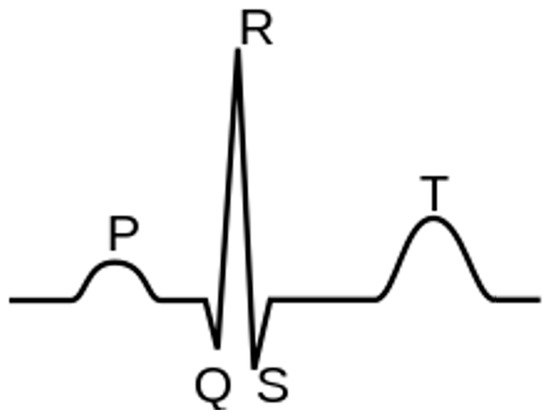
The electrocardiogram (ECG) is among the most commonly utilized clinical tests for patient monitoring and assessment because it is easy to acquire and provides extensive information about patients’ cardiac health [1]. Instead, continuous, real-time, remote monitoring allows for a more rigorous oversight of patients’ conditions, even compared to in-hospital observation. Wearable devices to address monitoring are now a prominent focus of industry [1,2,3,4,5,6], which in turn provides strong motivation for applying artificial intelligence (AI) algorithms to ECG signals for automated disease detection and prediction [7,8,9,10,11].
- ECG
- wearable technology
- machine learning
- deep learning
- m-health
1. Diseases
1.1. Arrhythmias
1.2. Coronary Artery Disease
2. Wearables
3. Algorithms
3.1. Arrhythmia
| Authors (Year) | Specific Application | ECG System (Sampling Frequency) |
AI Algorithm/Method | Database/Dataset | Performance (%) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Acc | Sen | Spe | AUC | F1 | |||||
| Jeon et al. (2020) [39] | General arrhythmias | 2-lead ECG patch [Samsung S-Patch 2] (256 Hz) |
Recurrent Neural Networks | MIT-BIH Arrhythmia Wearable device: S-Patch 2 |
99.80 | - | - | - | - |
| Plawiak et al. (2020) [51] | General arrhythmias | - | Deep Genetic Ensemble of Classifiers | MIT-BIH Arrhythmia | 99.37 | 94.62 | 99.66 | - | - |
| Panganiban et al. (2021) [31] | General arrhythmias | 2-lead ECG [HealthyPiV3 biosensors] (n.s.) |
CNN | MIT-BIH Atrial Fibrillation, PAF Prediction Challenge, PTB Diagnostic ECG, Challenge 2015 Training Set, Fantasia, and PAF Prediction Challenge. ECG signals collected for this study | 98.73 | 96.83 | 99.21 | - | 96.83 |
| Alqudah et al. (2021) [72] | General arrhythmias | - | CNN | IEEE DataPort MIT-BIH Arrhythmia |
99.13 | 99.31 | 99.81 | - | - |
| Yildirim et al. (2018) [52] | General arrhythmias | - | CNN | MIT-BIH Arrhythmia | 95.20 | 93.52 | 99.61 | - | 92.45 |
| Bazi et al. (2020) [40] | General arrhythmias | Wireless 3-lead ECG sensor [Shimmer Sensing (100, 200 Hz) |
SVM | 12-lead Tech-Patient CARDIO ECG simulator Wearable device: Shimmer Sensing MIT-BIH Arrhythmia |
95.10 | 95.80 | - | - | - |
| Lee et al. (2022) [44] | General arrhythmias | - | CNN | ECG from patients at the Korea University Anam Hospital in Seoul, Korea | 97.90 | 98.30 | 97.60 | 99.70 | 97.70 |
| Itzhak et al. (2022) [46] | General arrhythmias | - | Random Forest | Annotated Holter ECG database acquired at the University of Virginia Heart Station | 93.30 | 91.30 | 81.30 | 95.30 | 90.60 |
| Li et al. (2018) [61] | General arrhythmias | - | Generic CNN and Tuned Dedicated CNN | MIT-BIH Arrhythmia | 96.89 | - | - | - | - |
| Ran et al. (2022) [66] | General arrhythmias | 12-lead ECG prototype (500Hz) |
Deep CNN | 12-lead ECG recordings from three centers of Tongji Hospital | - | 89.10 | 99.70 | 94.40 | 91.30 |
| Ribeiro et al. (2022) [65] | General arrhythmias | - | CNN | MIT-BIH Arrhythmia | 99.60 | 98.50 | 99.80 | - | 98.80 |
| Hua et al. (2018) [50] | General arrhythmias | - | SVM | MIT-BIH Arrhythmia | 98.58 | 97.70 | 99.62 | - | - |
| Karthiga et al. (2021) [53] | General arrhythmias | - | CNN | MIT-BIH Arrhythmia | 91.92 | 90.21 | 95.19 | - | 90.11 |
| Zhang et al. (2022) [54] | General arrhythmias | - | CNN | MIT-BIH Arrhythmia | 98.74 | 98.11 | 99.05 | - | - |
| Lee et al. (2021) [73] | General arrhythmias | - | Beat-Interval-Texture CNN | 2017 PhysioNet/Computing in Cardiology Challenge | - | 80.73 | - | - | 81.75 |
| Smisek et al. (2018) [48] | General arrhythmias | - | SVMs Decision Tree | 2017 PhysioNet/Computing in Cardiology Challenge |
- | - | - | - | 81.00 |
| Shin et al. (2022) [58] | General arrhythmias | - | CNN-Bidirectional Long Short-Term Memory | MIT-BIH Arrhythmia | 91.70 | 92.00 | 91.00 | 99.40 | 92.00 |
| Alqudah et al. (2021) [75] | General arrhythmias | - | CNN | MIT-BIH Arrhythmia | 93.80 | 95.20 | 97.40 | - | 93.60 |
| Huang, et al. (2021) [57] | General arrhythmias | - | CNN-LSTM | MIT-BIH Arrhythmia | 98.93 | 96.46 | 99.33 | - | - |
| Tang et al. (2019) [49] | General arrhythmias | - | SVM | MIT-BIH Arrhythmia | 98.90 | 92.80 | 99.40 | - | 92.00 |
| Sakib et al. (2021) [64] | General arrhythmias | - | Deep-Learning-based Lightweight Arrhythmia Classification (CNN) | MIT-BIH Supraventricular Arrhythmia MIT-BIH Arrhythmia St Petersburg INCART 12-lead Arrhythmia Sudden Cardiac Death Holter |
96.67 | - | - | 97.96 | - |
| Shao et al. (2020) [13] | AF | Custom 1-lead ECG patch (250 Hz) |
Decision Tree Ensemble | 2017 PhysioNet/Computing in Cardiology Challenge MIT-BIH Atrial Fibrillation Simulated ECG signals from generator FLUKE MPS450 |
99.62 | 99.61 | 99.64 | - | 92.00 |
| Chen et al. (2020) [30] | AF | PPG & 1-lead ECG [Amazfit Health Band 1S] (250 Hz) |
CNN | PPG and single-channel ECG data | 94.76 | 87.33 | 99.20 | - | - |
| Cai et al. (2020) [15] | AF | 12-lead ECG (500 Hz) |
Deep Densely connected Neural Network | 12-lead ECG 10s recordings collected from multiple hospitals and wearable ECG devices (3 different data sources) | 99.35 | 99.19 | 99.44 | - | - |
| Cheng et al. (2020) [70] | AF | - | Deep Learning Neural Networks | MIT-BIH Atrial Fibrillation | 97.52 | 97.59 | 97.40 | - | 98.02 |
| Fan et al. (2018) [62] | AF | - | Multi-Scale CNN | 2017 PhysioNet/Computing in Cardiology Challenge | 98.13 | 93.77 | 98.77 | - | - |
| Ramesh et al. (2021) [55] | AF | - | CNN | Train: MIT-BIH Normal Sinus Rhythm, MIT-BIH Atrial Fibrillation, MIT-BIH Arrhythmia Test: UMass PPG, acquired from wrist-worn wearable devices |
95.50 | 94.50 | 96.00 | 95.30 | 93.40 |
| Ma et al. (2020) [41] | AF | SmartVest system (400 Hz) |
SVM extended with CNN predictions | Train: MIT-BIH Atrial Fibrillation Test: PhysioNet/Computing in Cardiology Challenge 2017, China Physiological Signal Challenge (CPSC) 2018, 24-h ECG recording (12 h before and 12 h after the radio frequency ablation surgery) collected from an AF patient with the wearable device |
99.08 | 98.67 | 99.50 | - | - |
| Lown et al. (2020) [32] | AF | 1. 12-lead ECG (n.s.) 2. HR monitor [Polar H7 (PH7) HR] (n.s.) |
SVM | MIT-BIH Atrial Fibrillation MIT-BIH Arrhythmia |
- | 100.0 | 97.60 | - | - |
| Zhang et al. (2021) [63] | AF | - | Global Hybrid Multi-Scale Convolutional Neural Network | China Physiological Signal Challenge 2018 (12-lead ECG) 2017 PhysioNet/Computing in Cardiology Challenge (single-lead ECG) |
99.84 | 99.65 | 99.98 | - | 99.54 |
| Zhang et al. (2020) [71] | AF | - | CNN | MIT-BIH Atrial Fibrillation | 96.23 | 95.92 | 96.55 | - | 96.25 |
| Chen et al. (2022) [56] | AF | - | Feedforward Neural Network | 2017 PhysioNet/Computing in Cardiology Challenge MIT-BIH Arrhythmia |
84.00 | 84.26 | 93.23 | 89.40 | - |
| Mei et al. (2018) [47] | AF | - | Baggin Trees | 2017 PhysioNet/Computing in Cardiology Challenge |
96.60 | 83.20 | 98.60 | - | - |
| Wu et al. (2020) [45] | AF | - | Extreme Gradient Boosting | 2017 PhysioNet/Computing in Cardiology Challenge MIT-BIH Atrial Fibrillation MIT-BIH Normal Sinus Rhythm MIT-BIH Arrhythmia |
95.47 | 94.59 | 96.40 | - | 95.56 |
| Bashar et al. (2021) [23] | AF, PAC and PVC | - | SVM | Medical Information Mart for Intensive Care (MIMIC) III | 97.45 | 98.99 | 95.18 | - | - |
| Yu et al. (2021) [18] | PVCs | - | Deep Metric Learning K-Nearest Neighbors | MIT-BIH Arrhythmia | 99.70 | 97.45 | 99.87 | - | - |
| Wang (2021) [24] | PVCs | - | CNN with improved Gated Recurrent Unit network | MIT-BIH Arrhythmia China Physiological Signal Challenge 2018 |
98.30 | 98.40 | 98.20 | - | - |
| Meng et al. (2022) [17] | PVC, SPB | - | Lightweight Fussing Transformer with LightConv Attention | The 3rd China Physiological Signal Challenge 2020 | 99.32 | 92.44 | - | - | 93.63 |
| Khan et al. (2020) [33] | CVDs | - | SVM | Cleveland Heart Disease dataset from the UCI repository | 93.33 | 94.29 | 92.73 | - | - |
| Dami et al. (2021) [76] | CVDs | - | LSTM Deep Belief Network | Four databases: DB1—KAGGLE heart disease dataset|DB2—Shahid Beheshti Hospital Research Center|DB3—Physionet site—Hypertensive patients|DB4—UCI Heart Disease dataset |
88.42 | 85.13 | 85.54 | - | - |
| Khan et al. (2020) [77] | CVDs | Custom 1-lead ECG (n.s.) |
Deep Convolutional Neural Network | UCI machine learning repository, Framingham, and Public Health Dataset | 98.20 | 97.80 | 92.80 | - | 95.00 |
| Tan et al. (2021) [60] | CVDs and COVID-19 | - | CNN-LSTM | MIT-BIH Arrhythmia | 99.29 | 97.77 | 99.53 | - | - |
| Mazumder et al. (2021) [59] | VT and VF | - | CNN-LSTM | MIT-BIH Malignant Ventricular Arrhythmia (VFDB) Creighton University Ventricular Tachycardia (CUDB) |
- | 99.21 | 99.68 | - | - |
3.2. Other Cardiovascular Diseases
| Authors (Year) | Specific Application | ECG System (Sampling Frequency) |
AI Algorithm/Method | Database/Dataset | Performance (%) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Acc | Sen | Spe | AUC | F1 | |||||
| Gibson et al. (2022) [12] | Myocardial Infarction | - | CNN | Latin America Telemedicine Infarct Network (LATIN) | 90.50 | 86.00 | 94.50 | - | - |
| Baloglu et al. (2019) [16] | Myocardial Infarction | - | CNN | PTB ECG: MI on standard 12-lead ECG data | 99.78 | 99.80 | - | - | - |
| Cho et al. (2021) [82] | Heart Failure | 12-lead ECG [Page Writer Cardiograph—Philips] (500 Hz) |
Short-time Fourier transform–CNN combination | ECG from multicenter study | 82.50 | 92.10 | 82.10 | 92.90 | - |
| Wasimuddin et al. (2021) [34] | Myocardial Infarction | Custom 1-lead ECG (n.s.) |
CNN | European ST-T Custom wearable device |
99.26 | 99.27 | 99.27 | - | - |
| Chowdhury et al. (2019) [35] | Myocardial Infarction-Cardiac Arrest | Custom 1-lead ECG (500 Hz) |
Support Vector Machine | MIT-BIH ST Change Normal subjects and an ECG simulator to simulate abnormal ST-elevated MI situations to test the functionality of the complete system in real-time |
97.40 | 99.10 | - | - | 98.70 |
| Shahnawaz et al. (2021) [79] | Myocardial Infarction | - | Artificial Neural Network | PTB (PhysioNet) | 99.10 | 100.00 | 98.10 | - | 99.00 |
| Sopic, et al. (2018) [78] | Myocardial Infarction | - | Random Forest | PTB (PhysioNet) | 80.30 | 87.95 | 79.63 | - | - |
| Martin et al. (2021) [80] | Myocardial Infarction | - | Deep Long Short-Term Memory | PTB-XL and PTB (PhysioNet) | 79.69 | 76.59 | 85.89 | - | 83.42 |
| Cao et al. (2021) [81] | Myocardial Infarction | - | Multi-Channel Lightweight model | PTB (PhysioNet) | 96.65 | 94.30 | 97.72 | 96.71 | - |
This entry is adapted from the peer-reviewed paper 10.3390/s23104805