | ||
| Factors that cause tight operating space: severe spinal deformity, tumor stage T4, large primary tumor, significant lymphadenopathy, distant lymph node metastasis, and tissue swelling and adhesion resulting from adjuvant chemotherapy or radiotherapy | Unresectable with invasion of adjacent tissues | |
4. Surgical Methods
During the early stages of mediastinoscopy in esophagectomy, limitations in the device and technology prevented a clear exposure of the mediastinal anatomy. Therefore, only esophageal mobilization and lymph node sampling were performed, but complete lymph node dissection was not possible [29]. If intraoperative rapid frozen-section pathological examination suggests lymph node metastasis, it may be necessary to change the body position and perform transthoracic lymph node dissection. This limits the application and promotion of the surgical approach.
4.1. Conventional IVMTE Mode
In 2015, Fujiwara et al. [15] proposed that the combination of pneumatic mediastinoscopy and laparoscopic esophagectomy represents a mature surgical approach that is increasingly being adopted by multiple medical centers. The surgical procedure involves the steps described below.
4.1.1. Cervical Procedures
The patient is positioned supine and administered general anesthesia with two-lung ventilation using a single-lumen endotracheal tube. A 4 cm incision is made on the left side of the neck, allowing access to the anterior cervical muscles. The sternocleidomastoid muscles are exposed along the medial side of the anterior cervical muscles. The cervical esophagus is mobilized, and the lymph nodes near the left recurrent laryngeal nerve (RLN) are dissected. A lap protector with an access port is inserted to seal the gap in the neck wound. This procedure results in the formation of a pneumomediastinum through inflation with carbon dioxide (8 mmHg, 1 mmHg = 0.133 kPa).
4.1.2. Transcervical Mediastinal Procedures
These procedures are performed using a LigaSure Maryland jaw sealer, and a special retractor is used to retract the arteries and esophagus. The azygos vein can be preserved because it does not affect the exposure of the esophagus; however, it is often cut off using the transthoracic approach (especially the right transthoracic route). The lymph nodes are mobilized and dissected en bloc. Finally, a right neck incision is made to dissect the lymph nodes adjacent to the right RLN under direct vision.
4.1.3. Abdominal Procedures
Carbon dioxide inflation (10 mmHg) is used for both transabdominal and transdiaphragmatic hiatus procedures. During abdominal surgery, the surgeon uses their left hand to assist the laparoscope and controls the stomach through a midline incision. In transesophageal hiatal surgery, the surgeon controls the esophagus and liver for hiatal dilation. The esophageal hiatus is opened by cutting the gastrosplenic ligament to allow entry into the mediastinum through the left diaphragmatic crus.
4.1.4. Transabdominal Mediastinal Procedures
The esophagus is mobilized axially, and the subcarinal and bilateral main parabronchial lymph nodes are dissected en bloc. The stomach is completely dissociated, the left gastric blood vessels are severed, and the abdominal lymph nodes are dissected. Finally, the esophagus is transected through a left cervical incision. A tubular stomach is created and lifted to the neck for the esophageal anastomosis.
4.2. Modified IVMTE Mode
In contrast to Fujiwara et al. [15], who ultimately performed a right cervical incision, which was only used for right recurrent laryngeal paraneurysm lymph node dissection under direct vision, Daiko et al. [14,20] proposed bilateral mediastinoscopy-assisted transdiaphragmatic hiatal laparoscopic esophagectomy (BTCMATLE) by adding a right cervical incision. The procedure is described below.
4.2.1. Cervical Procedures
A 4–5 cm incision is made 1 cm lateral to the bilateral sternocleidomastoid muscles to access the tissue space and dissect the cervical paraesophagus (No. 101 group) and most upper mediastinal lymph nodes, including the bilateral RLN lymph nodes (No. 106recR group and No. 106recL group). A lap protector is inserted into the cervical wound on both sides, the gap is closed with ports, two introducer sheaths are placed separately, a 5 mm flexible mediastinoscope lens and grasping forceps are placed on the left side, and a LigaSure Maryland jaw sealer and a retractor are placed on the right side.
4.2.2. Mediastinal Procedures
The esophagus is first freed from the anterior portion and then advanced from right to left and downwards. Typically, it can be sufficiently mobilized to expose the left atrium, after which the posterior esophagus is mobilized along the descending aorta. Finally, the left side of the esophagus is mobilized to meet the abdominal approach at the level of the left atrium. Upper (No. 105 group), middle (No. 108 group), and anterior (No. 112aoa group) thoracic paraesophageal lymph node dissections are performed. For patients with mediastinal stenosis, the BTCMATLE had good operability and a stable surgical field of view.
4.3. West China Hospital IVMTE Model
Researchers' center has also modified the surgical approach, with the left neck incision as the main operation path and the right minor incision as the auxiliary path. The surgical procedure is as follows: The patient is placed in a supine position (Figure 1a), and a 6–7 cm incision is made along the anterior border of the left sternocleidomastoid muscle (Figure 1b). The skin and subcutaneous tissues are carefully incised layer by layer. Muscle groups are gently separated. This allows visualization of the lower poles of the thyroid gland, trachea, and bilateral RLNs (Figure 1c). Additionally, bilateral cervical lymph nodes are dissected during the procedure. A small incision is made at the midpoint of the left lateral incision located at the anterior border of the right sternocleidomastoid muscle. A 5 mm trocar is then inserted, and a lap protector is placed in the left incision to establish a closed cavity. Finally, the mediastinum is inflated (pressure of 8 mmHg and flow of 10 L/min). An aspirator, mediastinoscope lens, and a LigaSure Maryland jaw sealer are placed on the left side, and a retractor is placed on the right side (Figure 1d). The esophageal wall is dissected in accordance with the sequence of “left—anterior—right—posterior” (Figure 2a). This is performed up to the carina level and is sometimes extended down to the inferior pulmonary vein level. During this process, various lymph nodes are also dissected, including the bilateral RLN, paraesophageal, tracheobronchial (No. 106tbL group), and subcarinal lymph nodes (Figure 2b). The authors concluded that dissecting the bilateral lymph nodes adjacent to the RLN is technically feasible through a left cervical incision under direct vision. By utilizing a suction apparatus and retractor, adequate exposure can be achieved while minimizing smoke interference, thereby decreasing surgical difficulty (Figure 2c,d). Morbidities associated with the IVMTE learning curve were analyzed.

Figure 1. (a) Position of the patient, (b) cervical incision, (c) left cervical mobilization, and (d) dispensation of the cervical device.
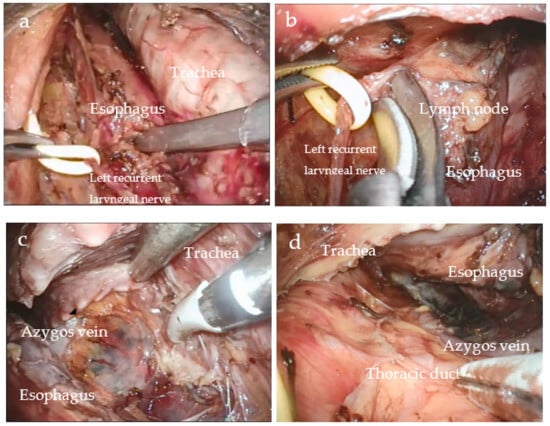
Figure 2. Transcervical view during esophageal mobilization. (a) Upper esophageal mobilization, (b) dissection of the lymph nodes around left RLN, (c) anterior mobilization of esophagus, and (d) posterior mobilization of esophagus.
This entry is adapted from the peer-reviewed paper 10.3390/biomedicines11102750
This entry is offline, you can click here to edit this entry!