The cell-free DNA (cfDNA) levels are known to increase in biological fluids in various pathological conditions. However, the data on circulating cfDNA in severe psychiatric disorders, including schizophrenia, bipolar disorder (BD), and depressive disorders (DDs), is contradictory. The meta-analysis showed that the levels of total cfDNA and genomic cfDNA in patients with schizophrenia are significantly higher than in healthy donors (SMD values of 0.61 and 0.6, respectively; p < 0.00001). Data on mitochondrial cfDNA in schizophrenia were scarce. Meta-analysis in BD and DDs found no significant differences in the level of mitochondrial cfDNA. However, further research on mitochondrial and genomic cfDNA levels in psychiatric disorders is needed due to the data heterogeneity.
- cfDNA
- cf-mtDNA
- DAMPs
- schizophrenia
- bipolar disorder
- major depressive disorder
1. Introduction
2. Reports Characteristics
The list of reports included in the meta-analysis and their characteristics are summarized in Table 1. Various analytical methods allow the detection of different types of cfDNA (cf-mtDNA and cf-gDNA) or total cfDNA. Therefore, researchers divided all reports depending on the type of analyzed cfDNA. As a result, the total cfDNA was investigated in 6 studies [20][21][22][23][24][25][37,38,39,40,41,42] and cf-gDNA in three reports in the case of schizophrenia [25][26][27][24,36,42]. There were insufficient data for a meta-analysis of cf-mtDNA in schizophrenia (only two studies) [28][29][34,35]. Cf-mtDNA was analyzed in BD and DDs. The data for other types of cfDNA were insufficient for a meta-analysis in BD and DDs. In particular, only one study on cf-gDNA was found for DDs [27][36]. Accordingly, this meta-analysis analyzed the total cfDNA and cf-gDNA in schizophrenia, and cf-mtDNA was investigated in BD and DDs.| Study | Year | DNA Type | Sample | Extraction Method | Detection Method | Population | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Schizophrenia | |||||||||||
| Ershova et al. [22] | Ershova et al. [39] | 2017 | Total CfDNA | Plasma | Solvent extraction method | FL, PicoGreen dye | SZ 58/HC 30 | ||||
| Jiang et al. [21] | Jiang et al. [38] | 2018 | Total CfDNA | Plasma | TIANamp Micro DNA Kit (spin-column) | FCS | SZ 65/HC 62 | ||||
| Ershova et al. [20] | Ershova et al. [37] | 2019 | Total CfDNA | Plasma | Solvent extraction method | FL, PicoGreen dye | SZ 100/HC 96 | ||||
| Jestkova et al. [23] | Jestkova et al. [40] | 2021 | Total CfDNA | Plasma | Solvent extraction method | FL, PicoGreen dye | SZ 334/HC 95 | ||||
| Ershova et al. [24] | Ershova et al. [41] | 2022 | Total CfDNA | Plasma | Solvent extraction method | FL, PicoGreen dye | SZ 100/HC 60 | ||||
| Lubotzky et al. [25] | Lubotzky et al. [42] | 2022 | Total CfDNA and Cf-gDNA | Plasma | QIAsymphony DSP Circulating DNA Kit (magnetic particles) | FL, bisulfite DNA treatment, PCR amplification followed by NGS | FEP 29/HC 31 | ||||
| Chen et al. [26] | Chen et al. [24] | 2021 | Cf-gDNA | Serum | TianLong DNA Kit (spin-column) | qPCR, target: Alu repeats | SZ 174/HC 100 | ||||
| Qi et al. [27] | Qi et al. [36] | 2020 | Cf-gDNA | Serum | TianLong DNA Kit (spin-column) | qPCR, target: Alu repeats | SZ 164/HC 100 | ||||
| Bipolar Disorder | |||||||||||
| Stertz et al. [30] | Stertz et al. [25] | 2015 | Cf-mtDNA | Serum | QIAmp DNA Mini Kit (spin-column) | qPCR, target: | MT-ATP8 | gene | BD 20/HC 20 | ||
| Kageyama et al. [29] | Kageyama et al. [35] | 2018 | Cf-mtDNA | Plasma | QIAamp DNA Blood Mini Kit (spin-column) | qPCR, target: | MT-ND1 | and | MT-ND4 | genes | BD 28/HC 29 |
| Jeong et al. [31] | Jeong et al. [43] | 2020 | Cf-mtDNA | Serum | QIAmp DNA Mini Kit (spin-column) | qPCR, target: | MT-ND1 | gene | BD 64/HC 41 | ||
| Kageyama et al. [32] | Kageyama et al. [44] | 2022 | Cf-mtDNA | Plasma | QIAamp DNA Blood Mini Kit (spin-column) | qPCR, target: | MT-ND1 | and | MT-ND4 | genes | BD 10/HC 10 |
| Depressive disorders | |||||||||||
| Lindqvist et al. [33] | Lindqvist et al. [45] | 2016 | Cf-mtDNA | Plasma | QIAmp 96 DNA Blood Kit (spin-column) | qPCR, target: | MT-ND2 | gene | Suicide attempters 37/HC 37 | ||
| Kageyama et al. [29] | Kageyama et al. [35] | 2018 | Cf-mtDNA | Plasma | QIAamp DNA Blood Mini Kit (spin-column) | qPCR, target: | MT-ND1 | and | MT-ND4 | genes | MDD 109/HC 29 |
| Lindqvist et al. [34] | Lindqvist et al. [47] | 2018 | Cf-mtDNA | Plasma | QIAmp 96 DNA Blood Kit (spin-column) | qPCR, target: | MT-ND1 | and | MT-ND4 | genes | MDD 50/HC 55 |
| Fernström et al. [35] | Fernström et al. [46] | 2021 | Cf-mtDNA | Plasma | QIAmp DNA Blood Mini Kit (spin-column) | qPCR, target: | MT-ND2 | gene | Current depression 236/HC 49 | ||
| Behnke et al. [36] | Behnke et al. [48] | 2022 | Cf-mtDNA | Serum | QIAamp DNA Micro Kit (spin-column) | qPCR with multiple target | MDD 24/HC 20 | ||||
3. CfDNA Level in Schizophrenia
As stated above, the total cfDNA and cf-gDNA were analyzed in schizophrenia due to insufficient data existing for another type of cfDNA (cf-mtDNA). A meta-analysis of the circulating total cfDNA in schizophrenia pooled data from six studies with a total of 686 patients and 375 healthy controls. It has been shown that the circulating total cfDNA concentration in schizophrenia is significantly higher than in healthy donors (Figure 1a). The SMD for the overall effect was 0.61 (95% CI = [0.40 to 0.82]), with moderate heterogeneity (Chi2 = 11.6, df = 5, p < 0.04; I2 = 57%). The test for the overall effect also confirmed the significance of the differences (Z = 5.6, p < 0.00001). No evidence of publication bias was observed using Egger’s test (p = 0.773) and Begg’s test (p = 0.851). The funnel plot analysis showed signs of asymmetry. The three reports on the left side of the graph were from the same research group using a similar method [20][22][24][37,39,41]. Therefore, the observed asymmetry may indicate a publication bias. One report falling outside the confidence interval was probably related to the measurement methodology (fluorescence correlation spectroscopy) [21][38]. Additionally, there was sample heterogeneity (one of the six reports analyzed FEP patients) [25][42].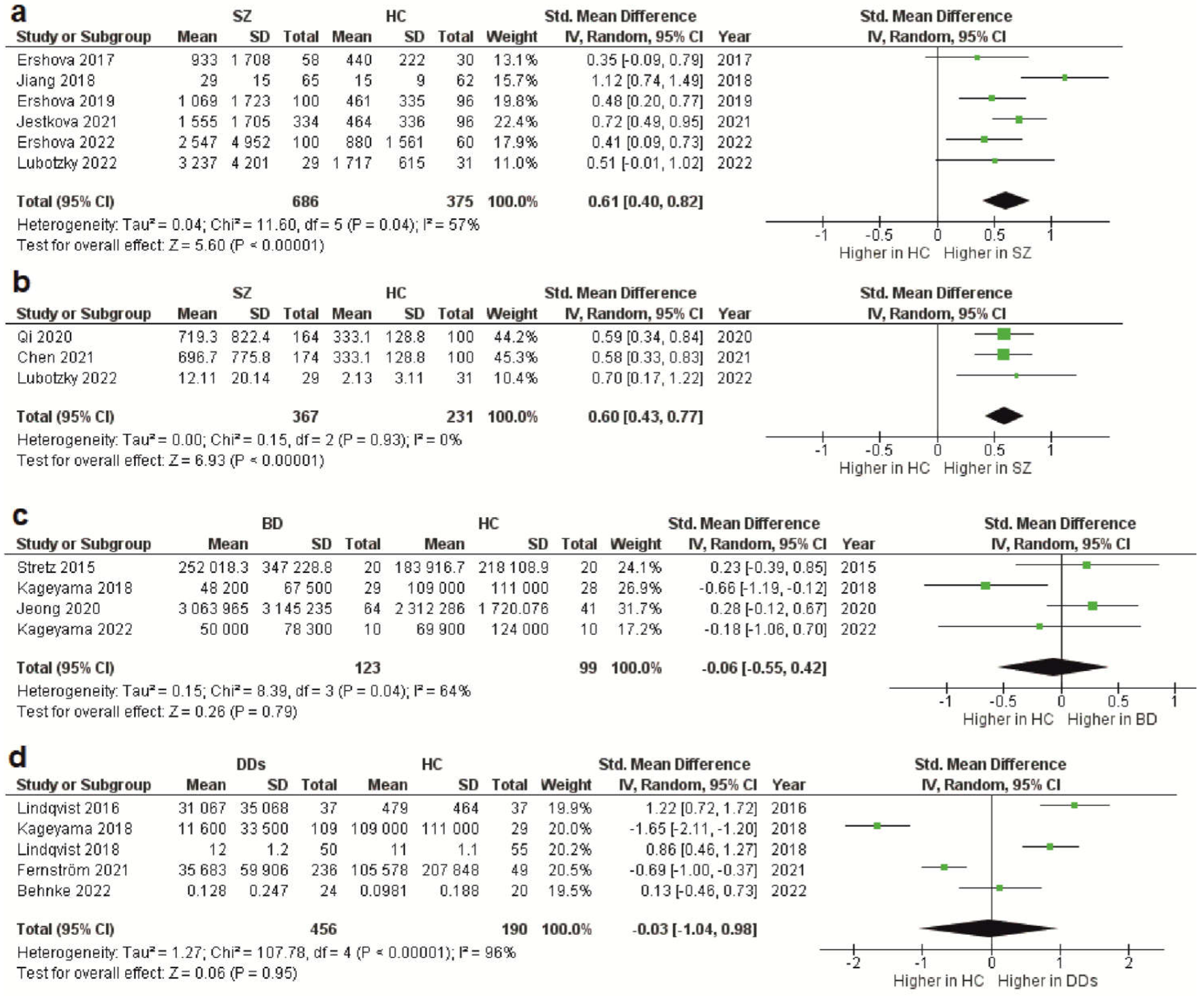 Figure 1. Forest plot showing plasma and serum levels of total cfDNA in patients with schizophrenia (a), cf-gDNA in schizophrenia (b), cf-mtDNA in BD (c), and cf-mtDNA in DDs (d) compared with healthy controls. BD—bipolar disorder; CI—confidence interval; DDs—depressive disorders; SD—standard deviation; SZ—schizophrenia; HC—healthy controls.
The meta-analysis of circulating cf-gDNA in schizophrenia included three studies with a total of 367 patients and 231 healthy individuals. A meta-analysis showed that the cf-gDNA concentration in schizophrenia was significantly higher than in the controls (Figure 1b). The SMD for the overall effect was 0.6 (95% CI = [0.43 to 0.77]). The test for the overall effect also confirmed the significance of the differences (Z = 6.93, p < 0.00001). Interestingly, there was practically no heterogeneity in the report results (Chi2 = 0.15, df = 2, p < 0.93; I2 = 0%). However, while Egger’s test (p = 0.058) and Begg’s test (p = 0.117) showed no evidence of bias, there were some indications of publication bias. In particular, the two reports had the same mean and standard deviation for the cf-gDNA for the group of healthy donors [26][27][24,36]. The funnel plot also confirmed this observation. Therefore, these results must be interpreted with caution. Nevertheless, after removing one of the studies with the same group of healthy donors [26][24], the meta-analysis results remained significant (SMD = 0.61, 95% CI = [0.38 to 0.84] with no heterogeneity (Chi2 = 0.13, df = 1, p < 0.72; I2 = 0%); test for overall effect: Z = 5.23, p < 0.00001). Therefore, further studies are needed to confirm the increased circulating cf-gDNA concentrations in schizophrenia.
Figure 1. Forest plot showing plasma and serum levels of total cfDNA in patients with schizophrenia (a), cf-gDNA in schizophrenia (b), cf-mtDNA in BD (c), and cf-mtDNA in DDs (d) compared with healthy controls. BD—bipolar disorder; CI—confidence interval; DDs—depressive disorders; SD—standard deviation; SZ—schizophrenia; HC—healthy controls.
The meta-analysis of circulating cf-gDNA in schizophrenia included three studies with a total of 367 patients and 231 healthy individuals. A meta-analysis showed that the cf-gDNA concentration in schizophrenia was significantly higher than in the controls (Figure 1b). The SMD for the overall effect was 0.6 (95% CI = [0.43 to 0.77]). The test for the overall effect also confirmed the significance of the differences (Z = 6.93, p < 0.00001). Interestingly, there was practically no heterogeneity in the report results (Chi2 = 0.15, df = 2, p < 0.93; I2 = 0%). However, while Egger’s test (p = 0.058) and Begg’s test (p = 0.117) showed no evidence of bias, there were some indications of publication bias. In particular, the two reports had the same mean and standard deviation for the cf-gDNA for the group of healthy donors [26][27][24,36]. The funnel plot also confirmed this observation. Therefore, these results must be interpreted with caution. Nevertheless, after removing one of the studies with the same group of healthy donors [26][24], the meta-analysis results remained significant (SMD = 0.61, 95% CI = [0.38 to 0.84] with no heterogeneity (Chi2 = 0.13, df = 1, p < 0.72; I2 = 0%); test for overall effect: Z = 5.23, p < 0.00001). Therefore, further studies are needed to confirm the increased circulating cf-gDNA concentrations in schizophrenia.