Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Bingwei Lu and Version 2 by Dean Liu.
Stroke is one of the leading causes of morbidity and mortality worldwide. A main cause of brain damage by stroke is ischemia-reperfusion (IR) injury due to the increased production of reactive oxygen species (ROS) and energy failure caused by changes in mitochondrial metabolism. Reverse electron transfer (RET) has been implicated in excessive ROS production during IR injury in stroke and new insights into the mechanism of RET gained from various systems in recent studies will help understand stroke pathophysiology and inform therapy.
- mitochondrial complex I
- reverse electron transport (RET)
- reactive oxygen species (ROS)
1. Introduction
Stroke is the second leading cause of morbidity and mortality worldwideafter cancer. In almost 80% of the cases, stroke develops due to a cerebral artery obstruction and/or occlusion [1][2][1,2]. During ischemic stroke, the absence of blood supply deprives the brain cells of the glucose and oxygen nutrients they require, disrupting their cellular homeostasis and ultimately resulting in cell death [2]. Mitochondrial dysfunction and deleterious post-stroke ROS are considered hallmark stroke pathologies [3]. A number of pathophysiological processes, including oxidative stress, excitotoxicity, dysregulated endocrine signaling, inflammation, and apoptosis, are involved in the complex pathophysiological process known as cerebral ischemia/reperfusion injury (CIRI), which frequently causes neuronal injury, cell death, and permanent brain damage [3]. ROS-induced oxidative stress during cerebral ischemia leads to eventual cell death after reperfusion. Mitochondrial ROS (mito-ROS) plays a detrimental role in neuronal death during CIRI at several key stages: inflammation, blood brain barrier (BBB) disruption, mitochondrial respiratory chain complex I-III dysfunction, oedema formation, and apoptosis and autophagy [4][5][6][4,5,6] Currently, thrombolytic and endoscopic thrombectomy are the only therapeutic options, along with post-stroke conservative treatments. The tissue plasminogen activator (tPA) is the only Federal Drug Administration (FDA)-approved therapy for stroke treatment, but due to its various side effects and limited therapeutic window, it only benefits a small portion of stroke patients [7][8][9][10][11][7,8,9,10,11]. Hence, there is an urgent need to develop safer and novel therapeutic options for the treatment of ischemia reperfusion injuries. Due to reduced blood flow and hypoxic conditions, mitochondria are heavily affected by the low O2 and glucose environment. Since the 1960s, the effect of ischemia reperfusion injury on mitochondria has been a research focus and extensive efforts have been dedicated to developing therapeutic strategies to combat reperfusion injury.
2. ROS and Oxidative Stress in Stroke
2.1. ROS Generation during Stroke
Oxidative stress is the result of an imbalance between ROS production and antioxidant defense mechanisms in cells [3]. Because of its high and specific metabolic activity, neurons are particularly vulnerable to oxidative damage. High oxygen consumption, almost entirely oxidative phosphorylation, low energy reserves, high concentrations of peroxidizable lipids, and high levels of iron acting as prooxidants all contribute to this vulnerability [12]. As a result, neuronal cells are extremely vulnerable to metabolic/ischemic damage and the associated oxidative stress [13]. The macro- and micromolecular changes of neuronal cells ends in neurodegeneration in various neurological disorders, e.g., post-stroke dementia, Alzheimer’s disease (AD), vascular dementia, and others [14]. The progression of ischemic stroke pathology is closely connected to dysregulated ROS. The most common ROS are superoxide (O2−), hydrogen peroxide (H2O2), hydroxyl radical (HO−), hypochlorous acid (HOCl−), nitric oxide (NO), and peroxynitrite (ONOO−) that are produced by either intracellular responses (mitochondria) or extracellular inflammation [3][15][3,15]. The intracellular production of ROS is mainly due to the altered metabolic activity of the mitochondrial respiratory chain, whereas extracellularly it is a result of inflammasome activation and the immune response [16][17][16,17]. These reactive molecules can cause lipid peroxidation, protein oxidation, and DNA and RNA damage, resulting in cellular homeostatic failure and tissue damage (Figure 1). Nitric oxide synthetase (NOS) produces NO that is instrumental in the immune response; phagocytes produce large amounts of NO during ischemic brain injury [3][18][3,18]. There are several natural defense mechanisms in the cell to remove ROS or prevent oxidative damage [19]. These include catalase (CAT), heme oxygenase (HO), glutathione reductase, glutathione (GSH), glutathione peroxidase (GSH-Px), superoxide dismutase (SOD), and Vitamins E and C. Microglia and astrocytes are the primary producers of ROS and reactive nitrogen species (RNS), the latter is produced by endothelial NOS (eNOS), inducible NOS (iNOS), or neuronal NOS (nNOS) during ischemic brain injury, which together influence synaptic transmission as well as non-synaptic communication between neurons and glia [20][21][20,21]. ROS and RNS diffuse to the oligodendrocyte myelin sheath during periods of increased neuronal activity, activating the protein kinase C and post-translationally modifying the myelin basic protein, a key structural component of myelin [22][23][22,23].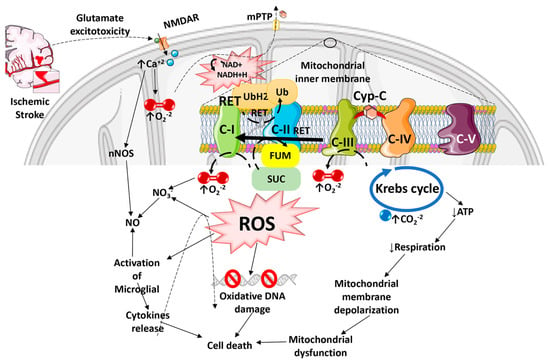
Figure 1. Diagram illustrating how Reactive Oxygen Species especially Reactive Oxygen Species generated by the Reverse Electron Transport process, and the ensuing oxidative stress contributes to mitochondrial dysfunction, cell death, and progressive ischemic stroke pathology. ROS can damage mitochondrial DNA because of the lack of a chromatin-like structure that would protect DNA against ROS insults. ROS can also damage lipids and protein structures in mitochondrial matrix and further exacerbate mitochondrial dysfunction. Mitochondrial ROS released into the cytosol can activate microglia and astrocytes, causing neuroinflammation and death of injured neurons.