Obstructive sleep apnea (OSA) and insomnia are the two most common sleep disorders among the general population, and they may often coexist in patients with sleep-disordered breathing (SDB). The higher prevalence of insomnia symptoms in patients with OSA (40–60%) compared to that observed in the general population has thus led researchers to identify a new disorder named comorbid insomnia and OSA (COMISA), whose true burden has been so far largely underestimated. The combined treatment of COMISA patients with positive-airway pressure ventilation (PAP) with cognitive behavioral therapy for insomnia (CBTi) has shown a better patient outcome compared to that obtained with a single treatment. Furthermore, recent evidence has shown that an innovative patient-centered approach taking into consideration patient characteristics, treatment preferences and accessibility to treatment is recommended to optimize clinical management of COMISA patients. However, in this complex mosaic, many other sleep disorders may overlap with COMISA, so there is an urgent need for further research to fully understand the impact of these therapies on outcomes for OSA patients with comorbidity. In light of this need, this re view focuses on the major sleep disorders comorbid with OSA and the recent advances in the management of these insomniac patients are discussed.
1. Introduction
Obstructive sleep apnea (OSA) and insomnia are sleep disorders highly represented in general population and that often coexist interacting to amplify an overall greater illness severity
[1][2][1,2]. The co-occurrence of the two disorders, if not recognized, may complicate OSA treatment reducing compliance with positive airway pressure (PAP) therapy in the presence of insomnia symptoms when not adequately treated together
[3][4][3,4], and, on the other hand, make insomnia more refractory to cognitive behavioral therapy (CBT
i) when there is an association with sleep-disordered breathing
[5][6][5,6]. Recently, researchers have coined the term “COMISA” (Co-Morbid Insomnia and Sleep Apnea) to identify a comorbid condition that can have a worse outcome than the separate conditions and higher management costs
[7][8][7,8]. The two conditions share some common features and may overlap but have different pathophysiological mechanisms and need a different approach
[9]. Unfortunately, this entity has been underestimated for a long time and only recently the interest of the scientific world has focused on recognizing comorbid insomnia and OSA to find an adequate and optimal treatment strategy. Moreover, in this complex framework, many other sleep disorders have been identified that sometimes may overlap with COMISA, making their correct identification, assessment and treatment more difficult.
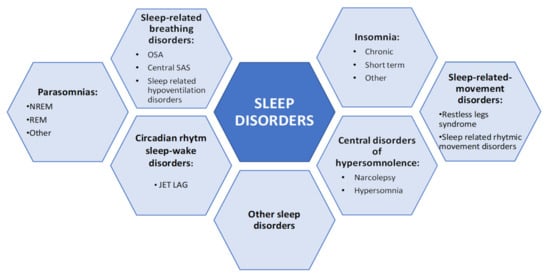
Figure 1 shows the list of diseases that may be diagnosed during sleep according to the International Classification of Sleep Disorders (ICSD) 3rd edition
[10].
Figure 1. Schematic representation of sleep disorders (ICSD-3). NREM: non-rapid eye movement, REM: rapid eye movement, OSA: obstructive sleep apnea, SAS: sleep apnea syndrome.
Given that some of these sleep disorders may occur in the same patients as comorbidities, clinicians should suspect the presence of comorbidities in obstructive sleep apnea (OSA) patients whenever symptoms persist despite adequate treatment. The differential diagnosis is further complicated by the fact that OSA symptoms may often have a different onset from that of the co-occurring sleep disorder, which may also vary over time independently from each other. It is now clear how the main complaint (e.g., OSA or other sleep disorders) needs to be addressed together with the so-called “comorbid” (or secondary) complaint, leading to more specific considerations and an appropriate assessment for a correct management. It is thus important to correctly identify all sleep disorders present in a patient, diagnose them separately and propose an integrated treatment of them to prevent sleep deprivation and preserve sleep integrity and daytime quality of life
[11].
2. Clinical Features and Relationships
2.1. Insomnia and Sleep Apnea
Insomnia and sleep-disordered breathing (SDB) are among the two most frequently diagnosed sleep disorders considering the general population. Because of the high prevalence of co-occurrence of these two conditions, often leading to cumulative morbidity and increased illness severity, a correct and early diagnosis of both disorders is crucial to define their potential interplay and optimize their treatment
[12]. In this regard, the first evidence of co-occurrence was reported by Guilleminault et al. in 1973, who described “a new clinical syndrome, sleep apnea with insomnia”, characterized by repeated episodes of apnea occurring during sleep. The augmented breathing in response to apnea was associated with general arousal and often complete awakening, resulting in loss of sleep
[13]. The ICSD-3 classification describes insomnia symptoms that may occur comorbidly with another sleep disorder, such as sleep apnea or restless leg syndrome
[10] and provides adequate criteria to diagnose comorbid insomnia (
Table 1).
Table 1.
Diagnostic criteria for comorbid Insomnia (ICSD-3).
| A Chronic Insomnia Disorder Diagnosis Would Apply Only When: |
The insomnia symptoms show some independence in their onset or variation over time from the other symptoms of the co-occurring sleep disorder.
When insomnia symptoms persist despite marked symptom improvement of the co-occurring sleep disorder following adequate treatment. A chronic insomnia disorder diagnosis would not apply when effective treatment of the coincident sleep disorder resolves the insomnia symptoms. |
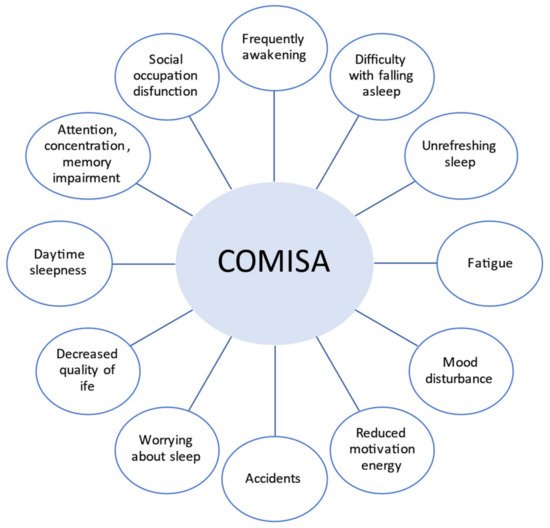
Luyster et al. identified and presented the shared symptoms in both diseases (
Figure 2)
[14].
Figure 2.
Symptoms of obstructive sleep apnea (OSA) and insomnia (COMISA).
According to Ong et al., in individuals with sleep apnea as the primary complaint (e.g., snoring, excessive daytime sleepiness and nocturnal breathing issues), the prevalence of co-occurrence of insomnia was reported as between 6% and 84%. On the other hand, in those patients complaining of the first symptoms of insomnia, the rate of sleep apnea co-occurrence was from 7% to 69%
[15]. In addition to clinical features, comorbidity of insomnia and sleep apnea is associated with increased morbidity and impairment. In particular, concurrent insomnia and OSA increase the risk for other conditions
[12][15][12,15] (Table S1).
One study by Mundt et al., to examine the contributions of OSA and insomnia to chronic pain, found that 80% of participants reported chronic pain, with the most common types of pain being musculoskeletal (28.57%) and headaches (24.76%). A post-hoc comparison showed that individuals with comorbid OSA/insomnia reported an average pain intensity that was 20 points (out of 100) higher than individuals with insomnia or no diagnosis and 28 points higher than those with OSA. They concluded that chronic pain was highly prevalent in this sleep clinic population, with the most severe pain reported by individuals with co-occurring OSA/insomnia with important clinical implications, as both chronic pain and insomnia have been shown to predict poorer adherence to positive airway pressure treatment of OSA
[16]. Another retrospective, cross-sectional study by Krell et al. to determine the prevalence of insomnia complaints in patients undergoing evaluation for suspected OSA showed that of 255 consecutive patients, 54.9% reported a complaint of insomnia. Clinical factors associated with insomnia included female gender, psychiatric diagnoses, chronic pain, the absence of regular alcohol use, restless leg symptoms and reports of nocturnal kicking
[17].
Furthermore, numerous studies have analyzed a higher risk to develop cardiovascular comorbidities (hypertension, cardiovascular diseases, cerebrovascular diseases, diabetes) among patients presenting comorbid OSA plus insomnia or other sleep disorders
[18][19][20][21][22][18,19,20,21,22]. An interesting study by Lang et al. examined the prevalence and profile of previously undiagnosed COMISA symptoms (COMISA) in community-dwelling men showing that men with COMISA have a greater prevalence and severity of depression than men with only one disorder
[23]. Another piece of research hypothesized that, in OSA patients, sleep onset problems mainly due to hyperarousal and sleep maintenance difficulty primarily relate to sleep-disordered breathing. The authors found different insomnia subtypes that related differently to measures of daytime sleepiness suggesting that OSA patients with sleep onset insomnia may be in a state of hyperarousal. This may be conducive to more appropriate treatment decisions in sleep-disordered breathing
[24]. Moreover, some researchers highlighted other conditions related to patients with COMISA, i.e., an increased risk of absenteeism from work
[25] and a reduced quality of life with functional impairment
[26].
For the aforementioned reasons, it is important to identify all comorbid disorders, diagnose them as separated ones and adequately treat each one of them to avoid long-term sequelae
[4].
2.2. Patients Phenotypes
Recent research has focused on symptom scores evoking the existence of distinct clinical phenotypes among OSA patients. Among these phenotypes, most patients present sleep disturbances with typical characteristics of chronic insomniac disorder
[11]. Indeed, subjects with a primary complaint of OSA are more likely to be female
[19][27][28][29][30][19,27,28,29,30], to have dysfunctional beliefs about sleep
[22][31][32][22,31,32], to suffer from restless legs syndrome
[17][33][17,33], and to report less alcohol intake compared to OSA-only patients
[17]. Conversely, patients with a primary complaint of insomnia are more likely to be male
[34][35][34,35], to have a higher body mass index (BMI)
[36][37][36,37], to be older
[38][39][38,39] and to display more daytime and nighttime nocturnal symptoms consistent with OSA compared to patients without OSA
[37][40][37,40]. These findings suggest that if a patient’s chief complaint is different to OSA or insomnia, then different clinical considerations, outcomes and treatment responses would need to be considered. For this reason, secondary complaints need to be completely and fully explored
[15]. In this regard, an interesting longitudinal cohort study by Bjornsdottir et al. investigated the presence of insomnia symptoms present in OSA patients before being treated for sleep apnea
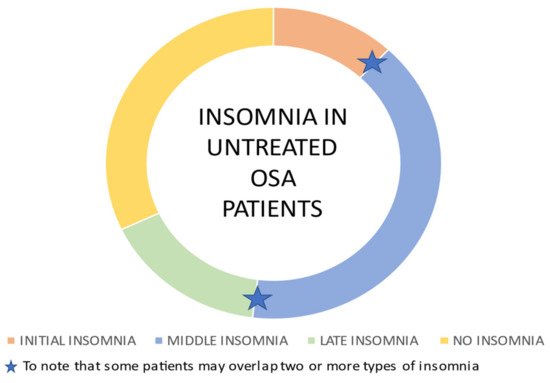
[4]. The authors underline that there are different subtypes of insomnia characterized by difficulties initiating sleep (initial insomnia), difficulties maintaining sleep (middle insomnia) and early morning awakenings (late insomnia) (
Figure 3), and they hypothesized that OSA may be a precipitating factor for each subtype of insomnia; on the other hand, insomnia subtypes may be associated with a different level of continuous positive airway pressure (CPAP) adherence to the treatments in OSA patients in a bidirectional relationship.
Figure 3. Insomnia subtypes in untreated OSA patients. The majority of untreated OSA patients is affected by middle insomnia consistent with OSA fragmentation induced sleep, while one-third of these patients do not experience insomnia. Some patients refer to difficulty in falling asleep (initial insomnia) or early morning awakenings (late insomnia). Some patients may overlap two or more types of insomnia
[4].
The results of the study showed that treatment with positive airway pressure (PAP) after two years significantly reduced symptoms of isolated middle insomnia, while other different mechanisms seem to contribute to symptoms of initial and late insomnia in these patients, likely leading to a negative adherence to PAP. This observation suggests the need for targeted treatment for insomnia (i.e., cognitive behavioral therapy for insomnia before PAP treatment) that may be beneficial for patients with OSA comorbid with insomnia affecting positively adherence to PAP. Another subsequent study by Castillo et al. supporting the overlap features between the two comorbid disorders showed how sleep apnea patients who underwent diagnostic polysomnography displayed a large spectrum of total sleep time misperception values, with one-third of the cohort underestimating their total sleep time by at least 60 min
[41]. Furthermore, in a recent meta-analysis of Zhang et al., the overall prevalence rates of insomnia, any insomnia complaints, difficulty in falling asleep (DFA), difficulty in maintaining sleep (DMS) and early morning awakening (EMA) recorded in OSA patients were 38%, 36%, 18%, 42%, and 21%, respectively. The authors found that, according to the regional classification of the WHO, the rates of DFA, DMS and EMA among OSA patients in the Western Pacific Region were lower than those in the European Region and the Region of the Americas.
They postulated that the regional differences might have been related to sex, age and BMI
[42]. As a general consideration, it is likely to be observed that a deeper investigation of pathogenetic mechanisms is needed and may possibly explain why the coexistence of OSA and insomnia has a negative impact on the two condition’s respective treatment if not promptly recognized.