Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Anant Kumar and Version 2 by Conner Chen.
Oral cancer is a type of head and neck cancer that affects the mouth, tongue, lips, and throat. According to the World Health Organization (WHO), oral cancer is the sixth most common cancer worldwide, with an estimated 300,000 new cases diagnosed each year [1]. The incidence of oral cancer varies widely between different regions of the world, with the highest rates being reported in South and Southeast Asia.
- artificial intelligence
- computer-aided diagnostics
- deep learning
1. Lip Cancer
Lip cancer, also known as squamous cell carcinoma (SCC) of the lip, is a prevalent form of oral malignancy that occurs in the oral–maxillary region. In recent years, there has been a significant increase in the incidence of lip cancer. The authors in [1][28] examined the epidemiological data and risk factors for lip cancer among patients who visited their departments between 2000 and 2010. Out of 540 cases, most patients (84.8%) were men and women over 45 years old. The research revealed that individuals with SCC displayed the typical clinical and epidemiological features identified in prior investigations. These findings can be used to inform the development of methods for health promotion and to raise awareness of the risk factors associated with lip cancer.
1.1. Squamous-Cell-Based Lip Cancer
Squamous-cell-based lip cancer typically presents as well-differentiated lesions that spread later in their growth, with a tendency for metastasis to the submandibular or submental nodes on the opposite side [2][34]. The lower lip (85–95%) is the most affected area, with the upper lip (2–7%) and lip sulcus (1–4%) being the next most frequently affected areas. Lip cancer can resemble an unhealing mouth sore, which may appear red on individuals with light skin or deep brown or grey on individuals with darker complexions [3][35]. Surgery to remove the malignancy is typically the first step in treatment, with more invasive treatments being used for the advanced stages [4][36]. However, these treatments can result in higher morbidity and treatment costs, as well as a significant reduction in the patient’s quality of life. In the later stages of malignancy, the prognosis for oral cancer (OC) deteriorates. According to studies, SCCs make up approximately 95% of non-melanoma skin malignancies and commonly occur on the lower lip [5][33]. In countries with low to moderate incomes, particularly in Southeast and South Asia, oral cancer accounts for two-thirds of cases [6][1]. Basal cell carcinomas, which are less common, tend to impact the upper lip, but typically do not involve lymph node metastases [7][37].
Most cases of OSCC arise from oral potentially malignant disorders (OPMDs) in the oral cavity, which have a 1% chance of transforming into malignant lesions such as erythroleukoplakia, oral lichen planus, and leukoplakia [8][30]. Early detection of OSCC is crucial for a successful treatment plan, improved prognosis, and low rates of death and morbidity [9][38]. The prognosis for advanced stages of oral cancer is poor, with a 50% typical therapeutic efficacy [10][11][7,39]. Histological analysis of tissue samples is the primary method for diagnosing OSCC, but this approach is time-consuming and prone to error [12][13][40,41]. Therefore, it is important to provide pathologists with effective diagnostic tools to aid in the assessment and treatment of OSCC. The use of DL technology for the detection and classification of OSCC has been shown to have great potential for improving treatment efficiency and accuracy [14][42].
1.2. Basal-Cell-Based Lip Cancer
Basal-cell-based lip cancer is characterized by multiple basal cell carcinomas and is also associated with malformations affecting various systems of the body, including the heart, genitourinary system, central nervous system, and skeletal system, as well as specific physical features such as frontal bossing, a large nasal bridge, macrocephaly, and a projecting jaw [15][43]. BCC is a locally invasive tumor that arises from stem cells in the interfollicular epidermis and hair follicles and presents as plaques or nodules on the skin [16][44]. It is important to detect and treat BCCs early, through routine skin cancer screening and sun protection, and to minimize ionizing radiation exposure [17][45]. Orbital invasion, which is associated with less than 5% of periocular BCCs, can occur with advanced BCCs or tumors that continue to grow perineurally [18][46]. Factors associated with a higher likelihood of orbital invasion include a primary tumor near the medial canthal, perineural infiltration, an infiltrative or sclerosing BCC, and multiple recurrences [19][47].
2. Jaw Cancer
Jaw cancer can be caused by the spread of other head and neck cancers or by a rare type of bone cancer called osteosarcoma. Jaw-related bone tumors make up approximately 1% of all head and neck malignancies. The five-year survival rate is typically between 25% and 40%, with mandibular tumors having a better prognosis than maxillary tumors [20][48]. Treatment options include surgery, radiation, and/or chemotherapy, with surgery being the first-line treatment. The risk of recurrence is higher in patients who are diagnosed at later stages, emphasizing the importance of early detection for a positive outcome [21][49].
2.1. Ameloblastic Carcinoma
Ameloblastic carcinoma (AC) is a rare and malignant odontogenic tumor that can be difficult to distinguish from the benign tumor, ameloblastoma. Conversion from ameloblastoma to AC is believed to occur over a long period and may involve multiple stages of carcinogenesis [22][23][50,51]. In recent years, there have been an increasing number of reported cases of AC, but this may be due to improved recognition and diagnosis rather than a true increase in incidence [24][52]. Repeated surgical treatment for odontogenic tumors in resource-limited settings can also lead to secondary cases of AC. It may present as an ulcerated, massive tissue mass with mobile teeth and bone resorption, or as a benign-appearing cystic lesion, making it difficult to diagnose. Dental professionals need to be aware of and recognize the distinguishing characteristics of AC [23][25][26][51,53,54]. It has distinct histological characteristics such as epithelial tumor islands and nests encircled by a layer of stellate basaloid cells during the early stages of malignancy or dedifferentiation, and the signs of malignancy include perineural invasion, cellular focal necrosis, mitoses, pleomorphism, and nuclear hyperchromatism.
The exact mechanism of how AC develops from ameloblastoma is not well understood [27][55]. Younger individuals have a higher survival rate, and primary AC has a better prognosis than secondary AC [28][56]. Adjuvant radiation or chemotherapy may not be more effective than standard postoperative care, but they should be considered for locally advanced or metastatic cases [29][57]. Surgical resection is the most effective treatment for AC, as it has a lower recurrence rate compared to alternative conservative therapies [27][55]. Early diagnosis and aggressive total excision of the tumor are recommended to increase survival rate. FDG PET/CT testing should be carried out during the diagnostic process to detect potential metastatic disease [30][58].
2.2. Primary Intraosseous Carcinoma
PIOC was first described as a core epidermoid cancer of the jaw in 1913 by Loos, and was later referred to as primary intra-alveolar epidermoid cancer by the World Health Organization (WHO) in 1971 [31][59]. In addition to radiation and chemotherapy, broad local excision is the mainstay of treatment for PIOC. In a previous study, at the initial examination, there was no evidence of regional lymph node enlargement in either patient being studied. However, 1 week after the tumors were treated, ipsilateral lymphadenopathy was noticed. The patients were treated with a hemimandibulectomy in these instances, in addition to a radical neck dissection [32][60]. PIOC has distinct histological characteristics, including features that indicate that the tumor originates from the odontogenic epithelium [33][61]. The condition is more common in males and typically affects adults over the age of 50 years; however, it is rare in pediatric and adolescent populations [33][61]. PIOC is sometimes mistaken for an odontogenic cyst since it occasionally displays well-defined boundaries in imaging tests [34][62].
2.3. Sclerosing Odontogenic Carcinoma
The most recent edition of the WHO classification of neck and head malignancies now includes sclerosing odontogenic carcinoma (SOC) which is a rare type of primary intraosseous cancer of the jaw [35][63]. Despite being recognized by the WHO as a unique entity, there have only been a small number of documented cases of this tumor in the literature [36][37][38][39][40][41][64,65,66,67,68,69]. The histomorphology of SOC includes mixed epithelial and mesenchymal components, resembling other odontogenic neoplasms, and presents a diagnostic problem due to the histologic overlap [35][39][41][42][63,67,69,70]. It should be treated as an excluding diagnosis and the treatment for this type of tumor is still challenging due to its rarity and locally invasive nature.
2.4. Clear Cell Odontogenic Carcinoma
Clear cell odontogenic carcinoma (CCOC) originates in the dental lamina, and it was first identified as such in 1985 [43][44][45][71,72,73]. It may be difficult to distinguish from other types of cancer due to its similarities in histology and immunology. It is more commonly found in the mandibular and maxillary bones and more frequently found in women [43][71]. The treatment options include surgical resection, but recurrence and metastasis rates are high [46][47][48][74,75,76]. In a previous study, the metastatic lesion resembled the initial biopsy in appearance, and the diagnosis was made after comparing histological characteristics and immunohistochemistry, and ruling out a second main tumor through clinical assessment and radiology [49][77]. There is little evidence to support the use of chemotherapy as a curative treatment; hence, it should only be used to relieve symptoms. For CCOC, moderate radiotherapy is also beneficial [50][78]. The primary method of treatment is surgical resection with a wide margin. Other options include curettage or surgical excision, laparotomy, post-operative radiation, and chemotherapy [51][79]. The WHO reclassified CCOC as a “malignant carcinoma” of odontogenic origin in 2005 due to its aggressive and locally destructive behavior, which can sometimes metastasize [52][80]. The CCOC’s histopathologic characteristics clearly indicate that this entity has an inductive capacity on the ectomesenchyme as well as a pathogenetic interaction with the ameloblastic epithelium [53][81]. Differential diagnoses include diseases of the odontogenic epithelium, salivary gland disorders, and distant organ metastases. However, recent research has suggested that CCOC may represent a low-grade sarcoma and the bone equivalent of hyalinizing clear cell carcinoma associated with the salivary gland [54][55][82,83].
2.5. Ghost Cell Odontogenic Carcinoma (GCOC)
GCOC, or ghost cell odontogenic carcinoma, is an aggressive type of malignant odontogenic tumor that develops from odontogenic ghost cells [56][84]. It is characterized by ghost cells, malignant cellular characteristics, dental deposits, and areas of invasion and necrosis. It can develop from benign odontogenic neoplasms such as calcifying odontogenic cysts or dentinogenic ghost cell tumors [57][58][85,86]. The diagnosis of GCOC can be difficult due to its similarities with other odontogenic ghost cell lesions, and its nonspecific radiologic and clinical features [58][86]. Its treatment usually involves a combination of aggressive surgical strategies and a multimodal treatment plan.
2.6. Odontogenic Carcinosarcoma
Odontogenic carcinosarcoma (OCS) is a very rare form of jaw cancer that is made up of both epithelial and mesenchymal components [59][60][87,88]. It is similar in structure to ameloblastic fibroma (AF) and can appear as a new lesion or develop from an existing odontogenic lesion [59][61][87,89]. The histological features of OCS include malignant epithelial cells present in hypercellular mesenchymal tissue, and hyperchromatic and pleomorphic cells. OCS can be mistaken for other types of odontogenic tumors and has a high rate of recurrence and metastases [61][89]. The WHO initially classified OCS as a unique entity in 1992, but later withdrew it in the third edition of its classification in 2005 due to difficulty in distinguishing it from other tumors; it was later reinstated as a unique entity in the most recent classification by WHO in 2017 [62][63][90,91]. The pathophysiology, incidence, and outcome of OCS are not well understood, and more research is needed to improve diagnosis and treatment.
2.7. Odontogenic Sarcomas
Ameloblastic fibrosarcoma (AF), also known as odontogenic sarcoma, is a malignant odontogenic tumor. It typically consists of a normal epithelial component and a malignant mesenchymal component [64][92]. A case report has documented a rare instance of AFS that developed from an AF [65][93]. Due to the rarity of metastasis, AFS is considered a low-grade tumor, but it still requires aggressive surgical treatment and postoperative care including chemotherapy and radiation therapy [66][94]. It is important to treat AF promptly to prevent its transformation into AFS, and to monitor patients with both AF and AFS over a prolonged period.
3. Gum, Cheek, Palate, and Other Mouth Cancers
3.1. Gum Cancer
Gum cancer, also known as oral malignancy, affects the gum tissue and makes up 6% of oral cancers. Symptoms include lumps, bleeding, and white or ulcerative lesions on the gums. Adenoid cystic carcinoma is the most common type, making up 15% of cases, followed by mucoepidermoid carcinoma (54%) and low-grade adenocarcinoma (17%) [67][95]. However, attrition from recurrent primary cancers in long-term survivors has hindered further advancements in survival. To improve survival rates, and increased knowledge and methods for early detection, as well as provide education concerning lifestyle-related risk factors are necessary [68][96].
3.2. Buccal Mucosa (Inner Cheek) Cancer
The inner lining of the cheeks, known as the buccal mucosa, is an area that can develop cancer. Buccal mucosal cancer is a rare and dangerous form of oral cancer that makes up a small percentage of patients diagnosed with mouth cancer [69][97]. There is a correlation between local relapse and margin condition for both small and large buccal cancers that are treated only with surgery; however, adjuvant therapy can improve local control in early stage buccal cancers [70][98]. In young people, SCC of the buccal mucosa is preventable and easy to identify, although it often presents in the advanced stages due to socioeconomic factors.
3.3. Floor of the Mouth Cancer
Treatment options for this type of cancer include local resection with radiation therapy and neck incision, local resection with radiation therapy, and composite resection with radiation therapy. However, a study found that none of these treatment options offered a significant survival benefit for patients with FOM cancer [71][99]. Cancers of the FOM can be challenging to treat due to the tendency for metastasis to bilateral cervical lymph nodes and the difficulty in reaching and resecting these tumors [72][73][100,101]. Additionally, FOM cancer is often combined with cancer of the oral tongue, and independent examination of these two types of cancer is preferred for treatment [74][75][76][102,103,104].
3.4. Hard Palate (Roof of the Mouth) Cancer
Hard palate cancer, a type of cancer that affects the bony portion of the roof of the mouth, occurs when cells in the area become uncontrollably proliferated and form tumors or lesions [77][105]. Risk factors for hard palate cancer include the use of tobacco products and excessive alcohol consumption. Early detection of hard palate cancer increases the chances of successful treatment. Surgery by a specialist in neck and head cancer is commonly used to treat the disease, to remove the cancer while preserving the appearance and function of the mouth. The treatment plan is determined by the depth and extent of the cancer and may include a procedure called a maxillectomy. In some cases, radiation therapy alone may be the only option for treatment [78][106]. Figure 1 7 illustrates the various categories of oral cancer grouped according to the origin location within the body.
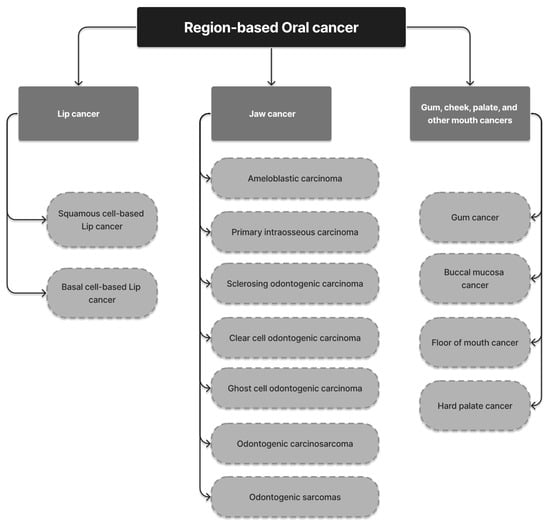
Figure 17.
Classification of OC based on the origin location of lesion.