Patients suffering from chronic gastritis and developing gastric mucosa atrophy are at increased risk of the development of gastric cancer. The diagnosis of chronic atrophic gastritis (CAG) is a complex procedure involving a detailed history taking, a thorough physical examination and the use of laboratory and instrumental diagnostic methods among which the endoscopy of the upper digestive tract is the cornerstone because it allows the assessment of the topography of gastritis and identification of erosions and areas of intestinal metaplasia with the use of NBI endoscopy. However, the diagnosis of CAG requires morphological examination of the gastric mucosa.
1. Introduction
Chronic atrophic gastritis (CAG) is the final stage of the inflammatory process, the key characteristic of which is the decrease of gastric glands substitute with fibrous tissue or metaplastic epithelium. The histopathological cascade of gastric carcinogenesis, also called as Correa’s cascade, after the pathologist who first described it in 1975, is a step-by-step process with unchanged gastric mucosa in the beginning followed by chronic superficial gastritis, chronic atrophic gastritis, intestinal metaplasia and dysplasia stages, and cancer in the end [
1]. These characteristics describe structural changes in the gastric mucosa at all stages of gastric carcinogenesis and highlight the importance of CAG identification for cancer prevention.
There are two main methodological approaches for the diagnosis of CAG. The first one suggests serological testing using markers of gastric function (pepsinogen I, pepsinogen I/pepsinogen II ratio, additional stimulated and basal gastrin-17), non-invasive testing for Helicobacter pylori (H. pylori) infection and, if required, endoscopic examination of gastrobiopsy specimens for histopathological verification of atrophy in case of identified atrophy stigmas in the patient. The second approach involves the invasive biopsy procedure from the start for histological analysis of biopsy specimens collected during esophagogastroduodenoscopy.
2. The Etiological Factor of Gastritis and the Atrophy Risk
The two most significant etiological factors of CAG are
H. pylori infection and autoimmune inflammation, with the dominant infectious factor [
17,
18].
H. pylori is a gram-negative, curved or S-shaped microaerophilic bacterium with high motility due to a unipolar bundle of coated flagella [
19].
H. pylori is thought to have been acquired by modern humans in Africa at least ~100,000 years ago, possibly being transmissed from an unknown animal [
20]. The most ancient phylogeographic population of
H. pylori is hpAfrica2, mainly found in South Africa. Other important, widespread, and recent populations include hpAfrica1, hpNEAfrica, hpEurope, hpEastAsia, hpAsia2, and hpSahul [
21,
22]. An important step in the evolution of
H. pylori from the ancestral population of hpAfrica2 to populations that spread around the world was the acquisition of the cag pathogenicity island (cagPAI), which encodes the components of the Cag T4SS protein complex [
23,
24], surrounding the bacterial cell membrane and facilitating the delivery of various effector molecules into host cells after attachment.
H. pylori is well adapted to colonize a unique ecological niche in the deep near-wall mucus layer of the antral mucosa. Several mechanisms, including motility, urease production, adhesion, and others, are important for
H. pylori colonization [
25,
26,
27].
H. pylori colonization of the gastric mucosa induces a proinflammatory response involving various immune cells in the mucosal layer resulting in chronic active gastritis [
28]. The severity of inflammation varies greatly in individuals depending on bacterial, host and environmental factors [
29,
30]. The most important determinant of the pro-inflammatory activity of the
H. pylori strain is its functional cagPAI [
31,
32]. Expression of additional host interaction factors, such as a set of adhesins that promotes strong binding to epithelial cells depends on the variable composition of host receptors [
33].
In addition to association with
H. pylori, CAG may also be primarily of autoimmune nature due to the production of autoantibodies to gastric parietal cells and/or intrinsic Castle factor. The prevalence of autoimmune gastritis (AIG) in the population ranges from 1 to 8% [
54]. The risk group of patients with autoimmune inflammation of the gastric mucosa includes women suffering from autoimmune diseases (e.g., type 1 diabetes mellitus, autoimmune thyroiditis), as well as celiac disease [
55]. It is noteworthy that the experts of the Maastricht Consensus addressed the problem of the diagnosis of autoimmune gastritis [
42]. For example, one of the provisions (WG 2 Diagnostics Statement 6) states that gastric functional serology (pepsinogens I-II and gastrin levels), anti-
H. pylori antibodies, anti-intrinsic factor and anti-parietal cell auto-antibodies may provide clinically valuable information on the likelihood of gastric mucosal atrophy, including its aetiology (agreement: 98%, grade 1 A).
It should be noted that with primary AIG, the risk of neuroendocrine tumors increases compared with other etiological factors of gastritis, but the risk of gastric adenocarcinoma is lower than with multifocal atrophy of the gastric mucosa due to
H. pylori infection (involving the mucous membrane of the antrum and body). Epidemiological studies estimate the incidence of gastric adenocarcinoma among patients with autoimmune gastritis as 14.2 cases per 1000 person-years [
56]. A study carried out in Sweden reported that the risk of developing gastric cancer in patients with autoimmune gastritis was 7.4 versus 1.4 cases per 1000 patient-years in the general population [
57], and a study performed in Finland reported a similar value risk with a standardized incidence rate of 5.0 [
58].
3. Possibilities of Endoscopic Examination and Sampling of Biopsy Specimens for the Diagnosis of Gastric Mucosa Atrophy
Endoscopic examination plays a key role in the diagnosis of CAG, since the competency of the endoscopist and the adequacy of gastrobiopsy sampling determine the subsequent morphological assessment of the lesion of the gastric mucosa and verification of the diagnosis [59]. The key data for the diagnosis of chronic atrophic gastritis, which can be obtained from the results of endoscopic examination, are the topography of gastritis and the actual identification of atrophy and metaplasia zones [60]. The inflammation of the gastric mucosa is usually considered from the standpoint of a predominant lesion of an organ part: body gastritis, antrum gastritis, pangastritis [61,62]. Clinical interpretation of the topography of inflammation can be as follows. The body gastric mucosa predominantly involved in the inflammatory process may indicate the presence of AIG [63]. In adults, and in cases of introduction of H. pylori infection during adolescence, inflammation begins in the antrum, in the so-called “ecological niche” of the H. pylori bacterium [20]. Further spread of the H. pylori infection in the proximal direction results in the additional involvement of the body of the stomach in the inflammatory process. Pangastritis is formed in this way. Regardless of the etiology, the dominance of gastric lesions is an unfavorable sign in terms of the risk of developing gastric cancer [44].
According to the data published in the literature, the sensitivity and specificity of conventional white light endoscopy for diagnosing gastric mucosal atrophy are 53–59%, and those of high-definition white light endoscopy with magnification are 70–74% [
64]. The study by Zhang Q. et al. presents findings of a meta-analysis of the data collected from 1724 patients which indicate that the combined sensitivity and specificity of white light endoscopy for diagnosing early gastric cancer were 48% and 67%, respectively [
65]. Moreover, a meta-analysis of 22 studies showed that almost 10% of gastric cancers could potentially be missed during white light endoscopy, mainly it relates to adenocarcinoma of the body of the stomach [
66].
To overcome the diagnostic limitations of standard white light endoscopy in detecting premalignant changes in the gastric mucosa, various imaging enhanced endoscopy (IEE) techniques have been developed, including dye chromoscopy, high-resolution imaging, virtual chromoscopy, and artificial intelligence [
65,
67,
68].
Chromoendoscopy (CE) is an IEE technique that sprays dyes onto the surface of the gastric mucosa to improve visualization of the lesions under study. The use of CE in the screening of malignancies and premalignant changes in the gastric mucosa can increase the detection rate and provide more accurate visualization of the boundaries of the lesion, which helps to differentiate benign or inflammatory changes from suspected precancerous or malignant ones and determine the zones for biopsy [
60,
69].
Virtual or electronic chromoendoscopy are imaging methods allowing a detailed examination of the gastric mucosa. Their use increases the efficiency of diagnosing precancerous changes and makes it easier for the endoscopist to select areas “suspicious” for intestinal metaplasia or dysplasia for taking gastrobiopsy specimens without any dye techniques. The methods are easy to use and less time-consuming than when using dyes [
60,
71,
72].
One of the virtual chromoendoscopy methods is narrow band imaging (NBI) developed by Olympus (Olympus Medical Systems Co., Ltd., Tokyo, Japan). The principle of NBI endoscopy is based on an optical phenomenon in which the depth of penetration of light into tissues depends on the wavelength. NBI uses narrow spectra of blue light (415 nm) and green light (540 nm) due to light filters installed in the illuminator, which allows you to get a clearer, more detailed image of the gastric mucosa [
60]. The sensitivity and specificity of NBI endoscopy for the diagnosis of the gastric mucosa atrophy reach 95 and 98.5%, and for the diagnosis of early gastric cancer, they are 83% and 96%, respectively [
64].
The standard for the study of biopsy specimens is the OLGA-system protocol which involves taking two fragments from the body of the stomach, two fragments from the antrum and one fragment from the incisura angularis of the stomach, and allows assessing the stage of the process and the risk of developing gastric cancer [
75]. In a detailed presentation, modern recommendations are indicated as follows: two biopsies from the antrum of the stomach at a distance of 2 cm from the pylorus along the lesser and greater curvatures, one biopsy from the incisura angularis and two biopsies from the body of the stomach at a distance of 8 cm from the rosette of the cardia along the lesser and greater curvatures [
76].
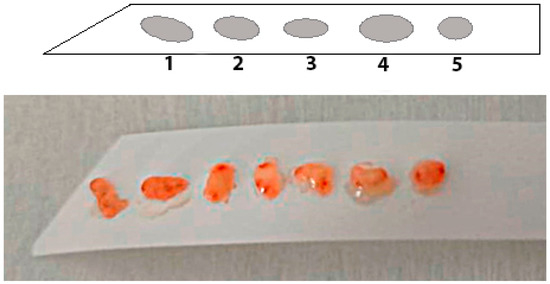
The use of special adhesive strips can be one of the effective approaches to solve the problem of orientation and fragmentation of biopsies. Orientation using specialized adhesive strips made of cellulose acetate can be carried out by fixing tissue fragments to the strip using manual pressing for 5 s. In this case, the first biopsy specimen is placed at the pointed end of the strip, which provides intuitive recognition of the serial number of the biopsy tissue sample (Figure 1).
Figure 1. Adhesive orientation strip for biopsy material with tissue fragments located on it. The sequential order of the tissue fragments in the direction from the pointed end allows the marking of the fragments. The photo presents a sequence of 7 oriented tissue fragments.
4. Histological Examination—“Pitfalls” of a Standard Study
In the OLGA (Operative Link for Gastritis Assessment) predictive system, the severity of mucosal atrophy is commonly referred to as the stage of gastritis [
62]. There are five stages: stage 0—there is no atrophy, minimal risk of gastric cancer; stages I and II—there is a moderate risk; stages III–IV—there is a high risk (5–6 times higher than in the population). The grade of gastritis is understood as the intensity of infiltration of the gastric mucosa by inflammatory cells: mononuclear and segmented leukocytes together, and not separately, as in the Modified Sydney system [
81,
82].
The stage of gastritis is a predictive indicator that is used and clinically interpreted much more often than the degree [
83]. The degree is usually treated in the same way as the indicator “inflammation” in the Modified Sydney system. The higher grade, the more pronounced the inflammatory cell infiltration, the more cytokines are formed in the gastric lamina propria, the more intense the transformation of specialized cells of the gastric glands into epithelium of intestinal phenotype—intestinal metaplasia—metaplastic atrophy. Therefore, the grade of gastritis is an indirect indicator of the intensity of the patient’s inflammatory response and, therefore, a high degree reflects the acceleration of the development of the carcinogenesis cascade (Correa’s cascade) from chronic inflammation to gastric cancer [
84,
85].
The assessment of a gastritis stage (severity of atrophy of the glands) is quite subjective. Atrophy is a concept that is not quite accurately identified for a practicing pathologist, which causes insufficient reproducibility of conclusions by different specialists [
86]. An additional difficulty for the identification of atrophy is the inflammatory infiltrate, which persists even under the conditions of
H. pylori eradication and spreading glands. The term “indefinite atrophy” is used to designate such a condition [
87,
88].
Another thing is intestinal metaplasia, a morphologically striking phenomenon, reproduced by pathologists with a high degree of agreement. The OLGIM (Operative Link on Intestinal Metaplasia Assessment) system has been developed for a predictive assessment of the risk of developing gastric cancer based on the identification of intestinal metaplasia in the biopsy specimen. If inflammation and indefinite atrophy can regress with timely and rational therapy, then intestinal metaplasia has no tendency to reverse development [
89].
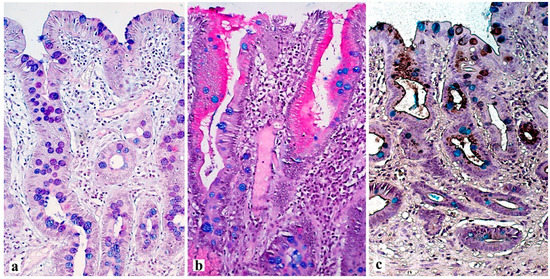
Intestinal metaplasia is a stigma of atrophy and is defined as the transformation of gastric glandular epithelium into intestinal epithelium. By prevalence, intestinal metaplasia is categorized as limited if the pathological process is located in one anatomical region of the stomach, or as extensive if two regions of the stomach are involved. According to the type of mucins in the lining epithelium, intestinal metaplasia is divided into complete and incomplete. Complete (type I) intestinal metaplasia is similar to the epithelium of the small intestine, and incomplete (type ΙΙ and type ΙΙΙ) intestinal metaplasia is similar to the epithelium of the large intestine (Figure 2).
Figure 2. Various types of intestinal metaplasia of the gastric mucosa. (a) complete intestinal metaplasia (type I) with a well-defined magenta stained brush border between the goblet cells stained with purple or blue. (b) incomplete intestinal metaplasia (type II) with the presence of mucus-producing epithelium between goblet cells, with the production of magenta stained neutral (in this case) or blue stained sialomucins. (c) incomplete intestinal metaplasia (type III) with production of sulfomucins by cylindrical cells brownish black stained with HID (high iron diamine) stain. (a,b)—PAS stain with alcian blue (pH = 2.5), (c)—high iron diamine with alcian blue (pH = 2.5). ×200.
Relatively recently, the corpus-predominant gastritis index has been included in the diagnostic practice. It is calculated from the totality of microscopic signs of gastritis in the Modified Sydney system. If these signs have higher gradations in the body of the stomach in comparison with the antrum, then the patient has a high risk of developing gastric cancer. The scholars believe that this indicator is more accurate than the staging of atrophy/metaplasia according to the OLGA and OLGIM systems of grading [
90].
Immunohistochemical examination in the diagnosis of atrophy has a supporting role. As a rule, the phenomenon of gland decrease is well visualized during routine histopathological examination. Gastrointestinal mucins can be used to better identify the glandular structures, especially in the case of a pronounced inflammatory infiltrate, to assess the level of functional maturity of cells. Of particular importance is the identification of the transformed cell phenotype, the so-called metaplastic atrophy [
18,
91,
92].
Distinguishing its two main types—intestinal and pseudopyloric (pyloric) metaplasia according to modern diagnostic approaches, the emphasis is shifting towards the diagnosis of SPEM (spasmolytic polypeptide-expressing metaplasia) as a special cell line associated with the risk of developing gastric adenocarcinoma rather than the ordinary intestinal metaplasia [
76].
5. Conclusions
The active introduction of OLGA/OLGIM system into the clinical practice allows the assessment of an individual’s risk of developing gastric cancer in a patient with chronic gastritis. The significant problem is the decrease in the informativeness of the histopathological assessment of chronic gastritis due to fragmentation and orientation of the biopsy material, which requires the use of special approaches. An additional opportunity in the study of biopsy specimens of the gastric mucosa is the identification of signs of gastritis specific for autoimmune inflammation and H. pylori infection. Modern approaches with the use of immunohistochemical markers in the examination of biopsies of the gastric mucosa play an auxiliary role in the identification of atrophy and intestinal metaplasia, and they may be important in determining the cell phenotype in ambiguous diagnostic cases.
This entry is adapted from the peer-reviewed paper 10.3390/diagnostics13152478