Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Giovanni Cimmino and Version 3 by Dean Liu.
Pharmacological research has led to the development of a new drug, the bempedoic acid, which further enrich the available therapies. This drug also acts on the biosynthesis of cholesterol but at upstream level than statins. From the biochemical point of view, it has the potential to be considered before the statin with consequent titration of statins to achieve the desirable LDL-C target.
- low-density lipoproteins
- atherosclerosis
- lipid-lowering strategy
1. Introduction
The relationship between low-density lipoprotein cholesterol (LDL-C) levels and cardiovascular events, such as myocardial infarction and stroke, has been confirmed by epidemiological, clinical, and Mendelian studies [1][2][1,2]. Based on this evidence, reducing LDL-C has become a key therapeutic target in the management of cardiovascular diseases (CVD) [3][4][3,4]. Over the past two decades, the concept “The lower the better” has been established indicating that higher is the LDL-C reduction, greater will be the benefits in terms of cardiovascular events [3]. The most recent guidelines from the European Society of Cardiology (ESC) on the management of dyslipidemias have further reduced the therapeutic targets of LDL-C in patients at high and very high cardiovascular risk, suggesting the ambitious value of 70 and 55 mg/dL, respectively [5]. Furthermore, in the patients with a previous acute coronary syndrome (ACS) who undergo a further event, an LDL-C levels < 40 mg/dL is suggested, identifying a class of patients defined at extreme cardiovascular risk [6]. These targets are now achievable owing to the availability of highly effective drugs such as statins, which today represent the most prescribed first-line drugs [7] in addition to a healthy lifestyle. However, in the real world, statin use is associated with large inter-individual variability in terms of response to a fixed statin dose [8] and with the risk of intolerance especially due to reported muscle toxicity [9] which often translates into reduced therapeutic adherence [10]. In case that statin therapy is not tolerated or does not allow to achieve the recommended LDL-C values, the use of other lipid-lowering drugs is necessary [11]. Additional therapeutical options currently available include ezetimibe and the proprotein convertase subtilisin/kexin type 9 (PCSK9i) inhibitors [12]. The higher cost of this latest strategy makes its wide-ranging use difficult, thus, in several country eligible criteria have been defined [13]. For this reason, scientific research in the field of CVD and especially in the management of atherosclerotic diseases, has led to the development of new therapeutic options to lower LDL-C. Among the emerging molecules, bempedoic acid might represent an interesting emerging option [14]. It is a prodrug activated at the hepatic level, which blocks the synthesis of cholesterol upstream of the target enzyme of statins [15]. The efficacy of bempedoic acid in reducing plasma LDL-C levels has been extensively proven in preclinical and clinical studies [16]. Bempedoic acid faces the complex scenario of dyslipidemia with an intriguing pharmacological potential that could make it an interesting alternative in the management of LDL-C-related atherosclerotic diseases.
2. Bempedoic Acid: Biochemical and Pharmacological Features
2.1. Cholesterol Biosynthesis: The Upstream Effect
Bempedoic acid (2,2,14,14-tetramethyl-8-hydroxy-pentadecanoic acid) belongs to a new class of drugs whose primary mechanism of action is direct, competitive inhibition of hepatic adenosine-triphosphate citrate lyase ACLY [17]. It is a cytosolic enzyme involved in the process of cholesterol synthesis that acts upstream of the enzyme 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase (HMGCR), target of statins. It is a prodrug that requires an activation step to exert its inhibitory effect, catalyzed by the enzyme very long chain acyl CoA synthetase-1 (ACSVL1), expressed in the liver but absent in the adipose tissue, intestine, and skeletal muscle [15][18][15,18]. Hence, bempedoic acid is activated only in the liver without muscle involvement [19]. This allows a reduction in the risk of potential adverse events affecting the muscles, such as myalgia and myopathy, which instead might occur during the statins use [20]. The ACSVL1 enzyme inserts an acyl-CoA into the prodrug [15][18][15,18], leading to the formation of the active metabolite, bempedoic acid-CoA, and its reversible conversion to ESP15228, another active metabolite, obtained by oxidation of bempedoic acid [17][21][17,21]. ESP15228 probably contributes less to the overall clinical activity than bempedoic acid [21]. The bempedoic acid-CoA complex competes for the ACLY enzyme with the citrate deriving from the mitochondrial Krebs cycle, preventing its transformation into acyl-CoA and thus blocking the chain of biochemical reactions occurring in the synthesis process of cholesterol [15]. This results in a reduction in the endogenous synthesis of cholesterol in the liver [18]. At the molecular level, the block of cholesterol synthesis activates a specific transcription factor (SREBP2) which in turn promotes the transcription of the gene for the LDL receptor (LDL-R), thus leading to an increased expression of the LDL-R [15]. Clinical data document a reduction in LDL-C levels, but also in non-high-density lipoproteins cholesterol (non HDL-C), apolipoprotein B (ApoB), and total cholesterol (TC) in patients with hypercholesterolemia or mixed dyslipidemia [16]. A schematic view of bempedoic acid function in cholesterol biosynthesis is shown in Figure 1.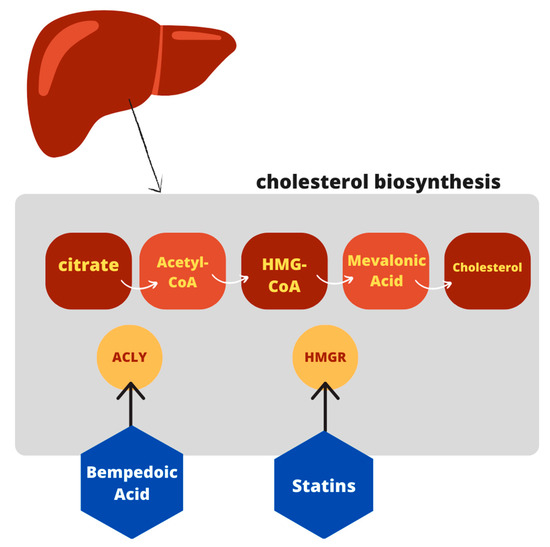
Figure 1.
Schematic view of bempedoic acid function in cholesterol pathway.
2.2. Alternative Biochemical Pathway beyond Cholesterol Synthesis
An additional target of bempedoic acid has also been demonstrated in experimental animals: the drug has shown the ability to activate adenosine monophosphate-activated protein kinase (AMPK) [24], which leads to a reduction in plasma cholesterol concentrations, triglycerides, and inflammatory markers. Moreover, the activation of the kinase could have positive effects on glycemia and insulin resistance [25]. However, it appears to be specific for the AMPK beta 1 isoform, which represents the isoform expressed in the murine liver; vice versa in the human liver where the prevalent form is Beta 2, toward which the drug does not show activity [26]. Thus, this hypothesis need to be corroborated by further evidence in humans. A schematic view is provided in Figure 2.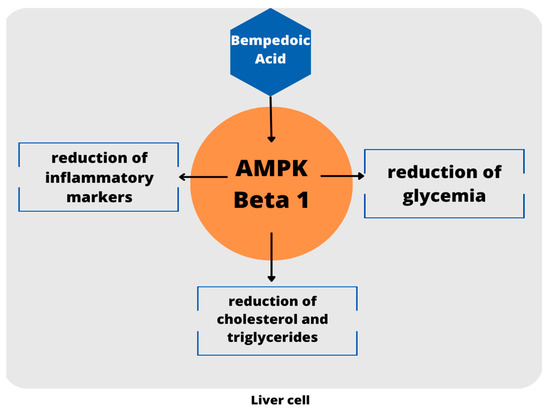
Figure 2.
Schematic view of AMPK activation. To date, these evidence are limited to the mouse model.