Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Mark L Ormiston and Version 2 by Dean Liu.
The natural killer (NK) cells of the immune system identify and remove stressed, infected, or cancerous cells in the body. This anti-tumor functionality has been harnessed through promising cell-based therapies that involve the isolation, expansion, activation, and delivery of NK cells for the treatment of several cancers.
- NK cell dysfunction
- NK cell plasticity
- TGFβ
1. Primary NK Cell Sources
To date, therapies that aim to harness the anti-tumor function of NK cells have involved either the adoptive transfer of ex vivo expanded NK cells, with or without genetic modification [1][2][3][4][15,16,17,18], or the promotion of in vivo NK cell activation through the administration of recombinant proteins, such as interleukin-15 (IL-15) superagonists [5][6][19,20]. For cell-based approaches, several sources have been explored, including primary NK cells from autologous or allogeneic peripheral blood, apheresis products, or umbilical cord blood (UCB) (Figure 1). Primary NK cells comprise only 10% of all lymphocytes in peripheral blood, limiting the number of cells that can be harvested for therapeutic applications and necessitating extensive purification methods, such as the magnetic depletion of undesired cell types [7][21]. NK cells are comparatively enriched in UCB, comprising 15–30% of total lymphocytes, but are immature and may be less cytotoxic compared to other sources [8][9][22,23].
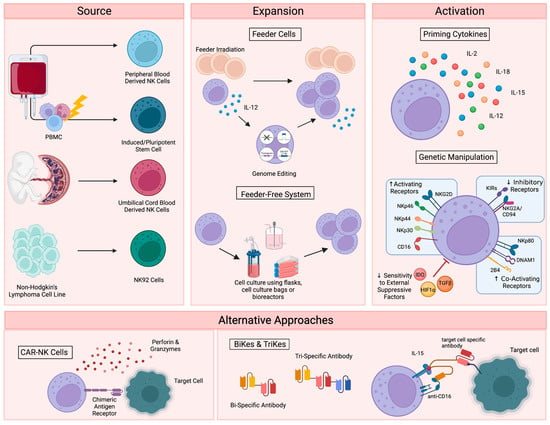
Figure 1. Current NK cell therapies. Schematic showing the current use of NK cell therapies, starting with source, expansion, and activation, then demonstrating the recently developed alternative approaches. Figure created with BioRender.
Alternatively, NK cells can be safely generated from CD34+ hematopoietic progenitors, induced pluripotent stem cells (iPSC), or embryonic stem cells [10][11][24,25]. While iPSC-derived NK cells offer a potentially infinite source of homogenously differentiated NK cells and can be functionally enhanced by genetic modification with relative ease, few groups have successfully created functional NK cells from this cellular source [12][26]. Woan and colleagues reported the use of a clonal iPSC-NK cell line, engineered to express both a high-affinity, non-cleavable version of the CD16a Fc receptor and a membrane-bound IL-15/IL-15 receptor-α fusion protein [13][27]. These cells demonstrated potent anti-tumor activity in vitro, as well as in myeloma and acute myeloid leukemia (AML) xenograft models. Clinical trials are currently underway [14][28]. The use of UCB-derived CD34+ cells as a source for NK cell therapies is also being explored by Deverra Therapeutics, through their non-engineered product DVX201 [15][29].
2. Immortalized NK Cell Lines
Immortalized NK cell lines also offer an alternative to primary NK cells, as they can be cultured indefinitely and are amenable to genetic manipulation. Several NK cell lines have been explored for therapeutic use, including NKL, NKG, NK-YS, YT, YTS, NK-92 cells, and high-affinity NK cells (haNKs). Originally isolated from an individual with non-Hodgkin’s lymphoma, NK-92 cells display high levels of anti-tumor cytotoxicity more consistently and reproducibly than other cell lines [16][17][30,31], are easily expandable to the clinical grade levels required for treatment [18][32], and have been used in recent clinical trials in patients with advanced, treatment-refractory malignancies [19][20][33,34]. HaNKs are NK-92 cells that have been engineered to express a high-affinity CD16 receptor for increased ADCC and endogenous production of IL-2 to maintain cytotoxic function [21][22][35,36]. While advantageous, the clinical application of these cells is not without limitation. NK-92 cells must be irradiated to protect from malignant expansion, potentially limiting their in vivo efficacy and persistence.
3. NK Cell Expansion and Activation
Regardless of their source, NK cells must be expanded to generate sufficient numbers of highly functional cells for therapeutic applications (Figure 1). Clinical scale expansion can be achieved using mitotically inactivated feeder cells, such as peripheral blood mononuclear cells (PBMCs), K562 or Jurkat cells, with or without genetic modification [23][24][25][37,38,39]. Relative to freshly isolated NK cells, expanded populations adopt an activated phenotype with increased expression of activating receptors NKG2D, NKG2C, NKp30, NKp44, DNAM-1 and key effector molecules, such as TRAIL, FasL and granzymes [26][40].
NK cells have also been successfully expanded in feeder-free systems using cell culture flasks, bags, or bioreactors in the presence of high doses of cytokines, such as IL-15 and IL-21 [27][28][41,42], cytokine-conjugated magnetic beads [29][30][43,44], or plasma membrane-derived particles [31][45]. However, these methods typically yield lower cell numbers than what is achieved with feeder cell-based expansion. More recently, advanced systems involving dissolvable polymer-based microspheres [32][46] or streamlined expansion protocols [33][47] have allowed for improved yields and the incorporation of nonviral genome editing into feeder-free expansion systems.
Although growing evidence supports the safety and efficacy of the majority of these expansion techniques [34][48], ex vivo NK cell expansion introduces the potential for senescence and exhaustion [35][49], resulting in the need for expanded NK cells to be activated or “primed” with cytokines like IL-2, IL-12, IL-15, and IL-18 to achieve maximal efficacy on tumors [36][37][50,51]. These cytokines, along with IL-21 and type I interferons, are central to the maturation, activation and survival of NK cells. IL-2 is critical to NK activation, can rejuvenate exhausted NK cells, and restores or preserves their cytotoxic potential in response to various stressors or following exposure to multiple myeloma [38][39][40][52,53,54]. Similarly, the stimulation of NK cells with various combinations of IL-2, IL-12, IL-15 and IL-18 increases the production of critical effector cytokines like IFNγ, IL-8, and TNF-α [41][55], enhances the responsiveness of the cells to the integrin, LFA-1, and improves subsequent receptor stimulation [42][56].
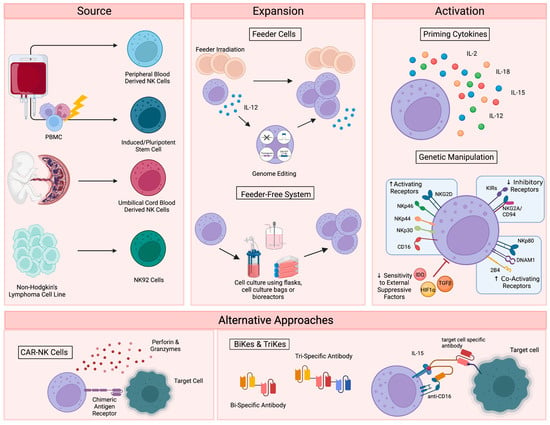
Figure 1. Current NK cell therapies. Schematic showing the current use of NK cell therapies, starting with source, expansion, and activation, then demonstrating the recently developed alternative approaches. Figure created with BioRender.
4. Alternative Approaches for NK Cell Activation
In addition to cytokine-based approaches, genetic manipulations, such as transgenic expression of the Chimeric Antigen Receptor (CAR), have also been explored as a means to enhance NK cell activation for therapeutic applications (Figure 1) [43][57]. CAR is a recombinant protein that can be introduced into cytotoxic lymphocytes to enable tumor antigen recognition and trigger activation [44][58]. CAR expression allows NK cells to specifically target cancer cells through recognition of tumor associated antigens. The generation of CAR-NK cells involves transducing isolated NK cells with CAR-encoding genes and expanding these cells prior to adoptive transfer into the patient [45][59]. Recently, UCB-derived CAR-NK cells were used to treat patients with relapsed or refractory CD19+ cancers, resulting in complete remission in the majority of patients without significant toxic effects [46][60]. Multiple clinical trials are currently underway [47][61], and ongoing studies are investigating the use of CAR-NK cells for the treatment of non-malignant targets, such as HIV-infected cells [48][49][62,63].
Despite these advantages, the complex CAR-NK cell manufacturing process is hindered by inefficient transduction methods [50][64], as well as the poor in vivo persistence shared by many NK cell therapy platforms. The personalized approach required for CAR-NK cells is also extremely expensive, time consuming, and difficult to apply large-scale. These limitations, which are not exclusive to CAR-NK approaches (Table 1), demonstrate a clear need for effective “off-the-shelf” therapies. One such approach is bi- and tri-specific antibodies (BiKEs and TriKEs), which trigger ADCC by binding both CD16 on NK cells and specific tumor antigens, creating a connection-like bridge between these cells and allowing for NK cell activation [51][65]. TriKEs have also been modified to incorporate cytokines like IL-15 to increase in vivo persistence and activation of NK cells [52][66]. In vitro, TriKEs have demonstrated enhanced NK cell activation and killing of both AML cell lines and patient-derived AML blasts [53][67]. A clinical trial in the treatment of high-risk hematological malignancies is currently underway [54][68].
Table 1. Advantages and Limitations to Current NK Cell Therapies.
| Advantages | Limitations | |
|---|---|---|
| Source | ||
| Peripheral Blood NK Cells | Reliable source of CD34 progenitor cells [50][64] | NK cells make up only ~10% of all lymphocytes in peripheral blood |
| High expression of CD16+ | Extensive purification is required to reduce contamination [7][21] | |
| Clinical studies have shown success with these cells after extensive enrichment and purification [55][69] | Isolating large amounts of PB NK cells is difficult [56][57][58][70,71,72] | |
| Cryopreservation has been shown to reduce cytotoxicity [57][59][71,73] | ||
| Umbilical Cord NK Cells | Greater abundance than PB NK cells (15–30% of total lymphocytes) [9][23] | UCB NK cells are immature |
| Fewer contaminating T cells in UCB than PB, reducing the risk of graft-versus-host disease [50][64] | ||
| Associated with good tolerance | May have reduced cytotoxic function [8][22] | |
| Minimal graft-vs-host-disease or toxicity [10][24] | ||
| Induced Pluripotent NK Cell | Easily genetically modified | Limited clinical success to date |
| High availability | Complex differentiation steps | |
| Ability to generate multiple doses from a single healthy donor [17][57][31,71] | Safety concerns regarding toxicity | |
| Commercial NK Cell Lines | Easy to obtain | Must undergo irradiation to prevent malignant expansion, which could limit persistence. |
| Highly cytotoxic | ||
| Easily expandable [18][32] | ||
| NK92 cells are the only cell line that has shown success in pre-clinical studies [17][31] | Efficiency of cells after expansion is variable (4–95%) [60][74] | |
| Expansion | ||
| Feeder Cells | Effective expansion of large numbers of NK cells [61][75]. | Difficult to maintain cytotoxic function after expansion [35][49]. |
| Feeder-Free Expansion | Large amounts of highly active NK cells have been produced | Cytotoxic function after expansion has not been well reported |
| Activation | ||
| IL-2 | Ability to restore NK cell cytotoxicity after exposure to various stressors [40][54]. | Systemic IL-2 leads to significant toxicity |
| Other Activating Cytokines | Less toxic than IL-2 | Thought to provide only minimal clinical benefit |
| Many combination therapies are required to provide a therapeutic benefit | ||
| Genetic Manipulation | Ability to target specific pathways of interest | Relatively newer area of study |
| Ability to avoid toxic effects associated with global therapies | ||
The NK cell engager platform (ANKET) has also been investigated as a means to harness NK cells as next-generation cancer immunotherapies. These NK cell engagers link a monoclonal antibody targeting the activating NK cell receptor NKp46 (or NKp30), an Fc fragment to promote ADCC via CD16, and an antibody targeting a tumor associated antigen, to enable the tumor-localized activation of host NK cells [62][76]. Work with these engagers has shown promise in targeting various cancer cell lines [62][63][64][76,77,78]. Recently, Demaria and colleagues reported a tetraspecific CD20-ANKET, which engages NKp46, CD16a, the beta chain of the IL-2 receptor, and a tumor associated antigen to induce preferential NK cell activation and target cell killing [65][79]. This tetraspecific CD20-ANKET induced the local control of tumors in non-human primates, without significant adverse side effects [65][79].