Up to 20% of patients with ischemic stroke or transient ischemic attack have a prior history of known atrial fibrillation (AF). Additionally, unknown AF can be detected by different monitoring strategies in up to 23% of patients with cryptogenic or non-cardioembolic stroke. However, most studies had substantial gaps in monitoring time, especially early after the index event. Following this, AF rates would be higher if patients underwent continuous monitoring early after stroke, avoiding any gaps in monitoring. The few existing randomized studies focused on patients with cryptogenic stroke but did not focus otherwise specifically on prevention strategies in patients at high risk for AF (patients at higher age or with high CHA2DS2-VASC scores). Besides invasive implantable loop recorders (ILRs), external loop recorders (ELRs) and mobile cardiac outpatient telemetry (MCOT) are non-invasive tools that are commonly used for long-term ECG monitoring in cryptogenic-stroke patients in the ambulatory setting.
1. Introduction
Stroke is one of the leading causes of death and disability worldwide. In ischemic stroke, comorbidities can suggest an embolic cause, but frequently a specific source cannot be identified. Following this, the term “embolic stroke of undetermined source” (ESUS) designates patients with non-lacunar ischemic stroke where embolism could be the likely stroke mechanism [
1]. Despite advancements in medical technology, the cause of ischemic stroke remains undetermined in approximately one third of cases [
2]. This is also termed “cryptogenic stroke” (CS). Risk of stroke is increased five-fold in atrial fibrillation (AF) [
3] independently of whether AF is paroxysmal or persistent [
4]. Up to 20% of patients with ischemic stroke have a previous history of AF, but incidence rates increase steeply with age [
5]. In stroke patients >80 years of age the incidence of AF-related stroke has increased three-fold during the last 35 years, and another three-fold increase is expected by 2050 [
5]. Detection of AF is of central importance after stroke or transient ischemic attack (TIA), as risk of recurrent stroke can be effectively reduced by oral anticoagulation with warfarin [
6] and novel oral anticoagulants [
7]. This strategy has a huge impact on secondary prevention [
8]. Prolonged electrocardiogram (ECG) monitoring is appropriate in patients with CS and transient ischemic attack (TIA) who have a negative baseline diagnostic workup. This workup usually includes inpatient telemetry and at least 24 h outpatient Holter monitoring [
8]. The strategy of long-term monitoring is used to substantially increase the probability of AF detection in patients with CS. When AF is detected in time, early initiation of anticoagulation therapy can have a huge impact on recurrent-stroke prevention in these patients [
9]. Long-term electrocardiogram (ECG) monitoring tools are commonly used for paroxysmal AF detection, and proof of their accuracy and the reliability of detection algorithms should be of eminent interest. Current methods of ECG monitoring include invasive and non-invasive methods [
10]. External loop recorders (ELRs) and mobile cardiac outpatient telemetry (MCOT) are ambulatory non-invasive diagnostic tools that are commonly used for long-term ECG monitoring in CS patients [
11]. The accuracy of mobile cardiac outpatient telemetry (MCOT) in the detection of AF after cryptogenic stroke is currently unclear. Promising non-invasive tools such as novel mobile-health (mHealth) options for long-term ECG monitoring are arising, but their reliability and accuracy in the setting of CS have to be proven. Devices with the highest proven yield in detecting AF are implantable cardiac monitors (ICMs) and implantable loop recorders (ILRs). This is true especially in patients with CS, since ICMs prolong substantially the duration of cardiac monitoring (≥5 years) and use remote monitoring [
12]. Compared to conventional follow-up with scheduled ECG monitoring, both ILRs and MCOT have by far the highest rates of AF detection [
8,
11,
13]. Due to the relatively costly technology, the accuracy of ICMs should be improved for further implementation of this technology in ischemic-stroke patients. The use of artificial intelligence (AI) or other arising techniques may improve the detection algorithms of ICMs suffering from false-positive detection rates [
14].
In accordance with the 2021 American Heart Association/American Stroke Association guidelines for the management of acute ischemic stroke, the best duration of extended ECG monitoring after acute ischemic stroke is still uncertain [
15]. Existing systematic-review papers have their main focus on the assessment of the efficacy of ILRs in different settings [
10,
16], with a relative lack of literature investigating the use of MCOT after CS or comparing face to face the efficacy of ILRs with MCOT. Furthermore, the need for an invasive procedure when implanting ILRs and the resulting extended follow-up is not accepted by some patients [
17]. Although health-technology assessments have proven their efficacy, ILRs are still expensive and are considered cost effective if continuously used over a three-year period [
18]. Recently, promising data regarding the efficacy of MCOT have been shown in some individual studies. These data suggest that MCOT may replace or could be used in combination with ILRs [
10,
13].
2. Technologies to Detect and Monitor Atrial Fibrillation
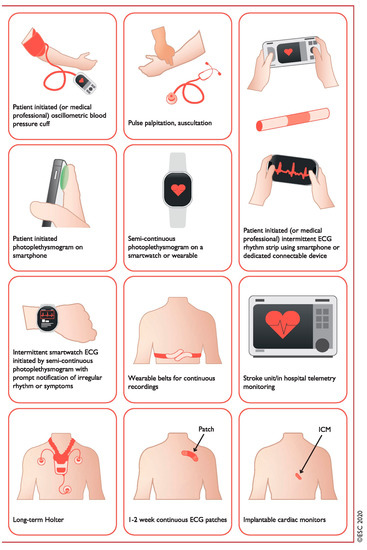
An overview of current technologies is outlined in Figure 1 and Table 1.
Figure 1. Systems used for AF screening. Pulse palpation, automated BP monitors, single-lead ECG devices, PPG devices, and other sensors (using seismocardiography, accelerometers, gyroscopes, etc.) used in applications for smartphones, wristbands, and watches. Intermittent smartwatch detection of AF is possible through PPG or ECG recordings. Smartwatches and other wearables can passively measure pulse rate from the wrist using an optical sensor for PPG and alerting the consumer of a pulse irregularity (based on a specific algorithm for AF detection analyzing pulse irregularity and variability). AF = atrial fibrillation; BP = blood pressure; ECG = electrocardiogram; PPG = photoplethysmography. Reprinted with permission from Ref. [
19]. 2021, Gerhard Hindricks.
2.1. Handheld Devices
Handheld devices are electronic devices that are small enough to be held in the palm of the user. These devices are portable and designed to be activated by touching and are capable of detecting, analyzing, and transmitting bio-signals. Currently, three technologies are available to detect and to monitor AF: photoplethysmography (PPG)-, electrocardiography (ECG)-, and mechanocardiography (MCG)-based devices [
20]. These include mainly FibriCheck [
21], CardiioRhythm [
20], Preventicus [
22], PULSE-SMART [
23], and Kardia mobile by AliveCor [
24], and many others are currently being introduced on the market.
2.2. Wearable Devices
Wearable devices are electronic devices that are worn on the body and are designed to be lightweight so they can be integrated into clothing or worn like an accessory. Wearables are characterized by their ability to collect data about the user, such as heart rate, ECG, activity, and sleep patterns. They are particularly popular among people who want to monitor their physical status with a wide range of PPG-based devices. Wearables can be designed as rings, armbands, wristwatches/bands, armbands, rings, and earlobe sensors. ECG-based devices can be designed as patches, chest belts, and wireless recorders. Finally, pulse-variability-based devices are devices such as sphygmomanometers. Due to the huge amount and continuous development and presentation of new devices, only the method is listed with names of current known products:
Photoplethysmography-based wearables: These include Apple Watch, Samsung Galaxy Watch, Fitbit, Empatica E4, and CardiacSense (all cleared by CE and the FDA). Storage of PPG recordings and access for patients is managed by secure cloud solutions. Currently, the following devices provide these solutions: Apple Watch, Samsung Galaxy Watch, Fitbit, CardiacSense, Samsung Simband, Empatica E4, Gear Fit 2, Wavelet Health, Amazfit, Honor Band 4, Huawei Watch GT, and Honor Watch.
Electrocardiography-based wearables: ZioXT (FDA approved), RhythmPad, Firstbeat Bodyguard 2 (CE approved), and Medi-Trace 200 (validated in clinical studies, FDA and CE approval). Usually, patches use a single-lead or a three-lead ECG recording that is placed on the patients’ chest. In contrast, RhythmPad consists of three sensors placed around both arms and the right leg to record a six-lead ECG. The monitoring duration varies between 10 s and two weeks. TWH (Nuubo) is a textile Holter monitor that can be worn for 90 days.
Pulse-variability-based wearables: These include Microlife BP and OMRON (validated in clinical studies, FDA and CE approval). Storage of PPG recordings and access for patients is managed by secure cloud solutions.
2.3. Implantable Loop Recorders
ILRs are small devices that are implanted under the skin in the chest area to continuously record ECGs. They can be triggered manually by the patient by an external handheld device or a smartphone. Due to the continuous-monitoring capability, activation is carried out automatically by software routines. ILRs have a broad spectrum of other established indications for use [
25]. Wireless communication is possible between the clinician programmer, the ILR, the smartphone, or other computing devices. Via different applications, patients receive information about the heart rhythm, possible rhythm disturbances, and when they should get in contact with the treating doctor. Currently, ILRs are available from four main manufactures: Reveal (Medtronic), BioMonitor (Biotronik), Lux (Boston Scientific), and Confirm (Abbott).
2.4. Mobile Platforms and Support Systems
There is widespread use of mobile devices (smartphones, watches, and tablets), and users spend time on mobile applications most of all. In 2017, 318,000 mobile applications were available worldwide, including more than 500 dedicated to AF management [
26].
This entry is adapted from the peer-reviewed paper 10.3390/jcdd10070306