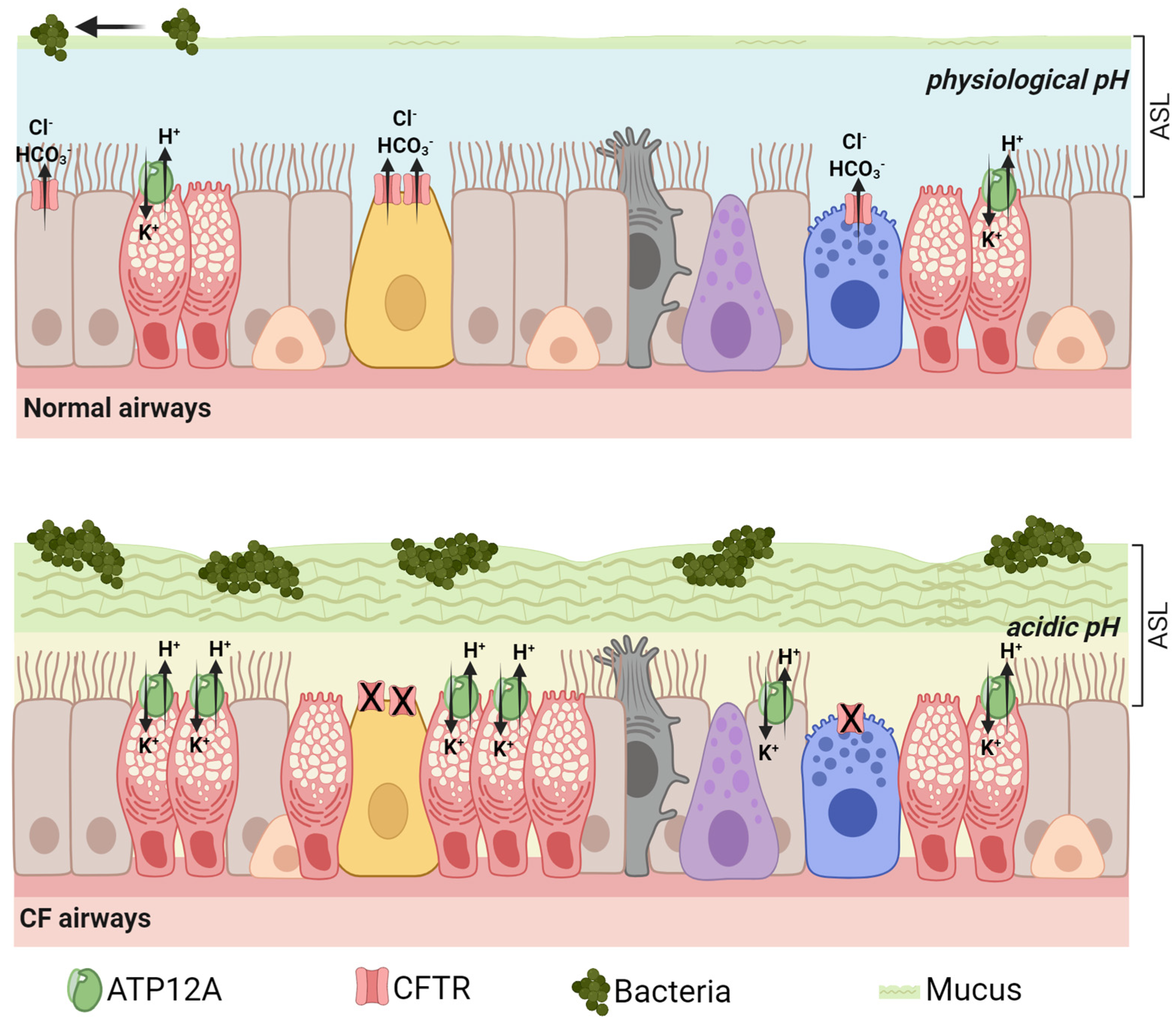
ATP12A encodes the catalytic subunit of the non-gastric proton pump, which is expressed in many epithelial tissues and mediates the secretion of protons in exchange for potassium ions. In the airways, ATP12A-dependent proton secretion contributes to complex mechanisms regulating the composition and properties of the fluid and mucus lining the respiratory epithelia, which are essential to maintain the airway host defense and the respiratory health. Increased expression and activity of ATP12A in combination with the loss of other balancing activities, such as the bicarbonate secretion mediated by CFTR, leads to excessive acidification of the airway surface liquid and mucus dysfunction, processes that play relevant roles in the pathogenesis of cystic fibrosis and other chronic inflammatory respiratory disorders. Here, the researchers summarize the findings dealing with ATP12A expression, function, and modulation in the airways, which led to the consideration of ATP12A as a potential therapeutic target for the treatment of cystic fibrosis and other airway diseases; the researchers also highlight the current advances and gaps regarding the development of therapeutic strategies aimed at ATP12A inhibition.
- ATP12A
- modifier genes
- airway acidification
- cystic fibrosis
- ASL
- proton transport
- respiratory diseases
1. Introduction
2. ATP12A Proton Pump Structure and Assembly
3. ATP12A Drives Airway Acidification in CF: Lessons from Animal Models
4. ATP12A Expression, Function, and Modulation in CF and Other Respiratory Diseases
5. ATP12A as a Modifier of Meconium Ileus in CF
6. Potential Strategies for ATP12A Targeting
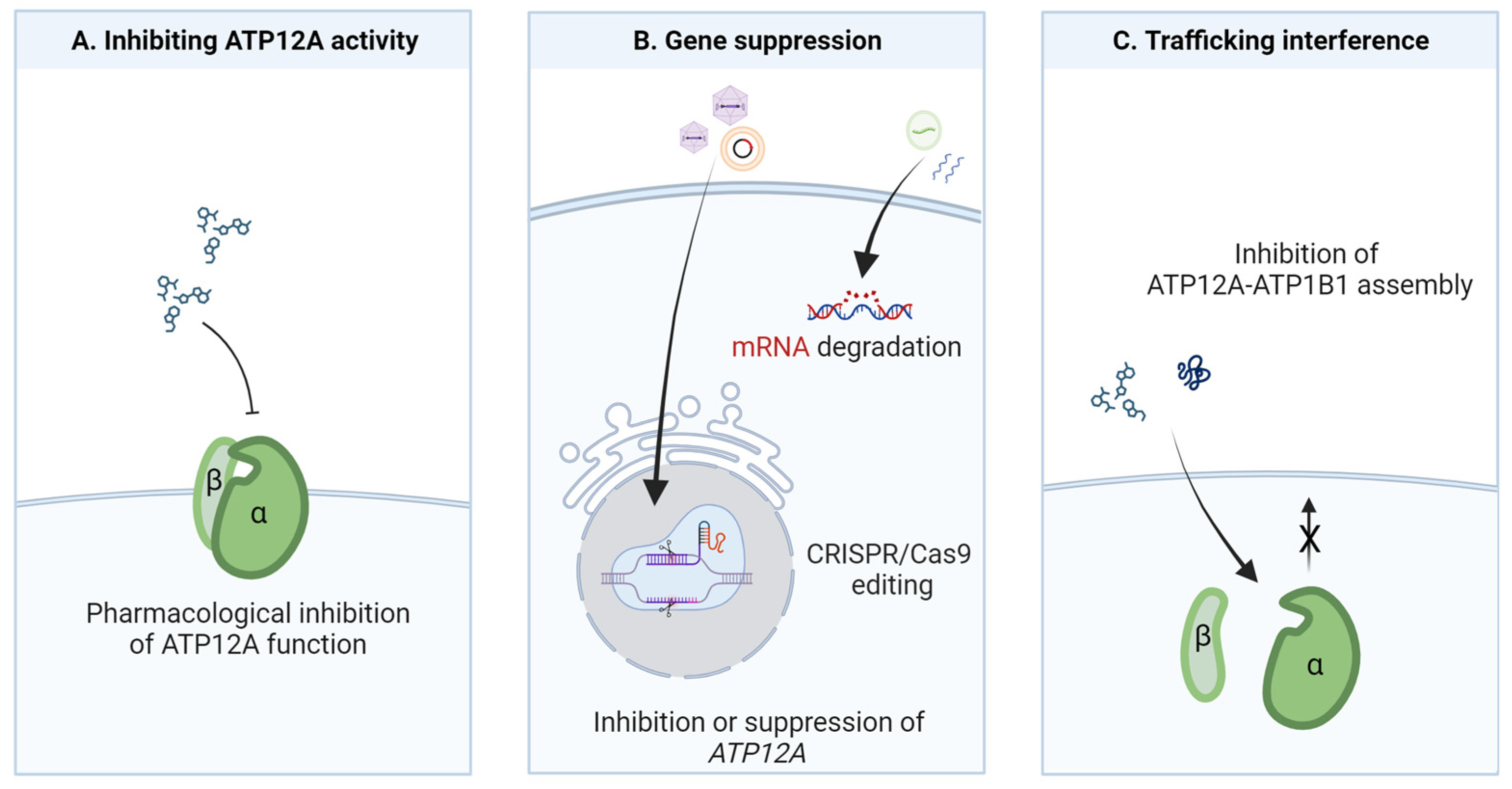
Figure 2. Potential strategies for ATP12A targeting in airway diseases. (A) Inhibition of ATP12A proton pump function can be achieved by screening libraries of small molecules with appropriate functional assays. (B) ATP12A gene suppression or downregulation can be achieved by targeting genomic DNA (genome editing) or mRNA (antisense strategy) through different delivery agents. (C) Trafficking interference could be achieved by in silico screening of chemical libraries to find molecules hindering α/β subunit assembly and therefore the trafficking of the proton pump to the plasma membrane.
This entry is adapted from the peer-reviewed paper 10.3390/biom13101455
References
- Sverdlov, V.E.; Kostina, M.B.; Modyanov, N.N. Genomic Organization of the Human ATP1AL1 Gene Encoding a Ouabain-Sensitive H,K-ATPase. Genomics 1996, 32, 317–327.
- Zajac, M.; Dreano, E.; Edwards, A.; Planelles, G.; Sermet-Gaudelus, I. Airway Surface Liquid PH Regulation in Airway Epithelium Current Understandings and Gaps in Knowledge. Int. J. Mol. Sci. 2021, 22, 3384.
- Jaisser, F.; Beggah, A.T. The Nongastric H+-K+-ATPases: Molecular and Functional Properties. Am. J. Physiol. 1999, 276, F812–F824.
- Gumz, M.L.; Lynch, I.J.; Greenlee, M.M.; Cain, B.D.; Wingo, C.S. The Renal H+-K+-ATPases: Physiology, Regulation, and Structure. Am. J. Physiol. Ren. Physiol. 2010, 298, F12–F21.
- Pestov, N.B.; Korneenko, T.V.; Adams, G.; Tillekeratne, M.; Shakhparonov, M.I.; Modyanov, N.N. Nongastric H-K-ATPase in Rodent Prostate: Lobe-Specific Expression and Apical Localization. Am. J. Physiol. Cell Physiol. 2002, 282, C907–C916.
- Pestov, N.B.; Korneenko, T.V.; Shakhparonov, M.I.; Shull, G.E.; Modyanov, N.N. Loss of Acidification of Anterior Prostate Fluids in ATP12A-Null Mutant Mice Indicates That Nongastric H-K-ATPase Functions as Proton Pump in Vivo. Am. J. Physiol. Cell Physiol. 2006, 291, C366–C374.
- Favia, M.; Gerbino, A.; Notario, E.; Tragni, V.; Sgobba, M.N.; Dell’Aquila, M.E.; Pierri, C.L.; Guerra, L.; Ciani, E. The Non-Gastric H+/K+ ATPase (ATP12A) Is Expressed in Mammalian Spermatozoa. Int. J. Mol. Sci. 2022, 23, 1048.
- Gorrieri, G.; Scudieri, P.; Caci, E.; Schiavon, M.; Tomati, V.; Sirci, F.; Napolitano, F.; Carrella, D.; Gianotti, A.; Musante, I.; et al. Goblet Cell Hyperplasia Requires High Bicarbonate Transport to Support Mucin Release. Sci. Rep. 2016, 6, 36016.
- Scudieri, P.; Musante, I.; Caci, E.; Venturini, A.; Morelli, P.; Walter, C.; Tosi, D.; Palleschi, A.; Martin-Vasallo, P.; Sermet-Gaudelus, I.; et al. Increased Expression of ATP12A Proton Pump in Cystic Fibrosis Airways. JCI Insight 2018, 3, e123616.
- Coakley, R.D.; Grubb, B.R.; Paradiso, A.M.; Gatzy, J.T.; Johnson, L.G.; Kreda, S.M.; O’Neal, W.K.; Boucher, R.C. Abnormal Surface Liquid pH Regulation by Cultured Cystic Fibrosis Bronchial Epithelium. Proc. Natl. Acad. Sci. USA 2003, 100, 16083–16088.
- Abou Alaiwa, M.H.; Reznikov, L.R.; Gansemer, N.D.; Sheets, K.A.; Horswill, A.R.; Stoltz, D.A.; Zabner, J.; Welsh, M.J. PH Modulates the Activity and Synergism of the Airway Surface Liquid Antimicrobials β-Defensin-3 and LL-37. Proc. Natl. Acad. Sci. USA 2014, 111, 18703–18708.
- Li, X.; Villacreses, R.; Thornell, I.M.; Noriega, J.; Mather, S.; Brommel, C.M.; Lu, L.; Zabner, A.; Ehler, A.; Meyerholz, D.K.; et al. V-Type ATPase Mediates Airway Surface Liquid Acidification in Pig Small Airway Epithelial Cells. Am. J. Respir. Cell Mol. Biol. 2021, 65, 146–156.
- Young, V.C.; Nakanishi, H.; Meyer, D.J.; Nishizawa, T.; Oshima, A.; Artigas, P.; Abe, K. Structure and Function of H+/K+ Pump Mutants Reveal Na+/K+ Pump Mechanisms. Nat. Commun. 2022, 13, 5270.
- Grishin, A.V.; Caplan, M.J. ATP1AL1, a Member of the Non-Gastric H,K-ATPase Family, Functions as a Sodium Pump. J. Biol. Chem. 1998, 273, 27772–27778.
- Shah, V.S.; Meyerholz, D.K.; Tang, X.X.; Reznikov, L.; Abou Alaiwa, M.; Ernst, S.E.; Karp, P.H.; Wohlford-Lenane, C.L.; Heilmann, K.P.; Leidinger, M.R.; et al. Airway Acidification Initiates Host Defense Abnormalities in Cystic Fibrosis Mice. Science 2016, 351, 503–507.
- Shteinberg, M.; Haq, I.J.; Polineni, D.; Davies, J.C. Cystic Fibrosis. Lancet 2021, 397, 2195–2211.
- Grubb, B.R.; Boucher, R.C. Pathophysiology of Gene-Targeted Mouse Models for Cystic Fibrosis. Physiol. Rev. 1999, 79, S193–S214.
- Guilbault, C.; Saeed, Z.; Downey, G.P.; Radzioch, D. Cystic Fibrosis Mouse Models. Am. J. Respir. Cell Mol. Biol. 2007, 36, 1–7.
- Pezzulo, A.A.; Tang, X.X.; Hoegger, M.J.; Abou Alaiwa, M.H.; Ramachandran, S.; Moninger, T.O.; Karp, P.H.; Wohlford-Lenane, C.L.; Haagsman, H.P.; van Eijk, M.; et al. Reduced Airway Surface pH Impairs Bacterial Killing in the Porcine Cystic Fibrosis Lung. Nature 2012, 487, 109–113.
- Hoegger, M.J.; Fischer, A.J.; McMenimen, J.D.; Ostedgaard, L.S.; Tucker, A.J.; Awadalla, M.A.; Moninger, T.O.; Michalski, A.S.; Hoffman, E.A.; Zabner, J.; et al. Impaired Mucus Detachment Disrupts Mucociliary Transport in a Piglet Model of Cystic Fibrosis. Science 2014, 345, 818–822.
- Birket, S.E.; Chu, K.K.; Liu, L.; Houser, G.H.; Diephuis, B.J.; Wilsterman, E.J.; Dierksen, G.; Mazur, M.; Shastry, S.; Li, Y.; et al. A Functional Anatomic Defect of the Cystic Fibrosis Airway. Am. J. Respir. Crit. Care Med. 2014, 190, 421–432.
- Randell, S.H.; Boucher, R.C. Effective Mucus Clearance Is Essential for Respiratory Health. Am. J. Respir. Cell Mol. Biol. 2006, 35, 20–28.
- Lennox, A.T.; Coburn, S.L.; Leech, J.A.; Heidrich, E.M.; Kleyman, T.R.; Wenzel, S.E.; Pilewski, J.M.; Corcoran, T.E.; Myerburg, M.M. ATP12A Promotes Mucus Dysfunction during Type 2 Airway Inflammation. Sci. Rep. 2018, 8, 2109.
- Min, J.-Y.; Ocampo, C.J.; Stevens, W.W.; Price, C.P.E.; Thompson, C.F.; Homma, T.; Huang, J.H.; Norton, J.E.; Suh, L.A.; Pothoven, K.L.; et al. Proton Pump Inhibitors Decrease Eotaxin-3/CCL26 Expression in Patients with Chronic Rhinosinusitis with Nasal Polyps: Possible Role of the Nongastric H,K-ATPase. J. Allergy Clin. Immunol. 2017, 139, 130–141.e11.
- Schultz, A.; Puvvadi, R.; Borisov, S.M.; Shaw, N.C.; Klimant, I.; Berry, L.J.; Montgomery, S.T.; Nguyen, T.; Kreda, S.M.; Kicic, A.; et al. Airway Surface Liquid pH Is Not Acidic in Children with Cystic Fibrosis. Nat. Commun. 2017, 8, 1409.
- Massey, M.K.; Reiterman, M.J.; Mourad, J.; Luckie, D.B. Is CFTR an Exchanger?: Regulation of HCO3− Transport and Extracellular pH by CFTR. Biochem. Biophys. Rep. 2020, 25, 100863.
- Garland, A.L.; Walton, W.G.; Coakley, R.D.; Tan, C.D.; Gilmore, R.C.; Hobbs, C.A.; Tripathy, A.; Clunes, L.A.; Bencharit, S.; Stutts, M.J.; et al. Molecular Basis for pH-Dependent Mucosal Dehydration in Cystic Fibrosis Airways. Proc. Natl. Acad. Sci. USA 2013, 110, 15973–15978.
- Shah, V.S.; Ernst, S.; Tang, X.X.; Karp, P.H.; Parker, C.P.; Ostedgaard, L.S.; Welsh, M.J. Relationships among CFTR Expression, HCO3− Secretion, and Host Defense May Inform Gene- and Cell-Based Cystic Fibrosis Therapies. Proc. Natl. Acad. Sci. USA 2016, 113, 5382–5387.
- Guidone, D.; Buccirossi, M.; Scudieri, P.; Genovese, M.; Sarnataro, S.; De Cegli, R.; Cresta, F.; Terlizzi, V.; Planelles, G.; Crambert, G.; et al. Airway Surface Hyperviscosity and Defective Mucociliary Transport by IL-17/TNF-α Are Corrected by Beta-Adrenergic Stimulus. JCI Insight 2022, 7, e164944.
- Delpiano, L.; Thomas, J.J.; Yates, A.R.; Rice, S.J.; Gray, M.A.; Saint-Criq, V. Esomeprazole Increases Airway Surface Liquid pH in Primary Cystic Fibrosis Epithelial Cells. Front. Pharmacol. 2018, 9, 1462.
- Abdelgied, M.; Uhl, K.; Chen, O.G.; Schultz, C.; Tripp, K.; Peraino, A.M.; Paithankar, S.; Chen, B.; Kakazu, M.T.; Bahena, A.C.; et al. Targeting ATP12A, a Non-Gastric Proton Pump Alpha Subunit, for Idiopathic Pulmonary Fibrosis Treatment. Am. J. Respir. Cell Mol. Biol. 2023, 68, 638–650.
- Saint-Criq, V.; Gray, M.A. Role of CFTR in Epithelial Physiology. Cell. Mol. Life Sci. 2017, 74, 93–115.
- Weiler, C.A.; Drumm, M.L. Genetic Influences on Cystic Fibrosis Lung Disease Severity. Front. Pharmacol. 2013, 4, 40.
- Collaco, J.M.; Cutting, G.R. Update on Gene Modifiers in Cystic Fibrosis. Curr. Opin. Pulm. Med. 2008, 14, 559–566.
- Marson, F.A.L. Disease-Modifying Genetic Factors in Cystic Fibrosis. Curr. Opin. Pulm. Med. 2018, 24, 296–308.
- Gong, J.; Wang, F.; Xiao, B.; Panjwani, N.; Lin, F.; Keenan, K.; Avolio, J.; Esmaeili, M.; Zhang, L.; He, G.; et al. Genetic Association and Transcriptome Integration Identify Contributing Genes and Tissues at Cystic Fibrosis Modifier Loci. PLoS Genet. 2019, 15, e1008007.
- Sathe, M.; Houwen, R. Meconium Ileus in Cystic Fibrosis. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2017, 16, S32–S39.
- Quinton, P.M. Cystic Fibrosis: Impaired Bicarbonate Secretion and Mucoviscidosis. Lancet Lond. Engl. 2008, 372, 415–417.
- Scheele, G.A.; Fukuoka, S.I.; Kern, H.F.; Freedman, S.D. Pancreatic Dysfunction in Cystic Fibrosis Occurs as a Result of Impairments in Luminal pH, Apical Trafficking of Zymogen Granule Membranes, and Solubilization of Secretory Enzymes. Pancreas 1996, 12, 1–9.
- Singh, V.K.; Schwarzenberg, S.J. Pancreatic Insufficiency in Cystic Fibrosis. J. Cyst. Fibros. 2017, 16, S70–S78.
- Wang, J.; Barbuskaite, D.; Tozzi, M.; Giannuzzo, A.; Sørensen, C.E.; Novak, I. Proton Pump Inhibitors Inhibit Pancreatic Secretion: Role of Gastric and Non-Gastric H+/K+-ATPases. PLoS ONE 2015, 10, e0126432.
- Simonin, J.; Bille, E.; Crambert, G.; Noel, S.; Dreano, E.; Edwards, A.; Hatton, A.; Pranke, I.; Villeret, B.; Cottart, C.-H.; et al. Airway Surface Liquid Acidification Initiates Host Defense Abnormalities in Cystic Fibrosis. Sci. Rep. 2019, 9, 6516.
- Grishin, A.V.; Bevensee, M.O.; Modyanov, N.N.; Rajendran, V.; Boron, W.F.; Caplan, M.J. Functional expression of the cDNA encoded by the human ATP1AL1 gene. Am. J. Physiol. 1996, 271, F539–F551.
- Xiong, W.; Zhang, Q.; Zhao, W.; Ding, W.; Liu, J.; Zhao, Y. A 12-month Follow-up Study on the Preventive Effect of Oral Lansoprazole on Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Int. J. Exp. Pathol. 2016, 97, 107–113.
- Oshima, T.; Miwa, H. Potent Potassium-Competitive Acid Blockers: A New Era for the Treatment of Acid-Related Diseases. J. Neurogastroenterol. Motil. 2018, 24, 334–344.
- Knowles, M.R.; Robinson, J.M.; Wood, R.E.; Pue, C.A.; Mentz, W.M.; Wager, G.C.; Gatzy, J.T.; Boucher, R.C. Ion composition of airway surface liquid of patients with cystic fibrosis as compared with normal and disease-control subjects. J. Clin. Investig. 1997, 100, 2588–2595.
- Namkung, W.; Song, Y.; Mills, A.D.; Padmawar, P.; Finkbeiner, W.E.; Verkman, A.S. In situ measurement of airway surface liquid using a ratioable K+-sensitive fluorescent dye. J. Biol. Chem. 2009, 284, 15916–15926.
- Sui, H.; Xu, X.; Su, Y.; Gong, Z.; Yao, M.; Liu, X.; Zhang, T.; Jiang, Z.; Bai, T.; Wang, J.; et al. Gene Therapy for Cystic Fibrosis: Challenges and Prospects. Front. Pharmacol. 2022, 13, 1015926.
- Perricone, M.A.; Morris, J.E.; Pavelka, K.; Plog, M.S.; O’Sullivan, B.P.; Joseph, P.M.; Dorkin, H.; Lapey, A.; Balfour, R.; Meeker, D.P.; et al. Aerosol and Lobar Administration of a Recombinant Adenovirus to Individuals with Cystic Fibrosis. II. Transfection Efficiency in Airway Epithelium. Hum. Gene Ther. 2001, 12, 1383–1394.
- Joseph, P.M.; O’Sullivan, B.P.; Lapey, A.; Dorkin, H.; Oren, J.; Balfour, R.; Perricone, M.A.; Rosenberg, M.; Wadsworth, S.C.; Smith, A.E.; et al. Aerosol and Lobar Administration of a Recombinant Adenovirus to Individuals with Cystic Fibrosis. I. Methods, Safety, and Clinical Implications. Hum. Gene Ther. 2001, 12, 1369–1382.
- Kuzmin, D.A.; Shutova, M.V.; Johnston, N.R.; Smith, O.P.; Fedorin, V.V.; Kukushkin, Y.S.; van der Loo, J.C.M.; Johnstone, E.C. The Clinical Landscape for AAV Gene Therapies. Nat. Rev. Drug Discov. 2021, 20, 173–174.
- Kochergin-Nikitsky, K.; Belova, L.; Lavrov, A.; Smirnikhina, S. Tissue and Cell-Type-Specific Transduction Using RAAV Vectors in Lung Diseases. J. Mol. Med. 2021, 99, 1057–1071.
- Loring, H.S.; ElMallah, M.K.; Flotte, T.R. Development of RAAV2-CFTR: History of the First RAAV Vector Product to Be Used in Humans. Hum. Gene Ther. Methods. 2016, 27, 49–58.
- da Silva, A.L.; de Oliveira, G.P.; Kim, N.; Cruz, F.F.; Kitoko, J.Z.; Blanco, N.G.; Martini, S.V.; Hanes, J.; Rocco, P.R.M.; Suk, J.S.; et al. Nanoparticle-Based Thymulin Gene Therapy Therapeutically Reverses Key Pathology of Experimental Allergic Asthma. Sci. Adv. 2020, 6, eaay7973.
- Cecchin, R.; Troyer, Z.; Witwer, K.; Morris, K.V. Extracellular Vesicles: The next Generation in Gene Therapy Delivery. Mol. Ther. 2023, 31, 1225–1230.
- Bardoliwala, D.; Patel, V.; Javia, A.; Ghosh, S.; Patel, A.; Misra, A. Nanocarriers in Effective Pulmonary Delivery of SiRNA: Current Approaches and Challenges. Ther. Deliv. 2019, 10, 311–332.
- Shaker, B.; Ahmad, S.; Lee, J.; Jung, C.; Na, D. In Silico Methods and Tools for Drug Discovery. Comput. Biol. Med. 2021, 137, 104851.