Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Ischemia with no obstructive coronary arteries (INOCA) is a relatively newly discovered ischemic phenotype that affects patients similarly to obstructive coronary artery disease (CAD) but has a unique pathophysiology and epidemiology. Patients with INOCA present with ischemic signs and symptoms but no obstructive CAD seen on coronary CTA or invasive coronary angiography, which can assess epicardial vessels.
- INOCA
- CMR
- ischemia with no obstructive coronary arteries
1. Introduction
First discovered in 1973 by Harvey Kemp [1], ischemia with no obstructive coronary arteries (INOCA) refers to patients with stable ischemic symptoms and visually normal or non-obstructive coronary arteries (i.e., <50% reduction in coronary artery diameter appreciated on invasive or CT angiography) [2]. The mechanism of INOCA involves coronary microvascular dysfunction and/or coronary vasospasm, which is explained further below. Though initially considered benign, INOCA is now known to represent true cardiac disease and increases morbidity and mortality. For accurate diagnosis and risk stratification of these patients, a combination of anatomical and functional testing of the epicardial arteries and the microvasculature is crucial [3]. However, diagnostic tests remain underutilized in INOCA [3]; as the current gold standard, coronary reactivity testing is invasive, expensive, and technically challenging [4][5]. Fortunately, non-invasive perfusion imaging techniques are emerging that can provide comparably accurate vasomotor measurements and lower the barrier for evaluation [3][6][7].
2. Epidemiology, Prevalence, Risk Factors, and Outcomes of INOCA
INOCA is a relatively common condition, affecting 3 to 4 million individuals in the United States alone [8]. Among patients undergoing coronary angiography for suspected angina, approximately 60% of women and 30% of men have INOCA [8]. It is thought that this demographic disparity in the prevalence of INOCA is due to sex-related differences in normal cardiac physiology as well as a heterogenous representation of risk factors in women compared to men [8]. There are several risk factors associated with INOCA, including traditional cardiovascular risk factors (i.e., hypertension, diabetes, hyperlipidemia, age, and smoking), non-traditional risk factors (i.e., psychosocial stress, autoimmune disorders, and hormonal changes), female sex, and postmenopausal status [9][10]. There is also growing evidence for drug-induced INOCA, including one study that found microvascular disease associated with the use of anthracycline [11].
Several studies have highlighted the significant morbidity and mortality associated with INOCA, including an increased risk of major adverse cardiac events (MACE), heart failure with preserved ejection fraction (HFpEF), stroke, and coronary microvascular dysfunction (CMD) [9][10]. INOCA has been found to increase the risk of MACE 1.5–1.8-fold and the risk of all-cause mortality 1.3–1.5-fold [9][10][12]. The WISE study demonstrated that symptomatic women with INOCA experienced a 10-fold increase in heart failure hospitalizations compared to healthy asymptomatic women [10]. Overall, INOCA reduces a patient’s quality of life with increased symptom burden, cardiac anxiety, emergency room visits, and repeated testing with invasive angiography [13][14]. INOCA also comprises a substantial healthcare burden, with costs comparable to obstructive CAD [9]. It accounts for almost half of all angiography procedures [10][15].
Unfortunately, INOCA is often under-detected and undertreated in both men and women due to limitations in the current diagnostic tools, inadequate awareness, and bias [3]. Early identification and appropriate management of INOCA are essential to reduce the risk of adverse outcomes in affected individuals.
3. INOCA Endotypes: Pathophysiology and Current Diagnostic Criteria
The coronary microvasculature (especially the small arterioles) provides a significant component of the overall coronary vascular resistance and is thereby a pivotal regulator of myocardial blood flow [16]. Disturbances in the microvascular structure and/or vasodilator responses can lead to INOCA [16].
The two endotypes of INOCA include microvascular dysfunction (MVD) and vasospastic angina (VSA). They represent distinct but frequently coexistent mechanisms [17]. A meta-analysis examining the distribution of these endotypes found that approximately 41% of INOCA cases are MVD, 40% are VSA, and 23% are a combined endotype [3]. Table 1 outlines the diagnostic criteria for each endotype and compares them to non-cardiac chest pain [18].
Table 1. Diagnostic criteria for INOCA endotypes and non-cardiac chest pain.
| Diagnosis | Diagnostic Criteria |
|---|---|
| Microvascular dysfunction (MVD) * |
|
| Vasospastic angina (VSA) ** |
|
| Non-cardiac chest pain |
|
Physiologically, endothelium-independent and endothelium-dependent vasodilator responses regulate the coronary vasculature [16]. Adenosine, which is released by cardiac tissue in the setting of insufficient oxygen supply, stimulates endothelium-independent vasodilation in the microvasculature in order to increase myocardial blood flow (MBF) [16]. This process then promotes flow-mediated acetylcholine (ACh) release, which triggers the endothelium to produce nitric oxide (NO), causing endothelium-dependent vasodilation in larger epicardial and microvascular vessels [16][17]. ACh also induces smooth muscle vasoconstriction, but normally, endothelium-dependent vasodilation predominates [19][20]. Additionally, other chemical stimuli like histamine, bradykinin, serotonin, adenosine diphosphate (ADP), substance P, and thrombin can trigger NO release, contributing to further vasodilation [16].
Aberrancies in the above pathway can lead to INOCA [16]. Just as atherosclerotic vascular disease is known to involve remodeling of the arteries, the coronary microvasculature can develop structural changes that can impair vasodilation and flow. The coronary arteries may also develop functional dysregulation, leading to enhanced response to vasoconstrictive stimuli. When the endothelium fails to release NO in response to ACh, ACh will induce unrestrained smooth muscle vasoconstriction, leading to vasospasm [19]. The physiology of coronary vasodilation and pathophysiology of INOCA are illustrated in Figure 1.
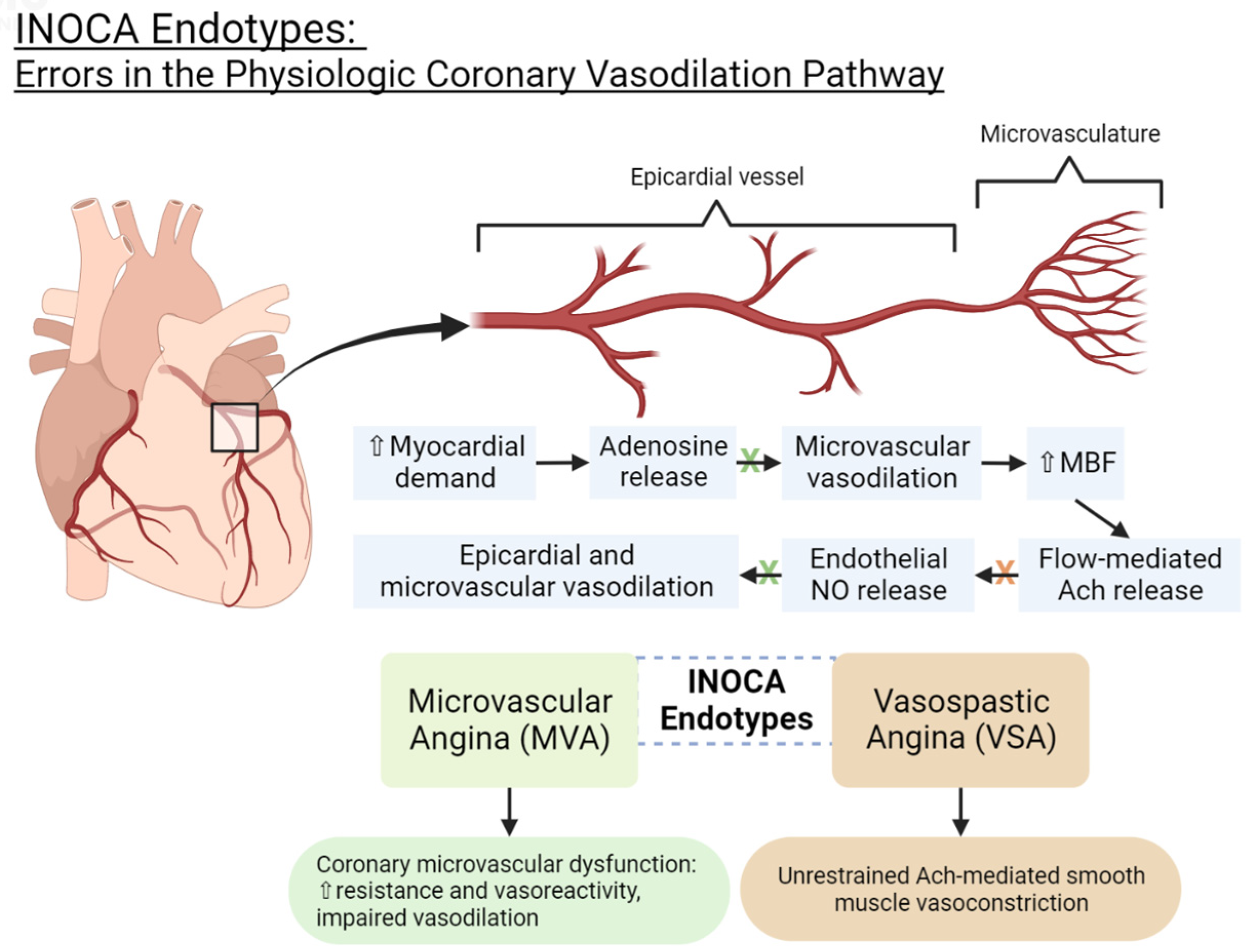
Figure 1. INOCA endotypes: errors in the physiologic coronary vasodilation pathway. NO = nitric oxide. Ach = acetylcholine. MBF = myocardial blood flow.
3.1. Microvascular Dysfunction Endotype (MVD)
The MVD endotype is characterized by coronary microvascular disease due to structural remodeling and/or microvascular vasospasm. Structural remodeling in the microvasculature leads to an increased wall-to-lumen ratio and a loss of myocardial capillary density (capillary rarefaction) [17]. This increases the index of microvascular resistance (IMR) and impairs vasodilation [17]. Traditional cardiovascular risk factors (i.e., smoking, hypertension, hyperlipidemia, diabetes, insulin resistance, and obstructive CAD), left ventricular hypertrophy, and cardiomyopathies can predispose one to structural microvascular remodeling, which can decrease microvascular vasodilatory capacity and limit the blood and oxygen reserve to the myocardium in response to stress or exercise [17]. Microvascular vasospasm due to enhanced vasoreactivity may also comprise part of MVD’s pathophysiology.
The current criteria for diagnosing MVD include the clinical presence of myocardial ischemia (i.e., symptoms of angina and/or ECG changes during stress testing), the absence of obstructive CAD on coronary CTA or invasive angiography, and evidence of microvascular dysfunction on invasive or non-invasive coronary reactivity testing [4]. The findings of coronary microvascular dysfunction include a measurement of CFR ≤ 2 or 2.5 after adenosine administration, an IMR > 25, and/or a corrected TIMI frame count ≥ 3 beats to fill a vessel [4][21][22].
3.2. Vasospastic Angina Endotype (VSA)
As opposed to the microvascular disease found in MVD, VSA is characterized by epicardial dysfunction without evidence of obstruction. Though functional dysregulation may lead to enhanced vasoconstriction in either epicardial and/or microvascular vessels [17], VSA is defined by coronary vasospasm that is predominately evidenced in the epicardial vessels [19][20][23].
According to the COVADIS criteria, definitive vasospastic angina is diagnosed when nitrate-responsive angina (either during a spontaneous episode or due to a trigger such as exercise, hyperventilation, or acetylcholine stimulation) is accompanied by either transient ischemic electrocardiographic changes (e.g., ST elevation or depression ≥ 0.1 mV, new negative U-wave) or coronary artery spasm (e.g., >90% coronary artery constriction) [5].
This entry is adapted from the peer-reviewed paper 10.3390/medicina59091570
References
- Kemp, H.G.; Kronmal, R.A.; Vlietstra, R.E.; Frye, R.L. Seven year survival of patients with normal or near normal coronary arteriograms: A CASS registry study. J. Am. Coll. Cardiol. 1986, 7, 479–483.
- Ford, T.J.; Stanley, B.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; Robertson, K.; et al. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina: The CorMicA Trial. J. Am. Coll. Cardiol. 2018, 72, 2841–2855.
- Mileva, N.; Nagumo, S.; Mizukami, T.; Sonck, J.; Berry, C.; Gallinoro, E.; Monizzi, G.; Candreva, A.; Munhoz, D.; Vassilev, D.; et al. Prevalence of Coronary Microvascular Disease and Coronary Vasospasm in Patients With Nonobstructive Coronary Artery Disease: Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2022, 11, 23207.
- Ong, P.; Camici, P.G.; Beltrame, J.F.; Crea, F.; Shimokawa, H.; Sechtem, U.; Kaski, J.C.; Bairey Merz, C.N. International standardization of diagnostic criteria for microvascular angina. Int. J. Cardiol. 2017, 250, 16–20.
- Beltrame, J.F.; Crea, F.; Kaski, J.C.; Ogawa, H.; Ong, P.; Sechtem, U.; Shimokawa, H.; Bairey Merz, C.N. International standardization of diagnostic criteria for vasospastic angina. Eur. Heart J. 2017, 38, 2565–2568.
- Van Dijk, R.; Van Assen, M.; Vliegenthart, R.; De Bock, G.H.; Van Der Harst, P.; Oudkerk, M. Diagnostic performance of semi-quantitative and quantitative stress CMR perfusion analysis: A meta-analysis. J. Cardiovasc. Magn. Reson. 2017, 19, 92.
- Kelshiker, M.A.; Seligman, H.; Howard, J.P.; Rahman, H.; Foley, M.; Nowbar, A.N.; Rajkumar, C.A.; Shun-Shin, M.J.; Ahmad, Y.; Sen, S.; et al. Coronary flow reserve and cardiovascular outcomes: A systematic review and meta-analysis. Eur. Heart J. 2022, 43, 1582–1593.
- Pepine, C.J.; Ferdinand, K.C.; Shaw, L.J.; Light-McGroary, K.A.; Shah, R.U.; Gulati, M.; Duvernoy, C.; Walsh, M.N.; Bairey Merz, C.N. The Present and Future Emergence of Nonobstructive Coronary Artery Disease A Woman’s Problem and Need for Change in Definition on Angiography. J. Am. Coll. Cardiol. 2015, 66, 1918–1933.
- Jespersen, L.; Hvelplund, A.; Abildstrøm, S.Z.; Pedersen, F.; Galatius, S.; Madsen, J.K.; Jørgensen, E.; Kelbæk, H.; Prescott, E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur. Heart J. 2012, 33, 734–744.
- Gulati, M.; Cooper-DeHoff, R.M.; McClure, C.; Johnson, B.D.; Shaw, L.J.; Handberg, E.M.; Zineh, I.; Kelsey, S.F.; Arnsdorf, M.F.; Black, H.R.; et al. Adverse Cardiovascular Outcomes in Women With Nonobstructive Coronary Artery Disease: A Report From the Women’s Ischemia Syndrome Evaluation Study and the St James Women Take Heart Project. Arch. Intern. Med. 2009, 169, 843–850.
- Klotzka, A.; Iwańczyk, S.; Ropacka-Lesiak, M.; Misan, N.; Lesiak, M. Anthracycline-induced microcirculation disorders: AIM PILOT Study. Kardiol. Pol. 2023.
- Gulati, M.; Parwani, P. Myocardial Blood Flow Reserve: The Achilles’ Heel of CAD Prognostication? JACC Cardiovasc. Imaging 2022, 15, 1645–1647.
- Ford, T.J.; Stanley, B.; Sidik, N.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; et al. 1-Year Outcomes of Angina Management Guided by Invasive Coronary Function Testing (CorMicA). JACC Cardiovasc. Interv. 2020, 13, 33–45.
- Heggie, R.; Briggs, A.; Stanley, B.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; et al. Stratified medicine using invasive coronary function testing in angina: A cost-effectiveness analysis of the British Heart Foundation CorMicA trial. Int. J. Cardiol. 2021, 337, 44–51.
- Maddox, T.M.; Stanislawski, M.A.; Grunwald, G.K.; Bradley, S.M.; Ho, P.M.; Tsai, T.T.; Patel, M.R.; Sandhu, A.; Valle, J.; Magid, D.J.; et al. Nonobstructive Coronary Artery Disease and Risk of Myocardial Infarction. JAMA 2014, 312, 1754.
- Carlos Plana, J.; Jones, P.H. The Use of Statins in Acute Coronary Syndromes: The Mechanisms Behind the Outcomes. Curr. Atheroscler. Rep. 2001, 3, 355–364.
- Jansen, T.P.J.; Konst, R.E.; Elias-Smale, S.E.; van den Oord, S.C.; Ong, P.; de Vos, A.M.J.; van de Hoef, T.P.; Paradies, V.; Smits, P.C.; van Royen, N.; et al. Assessing Microvascular Dysfunction in Angina With Unobstructed Coronary Arteries: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2021, 78, 1471–1479.
- Parwani, P.; Kang, N.; Safaeipour, M.; Mamas, M.A.; Wei, J.; Gulati, M.; Naidu, S.S.; Merz, N.B. Contemporary Diagnosis and Management of Patients with MINOCA. Curr. Cardiol. Rep. 2023, 25, 561–570.
- Pargaonkar, V.S.; Lee, J.H.; Chow, E.K.H.; Nishi, T.; Ball, R.L.; Kobayashi, Y.; Kimura, T.; Lee, D.P.; Stefanick, M.L.; Fearon, W.F.; et al. Dose-Response Relationship between Intracoronary Acetylcholine and Minimal Lumen Diameter in Coronary Endothelial Function Testing of Women and Men with Angina and No Obstructive Coronary Artery Disease. Circ. Cardiovasc. Interv. 2020, 13, 8587.
- Godo, S.; Suda, A.; Takahashi, J.; Yasuda, S.; Shimokawa, H. Coronary Microvascular Dysfunction. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1625–1637.
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 407–477.
- Beltrame, J.F.; Limaye, S.B.; Horowitz, J.D. The Coronary Slow Flow Phenomenon—A New Coronary Microvascular Disorder. Gen. Cardiol. Cardiol. 2002, 97, 197–202.
- Noel, C.; Merz, B.; Pepine, C.J.; Walsh, M.N.; Fleg, J.L.; Vincent, S. Ischemia and No Obstructive Coronary Artery Disease (INOCA): Developing Evidence-based Therapies and Research Agenda for the Next Decade. Circulation 2017, 135, 1075–1092.
This entry is offline, you can click here to edit this entry!