Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Cell Biology
Mesenchymal stem cell extracellular vesicles (MSCEVs) obtained from MSCs can have numerous therapeutic applications via regeneration of various body tissues. MSCEV action can be potentiated by modifying the mesenchymal stem cells culturing methodology and bioengineering extracellular vesicles (EVs).
- extracellular vesicles
- regenerative potential
- therapeutics
1. MSCEVs and Cardiac Tissue Regeneration
Endogenous repair of damaged myocardium is usually slow and depends on the inadequate division of pre-existing cardiomyocytes and recruitment and differentiation of local cardiac stem cells [29,30]. Exogenous MSCEVs address the inadequate response to myocardial injury. Preliminary investigation recognized the ability of human embryonic-derived MSCEVs (EMSCEVs) to reduce the size of infarct in a myocardial ischemia/reperfusion injury (MI) mouse model [31] by activating the PI3K/Akt signaling pathway, which increases myocardial viability and inhibits adverse remodeling [32]. Based on this, human Akt-transfected umbilical cord-derived MSCEVs (UCMSCEVs) were developed, which exhibited enhanced endothelial cell proliferation, migration, and blood vessel formation in vivo and tube-like structures in vitro, compared to nonmodified human UCMSCEVs [33].
A study revealed that human amniotic fluid-derived mesenchymal stem cells (AFMSCs) and murine-induced pluripotent mesenchymal stem cells (iPMSCs) triggered cardiac regeneration via paracrine modulation of endogenous mechanisms and improved cardiac repair in an MI murine model. Administration of iPMSCEVs was shown to be safer compared to iPMSCs [34,35]. Another MI rat model study revealed that combination treatment of rat bone marrow mesenchymal stem cells (BMMSCs) and derived BMMSCEVs improved cardiac functioning, reduced infarct size, and increased neo-vascularization compared to individual treatment with BMMSCs or BMMSCEVs [36].
Human BMMSCs preconditioned with hypoxia improved in vitro cell biological activity [37]. The report suggests that the efficacy of BMMSCs from Cynomolgous monkeys improves when implanted for treatment of MI in monkeys [38]. Hypoxia enhanced the therapeutic effectiveness of secretory EVs, such that hypoxia conditioned human BMMSCEVs with 1% O2 for 3 days exhibit more cardiac regeneration in the rat MI model compared to BMMSCEVs in normoxic conditions. The report suggests that the underlining mechanism is increased angiogenesis at the infract site [39]. Hypoxia reconditioned with murine and rat BMMSCEVs (at 1% O2 for 72 h or 0.5% O2 for 24 h) inhibited apoptosis of cardiomyocytes by enriching miR-125b-5p-EV and miR-210-EV. In this case, the underline mechanism is the suppression of proapoptotic p53 and BCL2-antagonist/killer 1 (BAK1) genes and higher recruitment of cardiac progenitor cells in the infarcted heart [40,41]. MSCEVs, when encapsulated as a hydrogel, offer targeted and controlled delivery to cardiac defects. For example, a sustained release profile and higher cardiac regeneration are provided by human UCMSCEVs loaded in peptide hydrogel. The EV/hydrogel complex improves myocardial functioning via reduction of apoptosis, inflammation, and fibrosis and enhancement of angiogenesis in the infarcted boundary zone of rat hearts [42].
2. MSCEVs and Nervous Tissue Regeneration
A small injury or disease in the nervous system may lead to serious or lethal effects. The complex physiological system and limited healing capacity present the biggest challenge to nerve repair in regenerative medicine [43]. Various studies reported the repair of injured peripheral nerves (PNs) by different MSCEVs. For example, rat bone marrow MSCEVs (BMMSCEVs) regenerated injured sciatic PNs using a rat model. BMMSCEVs exhibited higher growth-associated protein (GAP43) expression, improved histomorphometric repair, and enhanced the sciatic functioning index [44]. Similarly, human umbilical cord MSCEVs (UCMSCEVs) were reported to regenerate PNs at the sites of sciatic nerve defects (SNDs) in rats. Accumulation of UCMSCEVs at the site of injured PNs stimulates axons and generates Schwann cells to fence off individual axons, reduce muscle atrophy (denervated), and modulate inflammation by upregulating anti-inflammatory cytokines (e.g., interleukin (IL)-10) and downregulating pro-inflammatory cytokines (e.g., IL1β and IL6) [45]. Rat adipose-derived MSCEVs (AMSCEVs) are also known to promote PN regeneration and neurite growth in sciatic PN defects via Schwann cell modulation [46]. The AMSCEV perinuclear location and accumulation in vesicular-like structures in Schwann cells stimulate and proliferate damaged cells, thereby indicating an endocytosis facilitated internalization pathway [47]. PN regeneration by gingiva MSCEVs (GMSCEVs) indicates proliferation and migration of Schwann cells through activation of the c-Jun N-terminal kinase (JNK) pathway and upregulation of Notch1, c-Jun, glial fibrillary acidic protein (GFAP), and Sox2 genes for de-differentiation or repair of the Schwann cell phenotype [48].
MSCEVs also have therapeutic potential to repair the central nervous system (CNS). Reports suggest that BMMSCEVs cause neurite development (via miR-133b transfer into neural cells) in a middle cerebral artery (MCA) stroke rat model [49]. BMMSCEV administration raised the axon density and synaptophysin-positive area (along the ischemic zone of striatum and cortex) and increased the expression of von Willebrand factor (endothelial cell marker) and doublecortin (neuroblast marker) in MCA rats [50,51], which suggest their potential for neurite remodeling, angiogenesis, and neurogenesis in stroke treatment [52].
BMMSCEVs, when evaluated for their potential in traumatic brain injury (TBI) using a rat model, showed improvement in the recovery of brain functioning by enhancing the counts of new immature and mature neurons in the dentate gyrus and new endothelial cells in the lesion boundary and dentate gyrus [53]. MSCEVs have also shown potential in the recovery of spinal cord injury (SCI) characterized by disrupted microvascular stability and high blood–spinal cord barrier (BSCB) permeation (due to pericyte migration) [54,55]. Mouse BMMSCEV treatment inhibited pericyte migration, thus improving BSCB structural integrity and motor functioning in an SCI rat model [56].
Another mechanism for SCI recovery by BMMSCEVs suggests the inhibition of neuronal apoptosis via activation of the Wnt/β-catenin signaling pathway [57]. Modification of rat BMMSCEVs with miR-133b activated the ERK1/2 and STAT3 pathways in the SCI model, which enhanced axon regeneration, neuron preservation, and locomotor functioning, compared to BMMSCEVs that were not modified with miR-133b [58]. Human placental MSCEVs (PMSCEVs) exhibited regeneration of myelin through differentiation of oligodendrocyte precursor cells (endogenous) into myelinating oligodendrocytes in vitro and enhanced myelination in the spinal cord of treated mice (multiple sclerosis model), followed by improved motor functioning [59]. Human BMMSCEVs stimulated by interferon-gamma (IFN-γ) exhibited a reduction in demyelination and neuroinflammation, thereby improving motor skills, in a multiple sclerosis experimental autoimmune encephalomyelitis (EAE) mouse model [60]. Also, in an Alzheimer disease mouse model, MSCEVs enhanced neurogenesis and cognitive function recovery [61].
Evidence suggests that neonatal hypoxic ischemic (HI) encephalopathy is one of the major reasons for newborn disability and death. MSCEVs exert a regenerative effect on HI encephalopathy; for example, a study reported the neuroprotective effect of MSCEVs in a Rice–Vannucci mouse model of severe HI-induced neonatal brain insult [62]. Another study found protective effects of MSCEVs in a preclinical model of preterm HI brain injury. The study involved in utero intravenous administration of MSCEVs into ovine fetuses with induced global HI. The study revealed that MSCEV administration improved the functioning of the brain via a reduction of seizure duration and count and preservation of the reflex sensitivity of baroreceptors [63].
3. MSCEVs and Bone Regeneration
MSCEVs provide excellent benefits in skeletal regeneration. To date, various MSCEVs have been tested for their potential in regeneration of injured bone. Human iPMSCEVs and BMMSCEVs enhanced in vitro osteogenic differentiation of BMMSCs on the one hand, and in vivo angiogenesis and bone formation in a rat model with a critical-sized calvarial defect, on the other hand [64,65]. The report suggests that dimethyl-oxaloyl glycin human BMMSCEVs stimulate angiogenesis via the Akt/mTOR pathway [66]. The efficacy of ADMSCEVs for bone regeneration can be enhanced via pre-conditioning of ADMSCs with the cytokine tumor necrosis factor alpha (TNF-α). This is based on the proliferation and osteogenic differentiation of osteoblastic cells in an in vitro experiment [67]. The study revealed that human BMMSCEV administration in a CD9 mouse model with femoral shaft fracture (with impaired bone healing ability) improved fracture healing [68].
In dental regeneration, administration of human dental pulp MSCEVs (DPMSCEVs) causes in vitro odontogenic differentiation. This is based on DPMSCEV endocytosis, which stimulated the P38 MAPK pathway and regenerated dental pulp-like tissue in a tooth root slice model [69]. MSCEVs are known to stimulate the migration and proliferation of periodontal ligament cells via CD73-facilitated adenosine receptor activation of pro-survival Akt and ERK signaling and periodontal regeneration in a periodontal defect rat model [70]. For improved performance of scaffold and bone healing, MSCEVs are combined with tissue-engineered constructs. For example, human ADMSCEVs are immobilized with biotin-doped polypyrrole titanium and poly (lactic-co-glycolic acid) scaffolds. In vitro investigations of BMMSCEV-based and unmodified scaffolds revealed that BMMSCEV scaffolds led to high osteoinduction of BMMSCs and osteoblasts, whereas in vivo studies with a murine model of bone defect showed improved collagen and bone tissue formation [71]. Loading of human BMMSCEVs into the tricalcium phosphate scaffold enhanced bone healing of calvarial defects via activation of the PI3K/Akt signaling pathway [72]. The report suggests that rat BMMSCEVs encapsulated in decalcified bone matrix scaffold stimulates bone regeneration by promoting vascularization in grafts [73].
4. MSCEVs and Liver Tissue Regeneration
Human embryonic MSCEVs are known to promote hepatic regeneration in a carbon tetrachloride (CCl4)-induced liver injury mouse model by increasing the proliferation of hepatocytes and reducing their apoptosis [74]. A report suggests that human iPMSCEVs cause regeneration of hepatic cells in a hepatic ischemia–reperfusion injury rat model via inhibition of hepatocyte apoptosis, suppression of inflammatory response, and attenuation of the oxidative stress response [75]. Human iPMSCEVs are also known to induce in vitro and in vivo proliferation of hepatocytes (in a dose-dependent manner), which is related to the activation of the sphingosine kinase and sphingosine-1-phosphate signaling pathway (which promotes cell proliferation) [76,77]. The ability of UCMSCEVs to ameliorate neutrophil infiltration and inhibit oxidative stress in hepatic tissue supports their property of protecting against hepatic apoptosis [78]. The benefits of human embryonic MSCEVs can be further enhanced by encapsulating them into PEG hydrogel, intended to sustain systemic delivery against hepatic failure. MSCEV accumulation in the liver for a prolonged period of time in a chronic hepatic fibrosis rat model had superior antiapoptotic, antifibrotic, and regenerative properties compared to conventional MSCEV administration [79].
5. MSCEVs and Kidney Regeneration
Many studies have reported the regenerative potential of MSCEVs in chronic kidney damage (CKD) and acute kidney injury (AKI). An earlier study reported that human BMMSCEVs stimulated cell proliferation, hastened the recovery of injured tubular cells, supported the functional recovery of glycerol-induced AKI, and prevented apoptosis [80]. MSCEVs exhibit their therapeutic actions using several mechanisms. One mechanism includes transportation of genetic material (mRNAs and miRNAs) to renal cells (injured), which exerts antiapoptotic, proangiogenetic, anti-inflammatory, and antifibrotic effects on AKI [81]. The second mechanism involves the parallel transfer of human IGF-1 receptor mRNA (present in MSCEVs) into tubular cells [82]. Administration of mouse and human BMMSCEVs in rat and mouse AKI models caused protection from AKI and enhanced renal functioning by stimulating tubular epithelial cell proliferation and inhibiting apoptosis [83]. The study showed that human BMMSCEVs ameliorated kidney morphology and functioning in a cisplatin-induced AKI mouse model. Based on this, an in vitro study of cisplatin-treated human tubular epithelial cells showed that BMMSCEVs upregulated antiapoptotic genes (β-cell lymphoma 2, β-cell lymphoma, extra-large and baculoviral IAP repeat-containing 8) and downregulates the genes that participate in the execution phase of cell apoptosis (caspase-1,8 and α-lymphotoxin) [84].
For controlled and targeted release at the site of AKI (after ischemia–reperfusion) in a mouse model, loading mouse BMMSCEVs onto self-assembling peptide nanofiber hydrogel provides a substantial increase in efficacy (improved renal function) [85]. Human UCMSCEVs are reported to induce in vitro and in vivo kidney repair in a cisplatin-induced AKI rat model by de-differentiation of tubular cells, promotion of cell proliferation, and reduction in cell apoptosis and oxidative stress [86]. Renal regeneration is also exhibited by human Wharton’s jelly MSCEVs when administered in an AKI rat model. These MSCEVs improvise renal functioning by augmenting tubular cell proliferation and reducing apoptosis and inflammation through mitochondrial fission [87]. Human glomerular and liver MSCEVs are also reported to stimulate recovery after AKI [88]. A study reported the MSCEV effect in diabetes-associated chronic kidney damage (CKD) [89].
Human urinary MSCEVs (UMSCEVs) are known to prevent the progression of CKD through the promotion of vascular regeneration, inhibition of podocyte apoptosis, and cell survival in a streptozotocin-induced diabetic nephropathy rat model [90]. The administration of UMSCEVs in diabetic mice showed improved renal morphology and anti-apoptotic performance of tubular epithelial cells [91]. A report suggested that human BMMSCEVs and liver MSCEVs prevent fibrosis and its progression in a diabetic nephropathy mouse model mediated by miRNA (profibrotic gene downregulator) [92]. Similar action was reported with the administration of human liver MSCEVs in an aristolochic acid-induced CKD model [93]. The Murine BMMSCEVs also exhibit protective action after renal injury in vitro and in vivo [94]. The administration of human BMMSCEVs has the potential to repair damaged mitochondria renal proximal tubule apical/basolateral membranes and improve renal functioning in a medaka model of cadmium exposure that resembles CKD on long-term exposure to heavy metals [95]. A clinical trial of 40 patients with stage III and IV CKD (n = 20 administered MSCEVs, n = 20 administered placebo) reported that UCMSCEVs provided safety and ameliorated CKD progression [96].
6. MSCEVs and Muscle Regeneration
MSCEVs also show potential in skeletal muscle regeneration. For example, human BMMSCEVs can potentially augment myogenesis and angiogenesis in vitro (mediated by miR-494) and enhance muscle regeneration [97]. Amniotic fluid MSCEVs comprise several proteins and miRNAs that can regulate inflammation and angiogenesis, boosting skeletal muscle regeneration [98]. A bioinformatics study (miRNA profiling and proteomics) that evaluated the regenerative potential of human AMSCEVs in muscle injury revealed that repair was mediated by factors that were distributed in both MSCEVs and the soluble fraction of secretomes [99].
Reports suggest that human AMSC treatment protects from muscle injury associated with torn rotator cuff. MSCEV treatment in a rat model inhibited atrophy, fatty infiltration, inflammation, and vascularization of muscles in torn rotator cuffs, and enhanced the myofiber regeneration and biomechanical properties [100]. MSCEVs derived from human urine are also known to promote the repair of pubococcygeus muscle injury in a stress urinary incontinence rat model. This is done via stimulation of extracellular regulated protein (ERP) kinase phosphorylation and activation, proliferation, and differentiation of muscle satellite cells [101]. In addition, human ASCEVs were also reported to prevent muscle damage in a mouse model of critical hindlimb ischemia via neuregulin 1 protein (NRG1)-mediated signals, which play an important role in angiogenesis, muscle protection, and prevention of inflammation [102].
7. MSCEVs and Cartilage Regeneration
Injured articular cartilage has restricted endogenous regeneration ability. Poor healing of cartilage may result in osteoarthritis (OA) [103]. A study highlighted the therapeutic action of MSCEVs on their cellular origin during OA treatment. The study compared amniotic fluid MSCs (AFMSCs) and AFMSCEVs. Animals with defects treated using AFMSCEVs exhibited higher pain tolerance and histological scores compared to AFMSCs [104]. Human BMMSCEVs stimulate in vitro regeneration of cartilage by triggering type-2 collagen and proteoglycans of chondrocyte production, which assists in cartilage repair [105]. OA is related to cartilage degradation via Wnt5A (noncanonical Wnt protein), which activates matrix metalloproteinase (MMP) and reduces cartilage ECM formation [106]. Another investigation suggests that miR92a-3p enriched human BMMSCEVs suppress degradation of cartilage and stimulate cartilage repair in an OA mouse model in vitro as well as in vivo, attributed to miR-92a-3p targeting Wnt5A [107]. Also, pre-conditioning of rat MSCs with transforming growth factor beta (TGFβ) increases the quantity of miR-135b in derived EVs, which causes stimulation of chondrocyte proliferation in vitro via specificity protein 1 (Sp1) regulation and cartilage tissue repair in an OA rat model [108].
A study suggests that administration of human embryonic MSCEVs in an osteochondral defect rat and mouse model caused osteochondral regeneration through well-arranged mechanisms, such as augmentation of chondrocyte proliferation, attenuation of apoptosis, and regulation of immunoreactivity at the injury site, along with formation of balance and degradation of cartilage ECM, and restoration of matrix homeostasis [109,110]. Three-dimensional culture of UCMSCs in a hollow-fiber bioreactor resulted in high yield and exceptional therapeutic potential of UCMSCEVs in a cartilage defect rabbit model compared to MSCEVs from a conventional 2D culture [111]. To retain MSCEVs at the cartilage injury site, human iPSCEVs can be incorporated in situ with hydrogel glue. Such cellular tissue patches can assimilate with the native cartilage matrix and enhance cell deposition at cartilage defect sites, thereby resulting in cartilage repair [112]. Three-dimensional printing is an advanced fabrication technique for tissue engineering that enables the development of complex forms with high precision [113]. BMMSCEVs are fabricated with cartilage ECM/gelatin methacrylate hydrogel as a bio-ink to design bio-scaffolds. The 3D-printed device enables target delivery of BMMSCEVs to prevent mitochondrial dysfunction in degenerative chondrocytes in vitro and to assist in cartilage regeneration in an osteochondral defect rabbit model in vivo [114].
8. MSCEVs and Wound Healing
The wound healing process involves complex molecular and cellular events, such as angiogenesis, cellular migration, ECM deposition, proliferation, and tissue remodeling [115]. Wounds with impaired healing fail to progress via normal healing stages (inflammation, homeostasis, proliferation, and remodeling), which leads to excessive scar formation [116]. MSCEVs exhibit beneficial effects in several chronic types of wounds. A study demonstrated that BMMSCEVs enhanced fibroblast proliferation and migration in healthy people and chronic wound patients (in a dose-dependent manner) ex vivo, and mediated tube formation by endothelial cells via activation of Akt, ERK, and STAT3 wound healing pathways [117]. An in vitro study suggested that human iPSCEVs had potential in cutaneous wound healing, by increasing collagen synthesis and angiogenesis [118]. AMSCEVs also showed the potential to increase collagen and elastin synthesis in photodamaged human dermal fibroblasts in vitro [119]. In vivo administration of AMSCEVs using a mouse skin incision model showed increased wound healing by modification of the phenotype character of fibroblasts. Collagen 1 and 3 secretion from fibroblasts increases during an early stage of wound healing, whereas collagen synthesis diminishes to reduce scar formation during the later stages [120]. A report suggested that AMSCEVs trigger keratinocyte and fibroblast migration and proliferation in an excisional wound splinting rat model via activation of the Akt pathway [121]. A comparative study of BMMSCEVs and rabbit ADMSCEVs in a rat cutaneous wound model showed significant healing [122]. Human UCMSCEVs are known to promote healing of second-degree burn wounds in vivo by activating the Wnt/β-catenin signaling pathway, increasing dermal fibroblast proliferation and angiogenesis, and reducing skin cell apoptosis [123,124]. Wound healing and suppressed scar formation are facilitated by inhibition of myofibroblast differentiation at the site of the skin defect upon treatment with human UCMSCEVs. Such effect is attributed to the activity of specific microRNAs (miR-21, 23a, 125b, and 145) [125].
9. MSCEVs and Other Tissue Regeneration
Apart from their regenerative potential in the mentioned organs and tissues, MSCEVs have regenerative potential against injuries or diseases of several other organs, such as blood vessels, esophagus, lung, and bowel. For example, human placenta MSCEVs attenuated in vitro lung cell injury (by lipopolysaccharide stimulation) [126]; swine BMMSCEVs improved in vivo lung functioning in a pig model of influenza virus-induced acute lung injury [127]; human BMMSCEVs alleviated pulmonary vascular permeability and lung injury (induced by hemorrhagic shock and trauma) in a mouse model (via activation of proteins and pathways linked to cytoskeletal rearrangement of vascular permeability) [128]; and human placenta MSCEVs inhibited calcification of synthetic vascular grafts by immunomodulation and improved vascular performance and functionality in a hyperlipidemia rat model [129].
In the same way, AMSCEVs limit abnormal proliferation and migration of vascular smooth muscle cells, and neointimal hyperplasia in vein graft bypass surgery [130]; Mouse BMMSCEVs are known to improve ulcerative colitis symptoms in a dextran sodium sulfate-induced mouse model [131]; and human UCMSCEVs ameliorate severe ischemic injury in a hindlimb ischemia mouse model [132]. AMSCEVs (inserted into thermo response hydrogels) are also known to augment healing and ensure target delivery at the site of disease in cases of tracheoesophageal diseases like fistula [133]. Similarly, numerous MSCEVs are applied in tissue engineering of various tissues and organs (Figure 1).
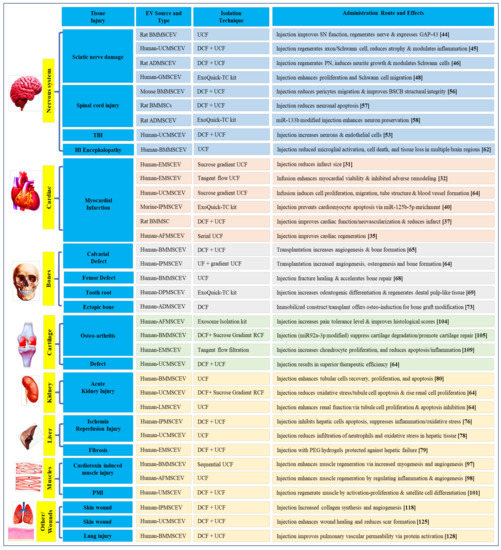
Figure 1. Applications of mesenchymal stem cells derived extracellular vesicles (MSCEVs) in tissue engineering.
This entry is adapted from the peer-reviewed paper 10.3390/biology10030172
This entry is offline, you can click here to edit this entry!