Obesity has become a major metabolic disorder due to a combination of genetic, nutritional, and environmental factors. Energy balance in the body is sustained by regulating food intake and energy expenditure. Excessive calorie consumption and/or inadequate energy expenditure result in the accumulation of excess body fat, which eventually leads to an obese phenotype. Obesity has long been linked to increased susceptibility and severity of infectious diseases of the respiratory tract. Studies have shown that Body Mass Index (BMI) is linked to worse outcomes and increased severity of respiratory tract infections, such as non-allergic rhinitis and influenza-like illness. During the 2009 H1N1 pandemic and the ongoing SARS-CoV-2 (COVID-19) pandemic, obesity also became a significant risk factor for severe illness and higher mortality.
- COVID-19
- obesity
- innate and adaptive immunity
- inflammation
1. Introduction
2. Relationship between Obesity and Outcome of Infectious Diseases
Obesity has traditionally been associated with increased susceptibility and severity of respiratory tract infectious diseases. Several studies have demonstrated that Body Mass Index (BMI) is associated with increased severity and worse outcome following respiratory tract infections like non-allergic rhinitis and influenza-like-illness. Obesity also emerged as a major risk for severe disease and increased mortality during the 2009 H1N1 pandemic and the ongoing SARS-CoV-2 (COVID-19) pandemic.2.1. Obesity and COVID-19
COVID-19 disease is caused by a novel coronavirus (SARS-CoV-2) that arose in the Chinese province of Wuhan and quickly spread to the entire world to infect and kill millions of people [44]. To this day, the disease is continuously spreading and continues to pose a global threat with devastating consequences. So far, (November 2022) there were 630,832,131 infected cases resulting in 6,584,104 deaths worldwide (WHO data). Several epidemiological studies strongly suggest an association between age and disease severity [45,46][45][46]. Most of the deaths have been reported in patients 65 years of age or older. In addition, people with comorbidities such as diabetes, cardiovascular disease, hypertension, and cancer have significantly higher mortality rates [47,48,49,50][47][48][49][50]. Obesity emerged as an independent risk factor for severe infection, higher ICU hospitalization, and increased death in COVID-19-infected patients. A recent systematic review and meta-analysis of 208 studies with 3,550,997 participants from over 32 countries clearly and convincingly demonstrated that people with obesity have adverse outcomes for COVID-19 disease [51]. The authors showed that being overweight increases the risk of COVID-19-related hospitalization but not mortality, whereas obesity and severe obesity increase the risk of both COVID-19-related hospitalization and death. Obesity was revealed to be a significant risk factor for poor COVID-19 outcomes, and every 5-unit increase in BMI was linked to 28% higher odds of COVID-19-related hospitalizations (OR 1.28, 95% CI 1.00 to 1.47, n = 5) and 10% higher odds of mortality (OR 1.10, 95% CI 1.05 to 1.16, n = 15). Another recent large-scale study involving the systemic review, meta-analysis, and meta-regression analysis of 3,140,413 patients from 167 studies also showed that obesity was significantly associated with increased severity and higher mortality among COVID-19 patients [52]. The authors found that obese individuals are 1.52 times more likely to experience severe outcomes and 1.09 times more likely to die when compared to non-obese individuals with COVID-19 disease. Yet, another meta-analysis involving thirty-eight studies with 902,352 COVID-19 patients found that obesity was a major factor for ICU admission [37]. The negative effect of obesity on COVID-19 infections was consistent in all age groups, in both genders, and in patients from every region of the world. Zhang et al. conducted a systematic review and meta-analysis of obesity and COVID-19 outcomes by quantitative analyses of 22 studies from 7 countries in North America, Europe, and Asia [53]. The authors show that obesity is significantly associated with several adverse comorbidities and outcomes from COVID-19. Obese patients are more likely than non-obese patients to present with severe symptoms (OR 3.03), develop acute respiratory distress syndrome (ARDS; OR 2.89), require hospitalization (OR 1.68), be admitted to the intensive care unit (ICU; OR 1.35), and undergo invasive mechanical ventilation (IMV; OR 1.76) [53]. Many additional research studies from a variety of demographics have established that obese patients are more likely to get severe disease, require hospitalization, and die following COVID-19 infection [34,54,55,56,57,58,59,60,61][34][54][55][56][57][58][59][60][61].2.2. Obesity and H1N1 Infection
The H1N1 virus is a novel strain of the influenza virus that was responsible for the 2009 swine flu pandemic [62,63][62][63]. The virus was first detected in the US before swiftly spreading to other countries. According to World Health Organization (WHO), the virus caused 284,000 deaths worldwide and many of these deaths (~80%) were in people younger than 65 years of age. Several large studies strongly indicated obesity to be a major factor for hospitalization, incentive care treatment and death in H1N1 patients [64,65][64][65]. A systematic review and meta-analysis of six cross-sectional studies with a total of 3059 patients hospitalized for influenza A (H1N1) viral infection revealed that ICU admission rate and mortality rate of severely obese patients (BMI ≥ 40 kg/m2) was significantly higher than patients who were not severely obese. Even those patients with a BMI ≥ 30 kg/m2 were twice as likely to be admitted to ICU or die (OR 2.01) as compared to patients with a BMI < 30 kg/m2, although this did not reach statistical significance [66]. A large study comprising 70,000 laboratory-confirmed hospitalized cases of H1N1 from 19 countries also indicated a strong association between obesity and poorer outcome in H1N1 patients [65]. The study included 70,000 patients of which 9700 were admitted to ICU resulting in the death of 2500 patients. Several other studies demonstrated that obesity was a major risk factor for hospitalization and due to 2009 H1N1 disease [36,67,68,69][36][67][68][69].2.3. Obesity and Other Viral Respiratory Infections
After the H1N1 pandemic, scientists began to explore if obesity was associated with increased severity and worse outcomes following viral respiratory infections. Using a series of Canada’s cross-sectional population-based health surveys Kwong et al. examined the outcomes of patients following influenza infection [70]. The retrospective analysis of twelve influenza seasons clearly showed that obesity was associated with a greater risk for hospitalization during the seasonal influenza periods. The impact of obesity on the risk and outcome of influenza has been reviewed in detail earlier [71]. The research summarizes the epidemiologic effects of obesity on hospital admissions, intensive care unit (ICU) admissions, illness severity, critical infection outcomes, and death related to influenza A/pdmH1N1 infection. After reviewing various cohort studies, the authors found that when compared to normal-weight people, seasonal influenza infections put morbidly obese people at a greater risk of hospitalization and a lengthier hospital stay. Numerous other epidemiological studies have demonstrated a link between obesity and a higher frequency of respiratory tract infections (RTIs), characterized by increased disease severity and higher risk of death [72,73,74][72][73][74].3. Mechanism Linking Obesity to Increased Vulnerability to Infections
It is unclear what specific mechanism(s) makes obese subjects more vulnerable to infectious diseases as compared to people with BMI < 25. [28]. However, obesity-related changes to the host immune system are thought to play a significant role [38,39,43][38][39][43]. Obesity alters both innate and adaptive immune responses and as a result, the immunological response to infectious pathogens is weakened, resulting in worse outcomes post-infection. Obesity-induced systemic inflammation and impaired immune function are illustrated in Figure 1.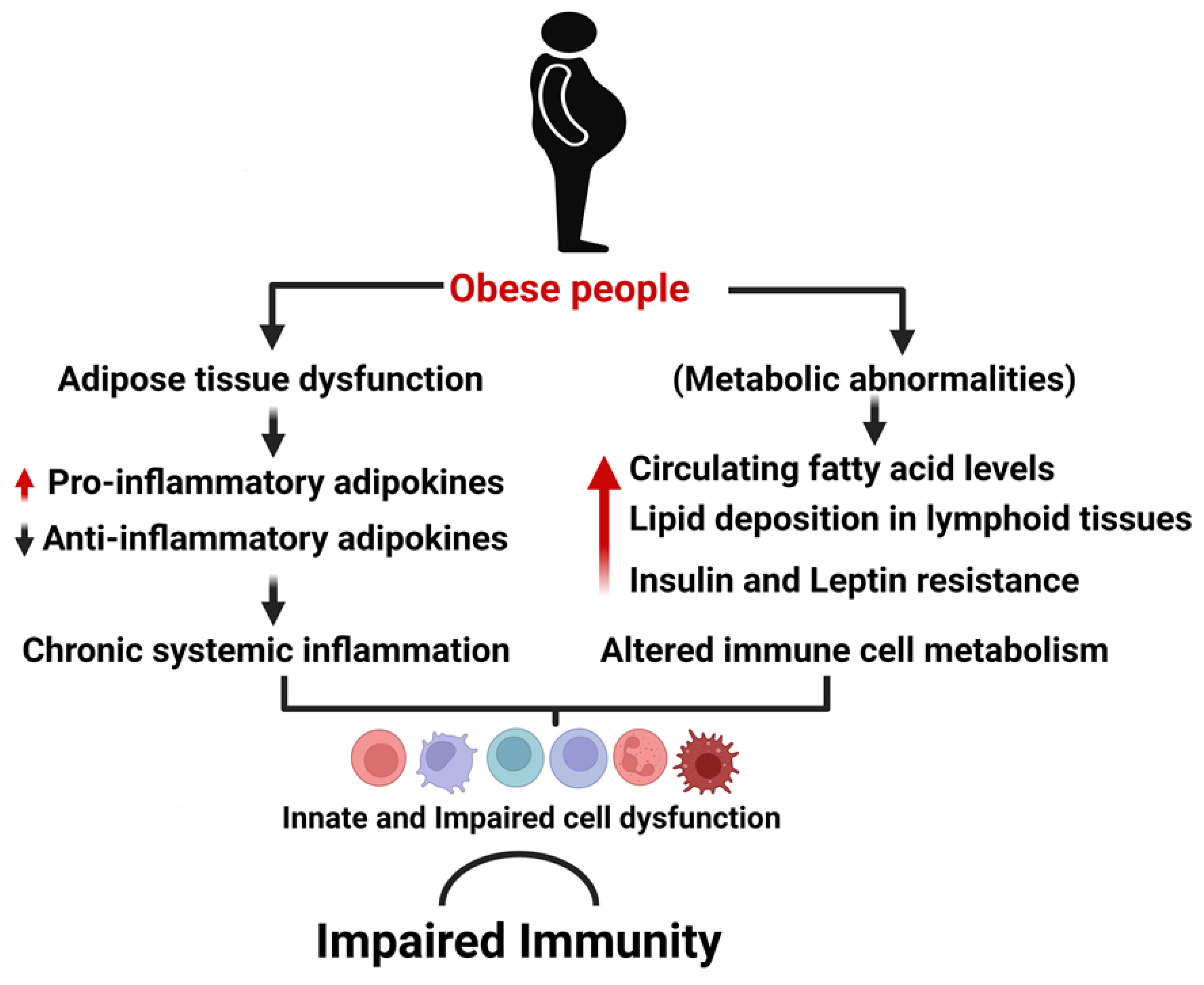
3.1. Obesity Associated Chronic Inflammation
Adipose tissue is a form of loose connective tissue that functions to store fat. While adipose tissue may be found all throughout the body, it is most commonly seen beneath the skin. Adipose tissue can also be seen between muscles and surrounding internal organs, especially those in the abdomen. Adipocytes are the principal constituents of adipose tissue, but it also contains other cell types such as pre-adipocytes, fibroblasts, vascular endothelial cells, and immune cells such as adipose tissue macrophages. Adipose tissue is an important endocrine organ that secretes a variety of factors (including adipokines, chemokines, and cytokines) that have a significant influence on immunological function and metabolism. [48,75][48][75]. Normal lean adipose tissue contains a diverse array of immune cells that maintain a balance between pro-inflammatory and anti-inflammatory responses. Along with their function in removing apoptotic adipocytes, these immune cells have also been connected to angiogenesis, adipogenesis, and the retention of insulin sensitivity in lean individuals. Obesity, on the other hand, affects the function and architecture of adipose tissue, with enlarged adipocytes becoming apoptotic and attracting macrophages and other immune cells to generate inflammatory adipose tissue [76,77,78,79,80][76][77][78][79][80]. Immune cells in healthy white adipose tissue are mostly regulatory and immunosuppressive in nature. Among them are Adipose tissue macrophages (ATMs), regulatory T cells (Tregs), T helper (Th) type 2 cells, and eosinophils. Hypertrophic adipocytes, on the other hand, are more prone to activating endoplasmic reticulum and mitochondrial stress responses, as well as causing shear mechanical stress on the extracellular environment. These elements, when combined, induce the establishment of a chronic, pro-inflammatory state inside the adipose tissue. Compared to healthy adipose tissue, where macrophages make up around 5–10% of the cells, hypertrophic obese adipose tissue in mice and humans can include up to 50% of the total cell types. Hypertrophic adipocytes and macrophages both enhance the release of Tumor necrosis factor (TNF-α), interleukin-6 (IL-6), and monocyte chemoattractant protein-1 (MCP-1), whilst inflammatory leukocytes within adipose tissue further prolong the dysfunctional condition caused by adipocyte hypertrophy by generating resistin and interleukin-1 (IL-1). This eventually results in both local and chronic systemic inflammation. Elevated chronic systemic inflammation is directly responsible for a diminished acute response to numerous stimuli in immune cells and, as a result, a reduced ability to fight infections [39,41,77,79,81,82,83,84][39][41][77][79][81][82][83][84].3.2. Obesity and Immune System Integrity
Obesity is often associated with ectopic lipid accumulation in non-adipose tissues like the liver, skeletal muscle, and pancreas [85,86][85][86]. Ectopic fat deposition, or the accumulation of extra lipids in metabolic organs including the liver and muscle, is associated with insulin resistance (IR) and related metabolic problems. Insulin resistance and ectopic fat interact in a vicious cycle that increases the risk of developing cardiometabolic diseases. Interestingly, ectopic lipid deposition in tissues other than adipose is not limited to metabolic tissues, and obesity-linked lipid deposition has also been found to occur in the main lymphoid organs (bone marrow and thymus). Several independent studies have shown that obesity also affects primary lymphoid organs (bone marrow and thymus) and adversely impacts their functioning [87,88][87][88]. The integrity of primary lymphoid tissues is critical for appropriate leukocyte formation and maturation. Blood cell lineages are formed from pluripotent hematopoietic stem cells obtained from bone marrow. Lymphoid cells are processed further in the thymus to become mature T-lymphocytes. Mature lymphocytes, such as lymph nodes and the spleen, dwell in secondary lymphoid tissues where they participate in immune surveillance and await pathogen activation. As a result, any change in lymphoid tissue architecture might have a detrimental effect on its functioning, resulting in changes in the distribution of immune cell populations, poorer T cell activity, and decreased immunological defense [39,89,90,91][39][89][90][91]). Ectopic lipid deposition impairs lymphoid tissue integrity and changes the cellular distribution of immune cell populations, resulting in decreased T cell activity and immunological protection against infections. It is well known that lipid buildup in lymphoid organs occurs in the elderly and has a negative impact on immunity. As a result, obesity is thought to accelerate aging of the immune system [91]. The authors used high-fat diet-fed mice (DIO mice) that are widely used to study human obesity and associated metabolic abnormalities. DIO was shown to significantly exacerbate the age-related decline of peripheral lymphocytes containing the T-cell receptor (TCR) excision circle, a marker of freshly produced T cells from the thymus [72].3.3. Insulin and Leptin Resistance Impact Immune System Functioning
Insulin is the primary hormone responsible for regulating glucose, protein, and lipid metabolism in metabolic tissues. Insulin is secreted from pancreatic β-cells and signals via the insulin receptor that is expressed throughout the body. Interestingly, immune cells also express the insulin receptor; however how insulin signaling affects the metabolism of immune cells is not completely understood [92]. Several studies have highlighted the importance of insulin receptor signaling in T-cell functioning during inflammation and acute infection. Helderman et al. were the first to show that stimulation of T cells upregulates the insulin receptor on their surface, providing the first evidence for insulin’s beneficial effects on increasing T cell proliferation and metabolism [93]. In vitro evidence of T cell insulin-responsive glucose uptake regulation and mTOR-dependent Tbet expression was provided by subsequent investigations [94,95][94][95]. Sue Tsai et al. reported that the expression of the insulin receptor is undetectable in T cells under the steady state and therefore loss of the Insulin receptors has little effect on T cell homeostasis in the steady state. However, loss of insulin signaling impaired the inflammatory capacity of both CD4+ and CD8+ T cells under activating circumstances, for example during homeostatic proliferation and viral infections [96]. In particular, the lack of insulin receptor signaling impaired the production of inflammatory cytokines by T cells, effector differentiation, proliferation, and migration/recruitment to target organs. Taken together these results imply that T-cell-specific insulin resistance in obese subjects might play a role in the diminished activation of T-cells during active infections. Other studies have confirmed impaired insulin signaling in lymphocytes of obese subjects and type 2 diabetes patients [89,97][89][97]. Adiponectin is a key hormone secreted that exerts an indirect action by enhancing the insulin sensitivity of cells and by reducing inflammation [98,99][98][99]. Adiponectin is recognized to have an important role in immune cell activity, particularly T-cells. Adiponectin levels are considerably lower in people infected with the COVID-19 and H1N1 viruses [69,100,101,102][69][100][101][102]. Adiponectin deficiency exacerbates insulin resistance and inflammation, decreasing overall immunological response to infection. Indeed, circulating adipokine levels are linked to COVID-19 disease severity, which includes hospitalization, the requirement for oxygen assistance, mechanical ventilation, and additional organ support in the intensive care unit [102]. In addition to insulin, leptin, a hormone released by adipocytes, has a significant impact on both innate and adaptive immunity. Leptin is a crucial regulator of metabolic balance, acting largely through leptin receptors (LEPR), which are abundantly expressed in POMC neurons in the hypothalamus, the brain region responsible for controlling hunger and energy expenditure. LEPRs are expressed in immune system cells, and several studies have shown that leptin regulates various aspects of immune cell development and activity [103,104,105,106][103][104][105][106]. Leptin has been shown to influence both innate and adaptive immune responses by influencing immune cell metabolism, proliferation, and activity [107]. Both leptin-deficient (ob/ob) and LEPR-deficient (db/db) mice have impaired innate and adaptive immune responses to infection. Besides, a missense mutation that causes leptin deficiency leads to immune dysfunction in humans [108]. Obese people have significantly higher circulating leptin levels, but their response to leptin is severely compromised due to leptin resistance [109,110,111][109][110][111]. As a result, leptin resistance would significantly impact the proper development and activity of immune cells in obese people, weakening the host defense against infections [32,107][32][107].3.4. Pulmonary Complications of Obesity
Excess weight significantly alters pulmonary physiology, causing decreased lung volumes, decreased compliance, abnormal ventilation and perfusion relationships, and respiratory muscle inefficiency [112,113,114][112][113][114]. In healthy individuals the diaphragm contracts during respiration pushing the contents of the abdomen downward and forward. The external intercostal muscles contract at the same time pulling the ribs up and forward. This function is compromised in obese people because the extra body fat restricts the ability of the respiratory muscles to contract, lining the chest and filling the abdomen excess thoracic and abdominal fat can impair chest wall movement, airway size, respiratory muscle function, and lung perfusion. The ability to move the chest wall decreases as fat accumulates, resulting in stiffness and decreased lung compliance. Measuring compliance is difficult, but reductions appear to be proportional to increases in BMI [112,113][112][113]. Finally, obesity appears to have a variety of effects on the respiratory system via mechanical, biochemical, and structural changes [115,116,117,118,119][115][116][117][118][119]. These can aggravate or worsen various respiratory conditions including viral infections.References
- Caballero, B. Humans against Obesity: Who Will Win? Adv. Nutr. 2019, 10, S4–S9.
- Withrow, D.; Alter, D.A. The Economic Burden of Obesity Worldwide: A Systematic Review of the Direct Costs of Obesity. Obes. Rev. 2011, 12, 131–141.
- Boutari, C.; Mantzoros, C.S. A 2022 Update on the Epidemiology of Obesity and a Call to Action: As Its Twin COVID-19 Pandemic Appears to Be Receding, the Obesity and Dysmetabolism Pandemic Continues to Rage On. Metabolism 2022, 133, 155217.
- Conway, B.; Rene, A. Obesity as a Disease: No Lightweight Matter. Obes. Rev. 2004, 5, 145–151.
- Smith, K.B.; Smith, M.S. Obesity Statistics. Prim. Care 2016, 43, 121–135.
- da Costa, L.A.; Arora, P.; García-Bailo, B.; Karmali, M.; El-Sohemy, A.; Badawi, A. The Association between Obesity, Cardiometabolic Disease Biomarkers, and Innate Immunity-Related Inflammation in Canadian Adults. Diabetes Metab. Syndr. Obes. 2012, 5, 347–355.
- Ghoorah, K.; Campbell, P.; Kent, A.; Maznyczka, A.; Kunadian, V. Obesity and Cardiovascular Outcomes: A Review. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 77–85.
- Black, P. Obesity and Diabetes: Time to Act. Br. J. Nurs. 2009, 18, 1089.
- Chan, M. Obesity and Diabetes: The Slow-Motion Disaster. Milbank Q. 2017, 95, 11–14.
- Shestakova, M.V.; Shestakova, E.A.; Sklyanik, I.A.; Stafeev, I.S. Obesity and Diabetes—Are They Always Together? Ter. Arkh. 2022, 94, 1131–1135.
- Leitner, D.R.; Frühbeck, G.; Yumuk, V.; Schindler, K.; Micic, D.; Woodward, E.; Toplak, H. Obesity and Type 2 Diabetes: Two Diseases with a Need for Combined Treatment Strategies—EASO Can Lead the Way. Obes. Facts 2017, 10, 483–492.
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The Incidence of Co-Morbidities Related to Obesity and Overweight: A Systematic Review and Meta-Analysis. BMC Public Health 2009, 9, 88.
- Sharma, V.; Coleman, S.; Nixon, J.; Sharples, L.; Hamilton-Shield, J.; Rutter, H.; Bryant, M. A Systematic Review and Meta-analysis Estimating the Population Prevalence of Comorbidities in Children and Adolescents Aged 5 to 18 Years. Obes. Rev. 2019, 20, 1341–1349.
- Sullivan, P.W.; Morrato, E.H.; Ghushchyan, V.; Wyatt, H.R.; Hill, J.O. Obesity, Inactivity, and the Prevalence of Diabetes and Diabetes-Related Cardiovascular Comorbidities in the U.S., 2000–2002. Diabetes Care 2005, 28, 1599–1603.
- He, Q.-X.; Zhao, L.; Tong, J.-S.; Liang, X.-Y.; Li, R.-N.; Zhang, P.; Liang, X.-H. The Impact of Obesity Epidemic on Type 2 Diabetes in Children and Adolescents: A Systematic Review and Meta-Analysis. Prim. Care Diabetes 2022, 16, 736–744.
- Yeh, T.-L.; Chen, H.-H.; Tsai, S.-Y.; Lin, C.-Y.; Liu, S.-J.; Chien, K.-L. The Relationship between Metabolically Healthy Obesity and the Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1228.
- Umer, A.; Kelley, G.A.; Cottrell, L.E.; Giacobbi, P.; Innes, K.E.; Lilly, C.L. Childhood Obesity and Adult Cardiovascular Disease Risk Factors: A Systematic Review with Meta-Analysis. BMC Public Health 2017, 17, 683.
- Fan, J.; Song, Y.; Chen, Y.; Hui, R.; Zhang, W. Combined Effect of Obesity and Cardio-Metabolic Abnormality on the Risk of Cardiovascular Disease: A Meta-Analysis of Prospective Cohort Studies. Int. J. Cardiol. 2013, 168, 4761–4768.
- Wang, Z.J.; Zhou, Y.J.; Galper, B.Z.; Gao, F.; Yeh, R.W.; Mauri, L. Association of Body Mass Index with Mortality and Cardiovascular Events for Patients with Coronary Artery Disease: A Systematic Review and Meta-Analysis. Heart 2015, 101, 1631–1638.
- Olsen, C.M.; Green, A.C.; Whiteman, D.C.; Sadeghi, S.; Kolahdooz, F.; Webb, P.M. Obesity and the Risk of Epithelial Ovarian Cancer: A Systematic Review and Meta-Analysis. Eur. J. Cancer 2007, 43, 690–709.
- Sun, J.-W.; Zhao, L.-G.; Yang, Y.; Ma, X.; Wang, Y.-Y.; Xiang, Y.-B. Obesity and Risk of Bladder Cancer: A Dose-Response Meta-Analysis of 15 Cohort Studies. PLoS ONE 2015, 10, e0119313.
- Li, H.; Boakye, D.; Chen, X.; Hoffmeister, M.; Brenner, H. Association of Body Mass Index With Risk of Early-Onset Colorectal Cancer: Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2021, 116, 2173–2183.
- Raglan, O.; Kalliala, I.; Markozannes, G.; Cividini, S.; Gunter, M.J.; Nautiyal, J.; Gabra, H.; Paraskevaidis, E.; Martin-Hirsch, P.; Tsilidis, K.K.; et al. Risk Factors for Endometrial Cancer: An Umbrella Review of the Literature. Int. J. Cancer 2019, 145, 1719–1730.
- O’Sullivan, D.E.; Sutherland, R.L.; Town, S.; Chow, K.; Fan, J.; Forbes, N.; Heitman, S.J.; Hilsden, R.J.; Brenner, D.R. Risk Factors for Early-Onset Colorectal Cancer: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2022, 20, 1229–1240.e5.
- Sohn, W.; Lee, H.W.; Lee, S.; Lim, J.H.; Lee, M.W.; Park, C.H.; Yoon, S.K. Obesity and the Risk of Primary Liver Cancer: A Systematic Review and Meta-Analysis. Clin. Mol. Hepatol. 2021, 27, 157–174.
- Global BMI Mortality Collaboration; di Angelantonio, E.; Bhupathiraju, S.; Wormser, D.; Gao, P.; Kaptoge, S.; Berrington de Gonzalez, A.; Cairns, B.; Huxley, R.; Jackson, C.; et al. Body-Mass Index and All-Cause Mortality: Individual-Participant-Data Meta-Analysis of 239 Prospective Studies in Four Continents. Lancet 2016, 388, 776–786.
- Huttunen, R.; Syrjänen, J. Obesity and the Risk and Outcome of Infection. Int. J. Obes. 2013, 37, 333–340.
- Mancuso, P. Obesity and Respiratory Infections: Does Excess Adiposity Weigh down Host Defense? Pulm. Pharmacol. Ther. 2013, 26, 412–419.
- Yuan, K.; Chen, H.-L. Obesity and Surgical Site Infections Risk in Orthopedics: A Meta-Analysis. Int. J. Surg. 2013, 11, 383–388.
- de Leeuw, A.J.M.; Oude Luttikhuis, M.A.M.; Wellen, A.C.; Müller, C.; Calkhoven, C.F. Obesity and Its Impact on COVID-19. J. Mol. Med. 2021, 99, 899–915.
- de Siqueira, J.V.V.; Almeida, L.G.; Zica, B.O.; Brum, I.B.; Barceló, A.; de Siqueira Galil, A.G. Impact of Obesity on Hospitalizations and Mortality, Due to COVID-19: A Systematic Review. Obes. Res. Clin. Pract. 2020, 14, 398–403.
- Mohammad, S.; Aziz, R.; al Mahri, S.; Malik, S.S.; Haji, E.; Khan, A.H.; Khatlani, T.S.; Bouchama, A. Obesity and COVID-19: What Makes Obese Host so Vulnerable? Immun. Ageing 2021, 18, 1.
- Yang, J.; Hu, J.; Zhu, C. Obesity Aggravates COVID-19: A Systematic Review and Meta-analysis. J. Med. Virol. 2021, 93, 257–261.
- Földi, M.; Farkas, N.; Kiss, S.; Zádori, N.; Váncsa, S.; Szakó, L.; Dembrovszky, F.; Solymár, M.; Bartalis, E.; Szakács, Z.; et al. Obesity Is a Risk Factor for Developing Critical Condition in COVID-19 Patients: A Systematic Review and Meta-Analysis. Obes. Rev. 2020, 21, e13095.
- Louie, J.K.; Acosta, M.; Samuel, M.C.; Schechter, R.; Vugia, D.J.; Harriman, K.; Matyas, B.T. A Novel Risk Factor for a Novel Virus: Obesity and 2009 Pandemic Influenza A (H1N1). Clin. Infect. Dis. 2011, 52, 301–312.
- Milner, J.J.; Rebeles, J.; Dhungana, S.; Stewart, D.A.; Sumner, S.C.J.; Meyers, M.H.; Mancuso, P.; Beck, M.A. Obesity Increases Mortality and Modulates the Lung Metabolome during Pandemic H1N1 Influenza Virus Infection in Mice. J. Immunol. 2015, 194, 4846–4859.
- Wang, Y.; Hou, H.; Xu, J.; Wang, Y.; Yang, H. The Association between Obesity and ICU Admission among COVID-19 Patients: A Meta-Analysis of Adjusted Risk Estimates. Am. J. Emerg. Med. 2022, 56, 318–320.
- Andersen, C.J.; Murphy, K.E.; Fernandez, M.L. Impact of Obesity and Metabolic Syndrome on Immunity. Adv. Nutr. 2016, 7, 66–75.
- de Heredia, F.P.; Gómez-Martínez, S.; Marcos, A. Obesity, Inflammation and the Immune System. Proc. Nutr. Soc. 2012, 71, 332–338.
- Fernández-Verdejo, R.; Moya-Osorio, J.L.; Fuentes-López, E.; Galgani, J.E. Metabolic Health and Its Association with Lifestyle Habits According to Nutritional Status in Chile: A Cross-Sectional Study from the National Health Survey 2016-2017. PLoS ONE 2020, 15, e0236451.
- Monteiro, R.; Azevedo, I. Chronic Inflammation in Obesity and the Metabolic Syndrome. Mediat. Inflamm. 2010, 2010, 289645.
- Viardot, A.; Lord, R.V.; Samaras, K. The Effects of Weight Loss and Gastric Banding on the Innate and Adaptive Immune System in Type 2 Diabetes and Prediabetes. J. Clin. Endocrinol. Metab. 2010, 95, 2845–2850.
- Vasheghani, M.; Hessami, Z.; Rekabi, M.; Abedini, A.; Qanavati, A. Evaluating Possible Mechanisms Linking Obesity to COVID-19: A Narrative Review. Obes. Surg. 2022, 32, 1689–1700.
- Simón Abadía, C. COVID-19, a Graphic Account. Emergencias 2020, 32, 206–209.
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-González, V.; Fácila, L.; Ariza, A.; Núñez, J.; Cordero, A. The Effect of Age on Mortality in Patients With COVID-19: A Meta-Analysis With 611,583 Subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918.
- O’Driscoll, M.; Ribeiro Dos Santos, G.; Wang, L.; Cummings, D.A.T.; Azman, A.S.; Paireau, J.; Fontanet, A.; Cauchemez, S.; Salje, H. Age-Specific Mortality and Immunity Patterns of SARS-CoV-2. Nature 2021, 590, 140–145.
- Bergman, J.; Ballin, M.; Nordström, A.; Nordström, P. Risk Factors for COVID-19 Diagnosis, Hospitalization, and Subsequent All-Cause Mortality in Sweden: A Nationwide Study. Eur. J. Epidemiol. 2021, 36, 287–298.
- Booth, A.; Magnuson, A.; Fouts, J.; Foster, M.T. Adipose Tissue: An Endocrine Organ Playing a Role in Metabolic Regulation. Horm. Mol. Biol. Clin. Investig. 2016, 26, 25–42.
- Dessie, Z.G.; Zewotir, T. Mortality-Related Risk Factors of COVID-19: A Systematic Review and Meta-Analysis of 42 Studies and 423,117 Patients. BMC Infect. Dis. 2021, 21, 855.
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345.
- Sawadogo, W.; Tsegaye, M.; Gizaw, A.; Adera, T. Overweight and Obesity as Risk Factors for COVID-19-Associated Hospitalisations and Death: Systematic Review and Meta-Analysis. BMJ Nutr. Prev. Health 2022, 5, 10–18.
- Singh, R.; Rathore, S.S.; Khan, H.; Karale, S.; Chawla, Y.; Iqbal, K.; Bhurwal, A.; Tekin, A.; Jain, N.; Mehra, I.; et al. Association of Obesity With COVID-19 Severity and Mortality: An Updated Systemic Review, Meta-Analysis, and Meta-Regression. Front. Endocrinol. 2022, 13, 780872.
- Zhang, X.; Lewis, A.M.; Moley, J.R.; Brestoff, J.R. A Systematic Review and Meta-Analysis of Obesity and COVID-19 Outcomes. Sci. Rep. 2021, 11, 7193.
- Booth, A.; Reed, A.B.; Ponzo, S.; Yassaee, A.; Aral, M.; Plans, D.; Labrique, A.; Mohan, D. Population Risk Factors for Severe Disease and Mortality in COVID-19: A Global Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0247461.
- Chu, Y.; Yang, J.; Shi, J.; Zhang, P.; Wang, X. Obesity Is Associated with Increased Severity of Disease in COVID-19 Pneumonia: A Systematic Review and Meta-Analysis. Eur. J. Med. Res. 2020, 25, 64.
- Mahamat-Saleh, Y.; Fiolet, T.; Rebeaud, M.E.; Mulot, M.; Guihur, A.; el Fatouhi, D.; Laouali, N.; Peiffer-Smadja, N.; Aune, D.; Severi, G. Diabetes, Hypertension, Body Mass Index, Smoking and COVID-19-Related Mortality: A Systematic Review and Meta-Analysis of Observational Studies. BMJ Open 2021, 11, e052777.
- Parohan, M.; Yaghoubi, S.; Seraji, A.; Javanbakht, M.H.; Sarraf, P.; Djalali, M. Risk Factors for Mortality in Patients with Coronavirus Disease 2019 (COVID-19) Infection: A Systematic Review and Meta-Analysis of Observational Studies. Aging Male 2020, 23, 1416–1424.
- Raeisi, T.; Mozaffari, H.; Sepehri, N.; Darand, M.; Razi, B.; Garousi, N.; Alizadeh, M.; Alizadeh, S. The Negative Impact of Obesity on the Occurrence and Prognosis of the 2019 Novel Coronavirus (COVID-19) Disease: A Systematic Review and Meta-Analysis. Eat. Weight. Disord. 2022, 27, 893–911.
- Tsankov, B.K.; Allaire, J.M.; Irvine, M.A.; Lopez, A.A.; Sauvé, L.J.; Vallance, B.A.; Jacobson, K. Severe COVID-19 Infection and Pediatric Comorbidities: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2021, 103, 246–256.
- Yang, J.; Ma, Z.; Lei, Y. A Meta-Analysis of the Association between Obesity and COVID-19. Epidemiol. Infect. 2021, 149, e11.
- Zhao, X.; Gang, X.; He, G.; Li, Z.; Lv, Y.; Han, Q.; Wang, G. Obesity Increases the Severity and Mortality of Influenza and COVID-19: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2020, 11, 595109.
- Fineberg, H.V. Pandemic Preparedness and Response—Lessons from the H1N1 Influenza of 2009. N. Engl. J. Med. 2014, 370, 1335–1342.
- Shah, N.K. H1N1 2009 Pandemic—Lessons Learnt. Indian Pediatr. 2011, 48, 363–364.
- Murphy, R.; Fragaszy, E.B.; Hayward, A.C.; Warren-Gash, C. Investigating Obesity as a Risk Factor for Influenza-like Illness during the 2009 H1N1 Influenza Pandemic Using the Health Survey for England. Influenza Other Respir. Viruses 2017, 11, 66–73.
- van Kerkhove, M.D.; Vandemaele, K.A.H.; Shinde, V.; Jaramillo-Gutierrez, G.; Koukounari, A.; Donnelly, C.A.; Carlino, L.O.; Owen, R.; Paterson, B.; Pelletier, L.; et al. Risk Factors for Severe Outcomes Following 2009 Influenza A (H1N1) Infection: A Global Pooled Analysis. PLoS Med. 2011, 8, e1001053.
- Fezeu, L.; Julia, C.; Henegar, A.; Bitu, J.; Hu, F.B.; Grobbee, D.E.; Kengne, A.-P.; Hercberg, S.; Czernichow, S. Obesity Is Associated with Higher Risk of Intensive Care Unit Admission and Death in Influenza A (H1N1) Patients: A Systematic Review and Meta-Analysis. Obes. Rev. 2011, 12, 653–659.
- Díaz, E.; Rodríguez, A.; Martin-Loeches, I.; Lorente, L.; del Mar Martín, M.; Pozo, J.C.; Montejo, J.C.; Estella, A.; Arenzana, Á.; Rello, J. Impact of Obesity in Patients Infected With 2009 Influenza A(H1N1). Chest 2011, 139, 382–386.
- Kikukawa, T.; Ogura, T.; Harasawa, T.; Suzuki, H.; Nakano, M. H1N1 Influenza-Associated Pneumonia with Severe Obesity: Successful Management with Awake Veno-Venous Extracorporeal Membrane Oxygenation and Early Respiratory Physical Therapy. Acute Med. Surg. 2016, 3, 186–189.
- Tsatsanis, C.; Margioris, A.N.; Kontoyiannis, D.P. Association between H1N1 Infection Severity and Obesity—Adiponectin as a Potential Etiologic Factor. J. Infect. Dis. 2010, 202, 459–460.
- Kwong, J.C.; Campitelli, M.A.; Rosella, L.C. Obesity and Respiratory Hospitalizations during Influenza Seasons in Ontario, Canada: A Cohort Study. Clin. Infect. Dis. 2011, 53, 413–421.
- Rojas-Osornio, S.A.; Cruz-Hernández, T.R.; Drago-Serrano, M.E.; Campos-Rodríguez, R. Immunity to Influenza: Impact of Obesity. Obes. Res. Clin. Pract. 2019, 13, 419–429.
- Atamna, A.; Elis, A.; Gilady, E.; Gitter-Azulay, L.; Bishara, J. How Obesity Impacts Outcomes of Infectious Diseases. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 585–591.
- Falagas, M.E.; Kompoti, M. Obesity and Infection. Lancet Infect. Dis. 2006, 6, 438–446.
- Karlsson, E.A.; Beck, M.A. The Burden of Obesity on Infectious Disease. Exp. Biol. Med. 2010, 235, 1412–1424.
- Kershaw, E.E.; Flier, J.S. Adipose Tissue as an Endocrine Organ. J. Clin. Endocrinol. Metab. 2004, 89, 2548–2556.
- Duffaut, C.; Galitzky, J.; Lafontan, M.; Bouloumié, A. Unexpected Trafficking of Immune Cells within the Adipose Tissue during the Onset of Obesity. Biochem. Biophys. Res. Commun. 2009, 384, 482–485.
- Liu, R.; Nikolajczyk, B.S. Tissue Immune Cells Fuel Obesity-Associated Inflammation in Adipose Tissue and Beyond. Front. Immunol. 2019, 10, 1587.
- Lu, J.; Zhao, J.; Meng, H.; Zhang, X. Adipose Tissue-Resident Immune Cells in Obesity and Type 2 Diabetes. Front. Immunol. 2019, 10, 1173.
- Mraz, M.; Haluzik, M. The Role of Adipose Tissue Immune Cells in Obesity and Low-Grade Inflammation. J. Endocrinol. 2014, 222, R113–R127.
- Schipper, H.S.; Prakken, B.; Kalkhoven, E.; Boes, M. Adipose Tissue-Resident Immune Cells: Key Players in Immunometabolism. Trends Endocrinol. Metab. 2012, 23, 407–415.
- Fernández-Sánchez, A.; Madrigal-Santillán, E.; Bautista, M.; Esquivel-Soto, J.; Morales-González, Á.; Esquivel-Chirino, C.; Durante-Montiel, I.; Sánchez-Rivera, G.; Valadez-Vega, C.; Morales-González, J.A. Inflammation, Oxidative Stress, and Obesity. Int. J. Mol. Sci. 2011, 12, 3117–3132.
- Hotamisligil, G.S. Inflammation and Endoplasmic Reticulum Stress in Obesity and Diabetes. Int. J. Obes. 2008, 32, S52–S54.
- Huh, J.Y.; Park, Y.J.; Ham, M.; Kim, J.B. Crosstalk between Adipocytes and Immune Cells in Adipose Tissue Inflammation and Metabolic Dysregulation in Obesity. Mol. Cells 2014, 37, 365–371.
- Li, H.; Meng, Y.; He, S.; Tan, X.; Zhang, Y.; Zhang, X.; Wang, L.; Zheng, W. Macrophages, Chronic Inflammation, and Insulin Resistance. Cells 2022, 11, 3001.
- Snel, M.; Jonker, J.T.; Schoones, J.; Lamb, H.; de Roos, A.; Pijl, H.; Smit, J.W.A.; Meinders, A.E.; Jazet, I.M. Ectopic Fat and Insulin Resistance: Pathophysiology and Effect of Diet and Lifestyle Interventions. Int. J. Endocrinol. 2012, 2012, 983814.
- Trouwborst, I.; Bowser, S.M.; Goossens, G.H.; Blaak, E.E. Ectopic Fat Accumulation in Distinct Insulin Resistant Phenotypes; Targets for Personalized Nutritional Interventions. Front. Nutr. 2018, 5, 77.
- Adler, B.J.; Kaushansky, K.; Rubin, C.T. Obesity-Driven Disruption of Haematopoiesis and the Bone Marrow Niche. Nat. Rev. Endocrinol. 2014, 10, 737–748.
- van den Berg, S.M.; Seijkens, T.T.P.; Kusters, P.J.H.; Beckers, L.; den Toom, M.; Smeets, E.; Levels, J.; de Winther, M.P.J.; Lutgens, E. Diet-Induced Obesity in Mice Diminishes Hematopoietic Stem and Progenitor Cells in the Bone Marrow. FASEB J. 2016, 30, 1779–1788.
- Karlsson, E.A.; Sheridan, P.A.; Beck, M.A. Diet-Induced Obesity in Mice Reduces the Maintenance of Influenza-Specific CD8+ Memory T Cells. J. Nutr. 2010, 140, 1691–1697.
- Viardot, A.; Heilbronn, L.K.; Samocha-Bonet, D.; Mackay, F.; Campbell, L.V.; Samaras, K. Obesity Is Associated with Activated and Insulin Resistant Immune Cells. Diabetes Metab. Res. Rev. 2012, 28, 447–454.
- Yang, H.; Youm, Y.-H.; Vandanmagsar, B.; Rood, J.; Kumar, K.G.; Butler, A.A.; Dixit, V.D. Obesity Accelerates Thymic Aging. Blood 2009, 114, 3803–3812.
- Fischer, H.J.; Sie, C.; Schumann, E.; Witte, A.-K.; Dressel, R.; van den Brandt, J.; Reichardt, H.M. The Insulin Receptor Plays a Critical Role in T Cell Function and Adaptive Immunity. J. Immunol. 2017, 198, 1910–1920.
- Helderman, J.H.; Strom, T.B. Specific Insulin Binding Site on T and B Lymphocytes as a Marker of Cell Activation. Nature 1978, 274, 62–63.
- Chi, H. Regulation and Function of MTOR Signalling in T Cell Fate Decisions. Nat. Rev. Immunol. 2012, 12, 325–338.
- Myers, D.R.; Wheeler, B.; Roose, J.P. MTOR and Other Effector Kinase Signals That Impact T Cell Function and Activity. Immunol. Rev. 2019, 291, 134–153.
- Tsai, S.; Clemente-Casares, X.; Zhou, A.C.; Lei, H.; Ahn, J.J.; Chan, Y.T.; Choi, O.; Luck, H.; Woo, M.; Dunn, S.E.; et al. Insulin Receptor-Mediated Stimulation Boosts T Cell Immunity during Inflammation and Infection. Cell Metab. 2018, 28, 922–934.e4.
- Yang, H.; Youm, Y.-H.; Vandanmagsar, B.; Ravussin, A.; Gimble, J.M.; Greenway, F.; Stephens, J.M.; Mynatt, R.L.; Dixit, V.D. Obesity Increases the Production of Proinflammatory Mediators from Adipose Tissue T Cells and Compromises TCR Repertoire Diversity: Implications for Systemic Inflammation and Insulin Resistance. J. Immunol. 2010, 185, 1836–1845.
- Achari, A.; Jain, S. Adiponectin, a Therapeutic Target for Obesity, Diabetes, and Endothelial Dysfunction. Int. J. Mol. Sci. 2017, 18, 1321.
- Nigro, E.; Scudiero, O.; Monaco, M.L.; Palmieri, A.; Mazzarella, G.; Costagliola, C.; Bianco, A.; Daniele, A. New Insight into Adiponectin Role in Obesity and Obesity-Related Diseases. Biomed. Res. Int. 2014, 2014, 658913.
- Jiang, Y.; Yi, C.; Yi, Y.; Jin, Q.; Kang, A.S.; Li, J.; Kumar Sacitharan, P. Adiponectin Exacerbates Influenza Infection in Elderly Individuals via IL-18. Signal Transduct. Target. Ther. 2020, 5, 32.
- Kearns, S.M.; Ahern, K.W.; Patrie, J.T.; Horton, W.B.; Harris, T.E.; Kadl, A. Reduced Adiponectin Levels in Patients with COVID-19 Acute Respiratory Failure: A Case-control Study. Physiol. Rep. 2021, 9, e14843.
- Flikweert, A.W.; Kobold, A.C.M.; van der Sar-van der Brugge, S.; Heeringa, P.; Rodenhuis-Zybert, I.A.; Bijzet, J.; Tami, A.; van der Gun, B.T.F.; Wold, K.I.; Huckriede, A.; et al. Circulating Adipokine Levels and COVID-19 Severity in Hospitalized Patients. Int. J. Obes. 2022, 47, 126–137.
- Fernández-Riejos, P.; Najib, S.; Santos-Alvarez, J.; Martín-Romero, C.; Pérez-Pérez, A.; González-Yanes, C.; Sánchez-Margalet, V. Role of Leptin in the Activation of Immune Cells. Mediat. Inflamm. 2010, 2010, 568343.
- Kim, S.Y.; Lim, J.H.; Choi, S.W.; Kim, M.; Kim, S.-T.; Kim, M.-S.; Cho, Y.S.; Chun, E.; Lee, K.-Y. Preferential Effects of Leptin on CD4 T Cells in Central and Peripheral Immune System Are Critically Linked to the Expression of Leptin Receptor. Biochem. Biophys. Res. Commun. 2010, 394, 562–568.
- Matarese, G. Leptin and the Immune System: How Nutritional Status Influences the Immune Response. Eur. Cytokine Netw. 2000, 11, 7–14.
- Procaccini, C.; la Rocca, C.; Carbone, F.; de Rosa, V.; Galgani, M.; Matarese, G. Leptin as Immune Mediator: Interaction between Neuroendocrine and Immune System. Dev. Comp. Immunol. 2017, 66, 120–129.
- de Candia, P.; Prattichizzo, F.; Garavelli, S.; Alviggi, C.; la Cava, A.; Matarese, G. The Pleiotropic Roles of Leptin in Metabolism, Immunity, and Cancer. J. Exp. Med. 2021, 218, e20191593.
- Ozata, M.; Ozdemir, I.C.; Licinio, J. Human Leptin Deficiency Caused by a Missense Mutation: Multiple Endocrine Defects, Decreased Sympathetic Tone, and Immune System Dysfunction Indicate New Targets for Leptin Action, Greater Central than Peripheral Resistance to the Effects of Leptin, and Spontaneous Correction of Leptin-Mediated Defects. J. Clin. Endocrinol. Metab. 1999, 84, 3686–3695.
- Enriori, P.J.; Evans, A.E.; Sinnayah, P.; Cowley, M.A. Leptin Resistance and Obesity. Obesity 2006, 14, 254S–258S.
- Liu, J.; Yang, X.; Yu, S.; Zheng, R. The Leptin Resistance. Adv. Exp. Med. Biol. 2018, 1090, 145–163.
- Zhou, Y.; Rui, L. Leptin Signaling and Leptin Resistance. Front. Med. 2013, 7, 207–222.
- Dixon, A.E.; Peters, U. The Effect of Obesity on Lung Function. Expert. Rev. Respir. Med. 2018, 12, 755–767.
- Salome, C.M.; King, G.G.; Berend, N. Physiology of Obesity and Effects on Lung Function. J. Appl. Physiol. 2010, 108, 206–211.
- De Sant’Anna, M., Jr.; Carvalhal, R.F.; de Oliveira, F.d.F.B.; Zin, W.A.; Lopes, A.J.; Lugon, J.R.; Guimarães, F.S. Mecânica Respiratória de Pacientes Com Obesidade Mórbida. J. Bras. Pneumol. 2019, 45, e20180311.
- Bui, D.S.; Cassim, R.; Russell, M.A.; Doherty, A.; Lowe, A.J.; Agusti, A.; Dharmage, S.C.; Lodge, C.J. Lung Function Levels Influence the Association between Obesity and Risk of COVID-19. Am. J. Respir. Crit. Care Med. 2021, 204, 1106–1108.
- Caci, G.; Albini, A.; Malerba, M.; Noonan, D.M.; Pochetti, P.; Polosa, R. COVID-19 and Obesity: Dangerous Liaisons. J. Clin. Med. 2020, 9, 2511.
- Littleton, S.W.; Tulaimat, A. The Effects of Obesity on Lung Volumes and Oxygenation. Respir. Med. 2017, 124, 15–20.
- Melo, L.C.; da Silva, M.A.M.; do Nascimento Calles, A.C. Obesity and Lung Function: A Systematic Review. Einstein 2014, 12, 120–125.
- Soyak Aytekin, E.; Sahiner, U.M.; Tuten Dal, S.; Unsal, H.; Hakverdi, O.; Oguz, B.; Ozsurekci, Y.; Sekerel, B.E.; Soyer, O. Obesity Is a Risk Factor for Decrease in Lung Function after COVID-19 Infection in Children with Asthma. Pediatr. Pulmonol. 2022, 57, 1668–1676.