Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Nicholas Geremia and Version 2 by Rita Xu.
Candida auris is considered to be an emerging fungal pathogen and is related to high mortality rates, persistent candidemia, inconsistencies in susceptibility testing results and misidentification by available commercial identification systems. Multidrug-resistant (MDR) and pandrug-resistant (PDR) strains are increasingly detected. In Europe, hospital outbreaks caused by C. auris have been reported in the United Kingdom (UK), Italy and Spain.
- Candida auris
- emerging fungal disease
- public health promotion
1. Introduction
From 2009, Candida auris has been considered to be a rising healthcare emergency worldwide. C. auris infections are related to high mortality rates, persistent candidemia, inconsistencies in susceptibility testing results and misidentification by available commercial identification systems. All this must be considered alongside a high risk of treatment failure, which complicates its management [1].
In 2009, C. auris was initially found in Japan [2][3][2,3]. However, a retrospective review of the Candida strain found C. auris in South Korea in 1996 [4]. Studies have suggested that C. auris emerged simultaneously and independently in four global regions (South Asia, East Asia, Africa and South America; also named clades I, II, III and IV, respectively). These four clades are genetically distinct [5]. Most recently, a new potential V clade was identified that was isolated from Iran [6]. In the last few years, C. auris infections have increased worldwide [1][7][1,7]. In many parts of Africa and Asia, C. auris is now considered to be endemic [8]. In addition, several outbreaks have been reported in European countries such as the United Kingdom (UK), Spain and Italy [1][8][9][10][1,8,9,10].
Multidrug-resistant (MDR) and pandrug-resistant (PDR) C. auris strains are increasingly detected worldwide. The most frequent resistance is to fluconazole (FLC), followed by amphotericin B (AMB) and voriconazole (VRC). Echinocandin remains the treatment of choice, but resistance can also affect this class of antifungal drugs [1][11][1,11].
2. Identification
C. auris was first detected in the external ear canal of a 70-year-old Japanese woman. A 26S ribosomal DNA (rDNA) D1/D2 domain analysis, 18S internal transcribed spacer (ITS) rDNA region sequences and chemotaxonomic studies showed that the newly discovered Candida species (spp.) had a close phylogenetic relationship to the Metschnikowiaceae clade, particularly with C. ruelliae and C. haemulonii [3]. A retrospective study on historical Korean isolates revealed that C. auris strains were initially misidentified as C. haemulonii [12]. A genetic analysis based on ITS 1/2 and D1/D2 sequences showed that C. auris belongs to the Metschnikowiaceae family within the Candida/Clavispora clade such as C. albicans, C. tropicalis, C. haemulonii and C. lusitaniae [3]. The misidentification of C. auris as another yeast species using conventional phenotypic and biochemical methods can be common (Table 1) [2][3][2,3]. The thermal tolerance property of growth at temperatures up to 42 °C on CHROMagarTM Candida Plus (CHROMagar, France) has been used to differentiate C. auris from other Candida spp. [13][14][13,14]. The diagnosis of C. auris infections includes biochemical-based tests such as analytical profile index strips, VITEK 2, BD Phoenix yeast identification and MicroScan. Nevertheless, these tests lack a comprehensive database for yeast identification [13]. Figure 1 shows C. auris identification.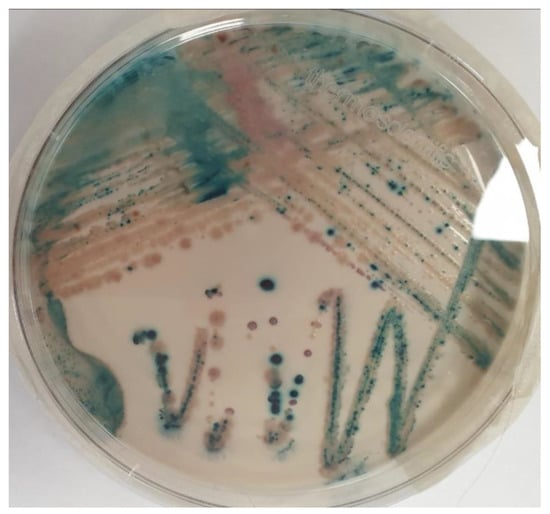
Figure 1. Candida isolates from Brilliance™ Candida Agar Base (Thermo Fisher ScientificTM, Waltham, MA, USA). C. auris (light blue with blue halo colonies), C. krusei (pink and fuzzy colonies) and C. albicans (green–blue colonies).
3. Virulence Factors
C. auris can express several virulence factors, including saps and lipases [15]. However, C. auris is less virulent than C. albicans. That characteristic was shown in murine and invertebrate G. mellonella infection models. In murine models, it was demonstrated that C. auris was much more virulent than C. glabrata and C. haemulonii [2][16][2,16]. This difference, compared with C. albicans, depended on the inability of C. auris to develop virulence factors such as hyphae or pseudohyphae, which play a critical role in tissue invasion [14]. Furthermore, C. auris is a haploid yeast whereas natural C. albicans isolates are diploid. This could have an essential role in the intrinsically low virulence of C. auris. In FLC-induced haploids, the C. albicans strain reduced their virulence compared with the diploid form [2][17][2,17]. The filamentous cells of C. auris are poorly implicated in its virulence during systemic infections, but could play a role in skin and environmental surface colonization [2].4. Antifungal Resistance
FLC and echinocandins are the most used antifungal drugs to treat candidemia. Unfortunately, FLC (or other azole) resistance is common. A recent meta-analysis from Sekyere et al. showed that the most frequent resistance was to FLC (44.29%), followed by AMB (15.46%), VRC (12.67%), caspofungin (CAS) (3.48%), flucytosine (FC) (1.95%), itraconazole (ITZ) (1.81%), isavuconazole (ISA) (1.53%), posaconazole (POS) (1.39%), anidulafungin (AFG) (1.25%) and micafungin (MFG) (1.25%) [11][12][11,12]. MDR C. auris strains have been reported in several cases, showing resistance phenotypes to FLC and AMB [18]. Resistance to echinocandins is not so frequent. Chen et al. found that the resistance rates to CAS, MFG and AFG were 12.1%, 0.8% and 1.1%, respectively. However, almost all isolates resistant to CAS were from India (23.6%) [19]. The molecular mechanism for azole resistance in C. auris is mainly related to alterations in the lanosterol demethylase enzyme, which is encoded by the ERG11 gene. C. auris can also encode ATP-binding cassette (ABC) and major facilitator superfamily (MFS) efflux pumps, which are essential mechanisms of antifungal resistance, especially during the initial stages of biofilm development. When resistance to echinocandins; occur, it is due to mutations in FKS genes that encode a subunit of the β-D-glucan synthase. Moreover, changes to the cell membrane sterol and/or a given point mutation are potential mechanisms of AMB resistance [13][20][13,20]. Unfortunately, no antifungal susceptibility breakpoints for C. auris are currently standardized for the Clinical and Laboratory Standards Institute (CLSI) and European Committee on Antimicrobial Susceptibility Testing (EUCAST). Therefore, the Centers for Disease Control and Prevention (CDC) defined a C. auris-specific antifungal susceptibility interpretation based on a close phylogenetic relationship to other Candida spp. The correlation between the microbiologic breakpoints and clinical outcomes is not known. The current breakpoints are summarized in Table 1 [21].| Antifungal | MIC | Interpretation |
|---|---|---|
| Fluconazole | ≥32 | Isolates with MIC ≥ 32 were shown to have a mutation of the Erg11 gene |
| Voriconazole | NA | Consider using fluconazole susceptibility as a surrogate for other azoles. Occasionally, isolates that are resistant to fluconazole may respond to voriconazole |
| Amphotericin B | ≥2 | Isolates with a MIC of ≥2 should be considered to be resistant |
| Anidulafungin | ≥4 | Breakpoints are based on the distribution of echinocandin MICs of approximately 100 isolates from diverse geographic locations |
| Caspofungin | ≥2 | |
| Voriconazole | ≥4 |