Therapeutic proteins, including monoclonal antibodies, single chain variable fragment (ScFv), crystallizable fragment (Fc), and fragment antigen binding (Fab), have accounted for one-third of all drugs on the world market. In particular, these medicines have been widely used in ocular therapies in the treatment of various diseases, such as age-related macular degeneration, corneal neovascularization, diabetic retinopathy, and retinal vein occlusion. The formulation of these biomacromolecules is challenging due to their high molecular weight, complex structure, instability, short half-life, enzymatic degradation, and immunogenicity, which leads to the failure of therapies. Various efforts have been made to overcome the ocular barriers, providing effective delivery of therapeutic proteins, such as altering the protein structure or including it in new delivery systems. These strategies are not only cost-effective and beneficial to patients but have also been shown to allow for fewer drug side effects. Researchers discuss several factors that affect the design of formulations and the delivery of therapeutic proteins to ocular tissues, such as the use of injectable micro/nanocarriers, hydrogels, implants, iontophoresis, cell-based therapy, and combination techniques. In addition, other approaches are briefly discussed, related to the structural modification of these proteins, improving their bioavailability in the posterior segments of the eye without affecting their stability. Future research should be conducted toward the development of more effective, stable, noninvasive, and cost-effective formulations for the ocular delivery of therapeutic proteins. In addition, more insights into preclinical to clinical translation are needed.
Therapeutic proteins, including monoclonal antibodies, single chain variable fragment (ScFv), crystallizable fragment (Fc), and fragment antigen binding (Fab), have accounted for one-third of all drugs on the world market. In particular, these medicines have been widely used in ocular therapies in the treatment of various diseases, such as age-related macular degeneration, corneal neovascularization, diabetic retinopathy, and retinal vein occlusion. However, the formulation of these biomacromolecules is challenging due to their high molecular weight, complex structure, instability, short half-life, enzymatic degradation, and immunogenicity, which leads to the failure of therapies. Various efforts have been made to overcome the ocular barriers, providing effective delivery of therapeutic proteins, such as altering the protein structure or including it in new delivery systems. These strategies are not only cost-effective and beneficial to patients but have also been shown to allow for fewer drug side effects. In this review, we discuss several factors that affect the design of formulations and the delivery of therapeutic proteins to ocular tissues, such as the use of injectable micro/nanocarriers, hydrogels, implants, iontophoresis, cell-based therapy, and combination techniques. In addition, other approaches are briefly discussed, related to the structural modification of these proteins, improving their bioavailability in the posterior segments of the eye without affecting their stability. Future research should be conducted toward the development of more effective, stable, noninvasive, and cost-effective formulations for the ocular delivery of therapeutic proteins. In addition, more insights into preclinical to clinical translation are needed.
- ocular diseases
- sustained ocular delivery
- therapeutic proteins
1. Introduction
2. Routes of Ocular Drug Administration
Achieving an efficient ocular bioavailability of different therapeutic proteins remains a challenge due to presence of multiple ocular barriers (Figure 1). Moreover, diseases such as age-related macular degeneration, diabetic retinopathy, and cytomegalovirus (CMV) retinitis require therapeutic proteins to be delivered to the back of the eye. Herein, static barriers (different layers of cornea, sclera, and retina including blood aqueous and blood–retinal barriers), dynamic barriers (choroidal and conjunctival blood flow, lymphatic clearance, and tear dilution), and efflux pumps, in combination, constitute a significant challenge for drug delivery to the posterior segment of the eye [11].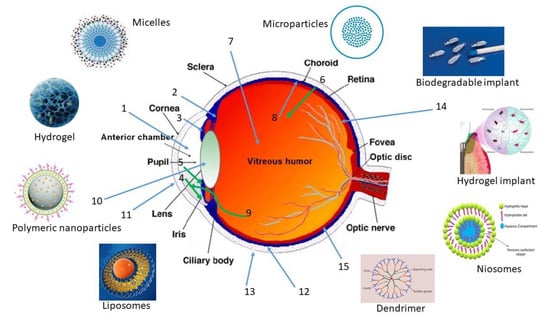
2.1. Intraocular
Intraocular delivery involves delivery through injection or implants of sterile solutions or devices in the ocular tissues via (1) intravitreal, (2) subretinal, or (3) suprachoroidal routes.- (a)
-
Intravitreal
- (b)
-
Subretinal
- (c)
-
Suprachoroidal
2.2. Periocular
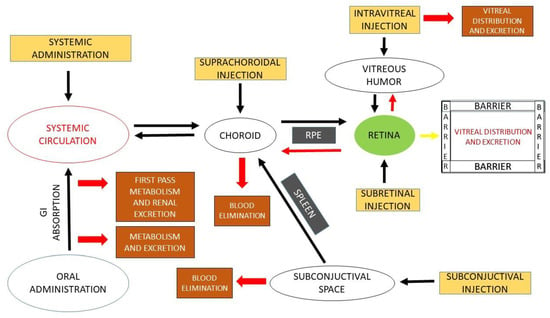
It is a less invasive method where drugs are administered directly into the eye via injection into the subconjunctival, subtenon, peribulbar, retrobulbar, and posterior juxtascleral spaces, without any risk of cataract and endophthalmitis. Compared to the topical route, this route provides excellent drug bioavailability by avoiding corneal barriers. Injected drugs reach the posterior segment through the conjunctival sclera, but the bioavailability is much lower (0.1%) than that of the topical route (Figure 2) [29]. Drugs rapidly clearing (80–95%) into systemic circulation through choroidal vessels and multiple barriers between the retina and subconjunctival space leads to poor bioavailability. This route is less invasive and eliminates the drug permeation through sclera. Moreover, in the case of retinal diseases, for drug administration in large volumes, this route is preferred due to the high volume of the injection (100–500 µL) compared with the suprachoroidal route (50–200 µL) [30].3. Ocular Barriers and Approaches to Ocular Administration
3.1. Ocular Barriers
Ocular distribution of protein therapeutics to the eye depends on several factors such as membrane permeability, ocular elimination, nontarget binding, and degradation by proteolytic enzymes. Membrane permeability and ocular elimination closely depend on their size, surface charge, and hydrophilicity and lipophilicity [31]. However, complexity of the ocular tissues in deciding parameters for ocular pharmacokinetics is a major obstacle in the designing of an effective delivery system for therapeutic proteins due to the presence of various ocular barriers.3.1.1. Tissue Conditions
Collagen fibers from the hydrophilic stroma also limit the penetration of therapeutic proteins, which usually takes place via pinocytosis or endocytosis (active transport mechanism) [31][32]. The tight junctions present in the cornea, sclera, and retina significantly prevent the diffusion of hydrophilic large macromolecules [32][33]. The tight junctions in the conjunctival epithelium are usually wider than those in the corneal epithelium but are still unable to provide penetration of large molecules [34][35]. The vitreous humor is a highly viscous fluid-like gel composed of 98 to 99% w/v water content, salts, sugars, a network of collagen-type II fibrils with hyaluronan, glycosaminoglycan, and a wide array of proteins located in the posterior segment of the ocular globe [36]. Drugs administered intravitreally will have direct access to the vitreous cavity and retina and may take several hours to diffuse across the entire vitreous humor. The clearance of macromolecules from the vitreous cavity is very slow due to hindrance by RPE, whereas diffusion from the vitreous to the retina is restricted by ILM [37]. Because several other factors are involved such as initial dose, volume of distribution, and the rate of elimination [38][39], it also depends on size, surface charge, and characteristics of the macromolecules injected [40][41][42][43]. The vitreous can allow the diffusion of small, anionic macromolecules, restricting the bigger size or cationic macromolecules that exhibit nondiffusion kinetics and distribution profile. Molecules can be eliminated through anterior and/or posterior routes [], which is influenced primarily by volume of distribution and elimination half-life [39]. A large number of diseases uveitis, cytomegalovirus retinitis, and retinitis and proliferative vitreoretinopathy affect the ocular pharmacokinetics of various topically instilled molecules and their formulations. The diseased conditions produce certain physiological changes in the corneal stroma composed of collagen and water, leading to poor bioavailability of hydrophobic molecules [44]. Fungal keratitis involving chronic inflammation of corneal tissues leads to poor permeation [45]. To solve this problem, drugs are administered with a vehicle/emulsion to avoid evaporation of the limited natural tears in dry-eye patients, as well as the use of the iontophoretic technique to permeate the ionized molecules into ocular tissues. BRB breakdown as well as choroidal and retinal neovascularization were observed in glaucoma, leading to blindness in a large population. Pharmacokinetic parameters need to be determined in such conditions using animal models to prove efficacy. In one study [46] of measuring the pharmacokinetic parameters, using healthy and diseased animal models, it was observed that the AUC and Cmax were significantly lower in diseased models compared to normal animal models due to BRB breakdown and exposure of drugs to ocular tissues. Therefore, dose calculation needs to be performed to avoid dose-related toxicity.3.1.2. Physicochemical Characteristics of Drug Molecules
Various physicochemical parameters of macromolecules such as solubility, hydrophilicity/lipophilicity, molecular weight, size and shape, surface charge, and degree of ionization affect the selection of the route and rate of drug permeation through the cul-de-sac [47]. Small and lipophilic molecules can diffuse and distribute rapidly and largely through RPE, inner limiting membrane (ILM), and outer limiting membranes (OLM), exhibiting efficient distribution to (and even faster elimination from) ocular tissues. Large and lipophilic molecules have poor membrane permeability, showing relatively longer retention time at the site of injection with poor ocular tissue distributions [48][49]. For example, the particles with a size of 200 nm were found to be retained in the retinal tissues for two months after injection [48][49]. The vitreal clearance rate is rapid for smaller particles and can also be observed from their half-lives, i.e., particles of size 50 nm, 200 nm and 2 µm showed half-lives of 5.4 ± 0.8, 8.6 ± 0.7, and 10.1 ± 1.8 days, respectively [50]. Most of the therapeutic proteins have complex structure, large size with molecular weight > 1000 Da, and large hydrogen bonding donor/acceptor groups and show poor membrane permeability across the ocular tissues and barriers [51]. Human retinal tissues prevent the permeation of macromolecules of size > 76 kDa due to inner and outer plexiform layers. Macromolecules greater than 150 kDa cannot reach the inner retinal tissues, while molecules such as brolucizumab (smaller size) can penetrate the retina and choroid tissues more effectively than other anti-VEGF [33][52]. Brolucizumab showed 2.2-fold higher concentrations in the retinal tissues and 1.7-fold higher concentrations in RPE/choroid tissues than ranibizumab in rabbits [53]. These macromolecular proteins, when traversing through the choroid, may wash out through the choriocapillaris, leading to a reduction in therapeutic concentrations, and, due to the large complex molecular structure, may increase the risk of their degradation at the physiological environment of pH and temperature resulting into shorter half-lives. Macromolecules showed half-life in the range of days to a week (Table 1) in the vitreous humor, i.e., bevacizumab had a half-life of 4.32 days with a minimum concentration of 162 μg/mL in the vitreous [54]. Frequent intravitreal injections of ranibizumab 0.3–2.0 mg/eye biweekly or monthly is required to maintain the therapeutic levels as it showed vitreous elimination of 9 days and intrinsic systemic elimination half-life of 2 h, making it noncompliant and often associated with other complications such as cataract, retinal hemorrhage, and detachment and endophthalmitis [55][56]. One comparative study showed brolucizumab clearance from the ocular tissues with a mean terminal half-life of 56.8 ± 7.6 h; ranibizumab took 62 h, and aflibercept was cleared with a half-life of 53 h in the same model [57][58][59]. The rapid clearance is presumed to be due to smaller molecular size and absence of the Fc domain in the case of brolucizumab. Unlike aflibercept, which has full-length antibodies, leading to the conservation mechanism, molecules without the Fc region are more prone to degradation and do not show a cumulative effect even after multiple injections [60]. The surface charge being a complex and heterogenous property of amino acid sequence of the therapeutic proteins along with pH of the surroundings are important criteria to be considered. Deamination, isomerization, or post-translational modification of the therapeutic proteins in a particular environment lead to formation of charge variant species in a mixture of therapeutic proteins [61]. Most therapeutic proteins are found to be positively charged at an isoelectric point (pI) of 7–9, leading to charge interactions with other molecules and ocular membranes and showing good penetration compared to negatively charged proteins [61]. Although the undesired entrapment of the polymeric network of the vitreous (negatively charged) should not be ignored, positively charged molecules tend to remain clumped in the vitreous without diffusion, while anionic particles diffuse to the retina [62][63]. The effect of surface charge on the particles was studied on human serum albumin (HSA) and showed that anionic particles of size 114 nm with an overall zeta potential of −33.3 mV can easily diffuse through the vitreal collagen fibrils to the retina within 5 h after injection, while cationic particles of size 175.5 nm with mean zeta potential of +11.7 mV showed aggregation in the vitreous [63]. An inflammatory condition of the vitreous showed accelerated diffusion and clearance of HSA [64].3.1.3. Viscosity and pH of the Formulation
Most of the protein formulations are available with high and variable viscosity as sustained release of therapeutic proteins for longer duration needs very high quantities to be injected in single-dose administration, which is often associated with high viscosity and difficulty of the syringe to handle the formulation and is not allowed by FDA. A high concentration of therapeutic proteins is very difficult to pass through an 18 mm, 27–30 G needle [65]. Use of viscosity builders required in the formulation of small molecules helps the proteins reach the anterior chamber of the eye in contrast to macromolecules, which helps provide sufficient viscosity to the formulation up to 20 cps, prolong the corneal residence time, enhance the transcorneal absorption into the anterior chamber, and thereby increase bioavailability [66]. pH and osmolarity play a vital role in the ocular therapeutics. For drug delivery to the anterior segment, maximum therapeutic benefits can be achieved when the pH of the formulation matches the lacrimal fluid. The pH of the formulation is a critical parameter that needs to be observed as proteins become denatured and unstable due to irreversible conformational changes at both high and low pH values. Apart from pH, the type and concentration of buffer used can also influence the protein degradation pathways, i.e., deamination, disulfide bond formation/exchange, isomerization, and fragmentation [67][68]. A weak acidic buffer is optimal for the storage of antibodies, i.e., adalimumab (pH 5.2), ranibizumab (pH 5.5), and bevacizumab (pH 6.2), below their isoelectric points (~8.3–8.8) for ocular treatments [69][70]. Though buffers play a crucial role in providing stability and preservation of macromolecules, their use must be carefully considered to avoid associated complications such as immunogenicity and local toxicity [71]. Buffers used also must be within the osmolarity range (280–300 mOsm/kg) to be compatible with ocular tissues as they also impair tonicity. Moreover, hypotonic solutions originate clouding and cause edema of the corneal tissues, while hypertonic solutions desiccate the corneal tissues in the anterior chamber [72]. Therefore, to facilitate protein delivery, proper understanding of the formulation pH and viscosity, selection of buffer system, and use of chemical chaperones are of the utmost importance. This helps to control the behavior and characteristics of the therapeutic proteins and also avoid protein misfolding [73][74].3.1.4. Protein Binding
Protein binding shows less effect on ocular distribution of therapeutic proteins as the level of protein in the eye (0.5–1.5 mg/mL) is significantly less compared to that of plasma (60–80 mg/mL) [75][76]. Vasotide® administered in genetically modified mouse model showed significant reduction in retinal angiogenesis in AMD [77]. Intravitreally administered molecules required to cross the ILM to reach the retina after diffusion through the vitreous body, which contains a high-density extracellular matrix made up of collagen, laminin, and heparin sulphate proteoglycan (composition changes with age), affect the drug permeability [78]. Higher drug penetration was observed with high binding affinity to the extracellular matrix, which led to effective penetration to the ILM, making the drug available to the retina. For example, adeno-associated virus serotype-2 showed excellent transduction to the retina after intravitreal injection due to high heparin sulphate proteoglycan binding affinity, while other serotypes and modified serotypes failed to transfect (low affinity with proteoglycan) [79].3.1.5. Enzymatic Degradation
Different metabolic pathways also cause the loss of therapeutic activity or inactivation of the macromolecules by protein denaturation, aggregation, precipitations, adsorption, and proteolytic degradation, denaturation by temperature, pH, salt or ionic concentrations, and complexations with enzymes/coenzymes. Enzymatic degradation by proteolytic enzymes depends on concentrations of the enzymes in the vitreous (levels may rise with age and tissue conditions) and on the hydrolytic enzymes and esterases in retina [80][81]. Structural changes in the active form of complex primary, tertiary, or quaternary structures of protein molecules or chemical modification lead to irreversible aggregation and finally inactivation. The main routes of drug administration and fate from ocular tissues are shown schematically in the Figure 1 and Figure 2, respectively. Peptides are highly susceptible to enzymatic degradation (proteolytic cleavage) [82]. The proteolytic cleavage and breakdown to small peptides leads to lower half-lives. The drug pharmacokinetic properties and thereby therapeutic efficacy can be achieved by improving bioavailability to the ocular tissues, and that can be achieved by chemical or physical modification of the molecules using various formulation strategies, i.e., coadministration, conjugation of functional moieties, particle formulation, encapsulation into implant or hydrogel, and chemical modification/substitutions. Proteolytic stabilization of macromolecules and membrane permeability can be achieved by a prodrug approach or using biological analogues [31][83][84]. Similarly, lipophilicity or hydrophobicity can also be increased by covalent conjugation with hydrophobic moiety or by noncovalent interactions with any hydrophobic compound. Solubility improvements can also be achieved using a conjugation with cyclodextrin and PEG, eliminating enzymatic degradation [15][16][32][51]. Thus, the pharmacokinetic properties of therapeutic proteins can be optimized, keeping in mind these changes must not affect their biological efficacy. Therapeutic proteins need protection against enzymatic attack from the various proteolytic enzymes present in the vitreous such as matrix metalloproteinase and serine/cysteine protease. The level of enzyme concentration in the vitreous changes with the age and disease conditions, so the formulation targeted to the retinal diseases needs to be optimized against such enzymatic attack [85][86]. Use of D-form peptides or peptoid type has been shown to have good enzymatic resistance [87] in addition to chemical modifications at the N and C terminus; for example, C-terminal amidation or N-terminal acetylation will make the peptides more difficult to be recognized and targeted by the enzymatic attack [88][89]. Apart from proteolytic enzymes, certain metabolic enzymes such as cytochrome P450 reductases and lysosomal enzymes are also found in large amounts in the ocular tissues that maintain homeostasis and protect the ocular tissues [90][91][92]. Encapsulation of retinal drugs in a nanoparticulate system or implant matrix can improve the protection against the enzymatic degradation [93], as discussed later in formulation approaches.3.2. Use of Penetration Enhancers
Different therapeutic approaches have been investigated for the improvement of drug bioavailability and providing sustained drug release to the corneal tissues. Bioavailability improvement to the anterior segment of the eye can be achieved by maximizing corneal absorption and reduction in precorneal drug loss, which can be achieved by using viscosity enhancers, penetration enhancers, and prodrug approaches [56][57][58]. The presence of tight junctions in the stratified epithelium allows only ions to be transported across the tissues, offering high resistance to therapeutic proteins; thus, the addition of absorption promotors or penetration enhancers can be more helpful to improve the permeability across the corneal tissues or membrane [29][57][94]. Permeation enhancers alter the integrity of the corneal epithelium, leading to the promotion of the corneal uptake and thus a rate-limiting step in the transport of macromolecules from the corneal tissues to the receptor site [58]. Inclusion of cetylpyridinium chloride [95], lasalocid [96], benzalkonium chloride [52], parabens [94], tween® 20, saponins [40], Brij® 35, Brij® 78, Brij® 98 ethylenediaminetetraacetic acid, bile salts [59], bile acids (such as sodium cholate, sodium taurocholate, sodium glycodeoxycholate, sodium taurodeoxycholate, taurocholic acid, chenodeoxycholic acid, and ursodeoxycholic acid), capric acid, azone, fusidic acid, hexamethylene lauramide, saponins [60], hexamethylene octanamide, and decyl methyl sulfoxide [97] in different formulations has shown a significant enhancement of corneal drug absorption. Moreover, the ability to catalyze the degradation of hyaluronic acid by hyaluronidase is also utilized since it has taken decades to improve the permeability across the ocular tissue barriers [98]. In the vitreous, hyaluronic acid provides a key role in maintaining structural integrity, volume expansion, and viscosity of the vitreous body [99]. Keeping in mind the associated toxicity and irritation, penetration enhancers should be used precisely and carefully.
References
- Sharma, D.S.; Wadhwa, S.; Gulati, M.; Ramanunny, A.K.; Awasthi, A.; Singh, S.K.; Khursheed, R.; Corrie, L.; Chitranshi, N.; Gupta, V.K.; et al. Recent advances in intraocular and novel drug delivery systems for the treatment of diabetic retinopathy. Expert Opin. Drug Del. 2021, 18, 553–576.
- Kim, H.M.; Woo, S.J. Ocular Drug Delivery to the Retina: Current Innovations and Future Perspectives. Pharmaceutics 2021, 13, 108.
- Bourne, R.R.A.; Flaxman, S.R.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; Leasher, J.; Limburg, H.; et al. Vision Loss Expert Group. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e888–e897.
- Claudio, F.; Francesco, B.; Michele, R.; Giovanni, A. Intravitreal Therapy for Diabetic Macular Edema: An Update. J. Ophthalmol. 2021, 2021, 6654168.
- Aiello, L.P. The potential role of PKC b in diabetic retinopathy and macular edema. Survey Ophthalmol. 2002, 47 (Suppl. S2), 263–269.
- Alqahtani, F.Y.; Aleanizy, F.S.; El Tahir, E.; Alquadeib, B.T.; Alsarra, I.A.; Alanazi, J.S.; Abdelhady, H.G. Preparation, characterization, and antibacterial activity of diclofenac-loaded chitosan nanoparticles. Saudi Pharm. J. 2019, 27, 82–87.
- Hu, J.; Zhang, Y.; Li, X.; Han, W.; Zheng, J.; Yang, G.; Xu, A. Combination of Intrastromal and Intracameral Injections of Amphotericin B in the Treatment of Severe Fungal Keratitis. J. Ophthalmol. 2016, 2016, 3436415.
- Patel, P.B.; Shastri, D.H.; Shelat, P.K.; Shukla, A.K. Ophthalmic drug delivery system: Challenges and approaches. Syst. Rev. Pharm. 2010, 1, 113–120.
- Liu, W.; Borrell, M.A.; Venerus, D.C.; Mieler, W.F.; Kang-Mieler, J.J. Characterization of Biodegradable Microsphere-Hydrogel Ocular Drug Delivery System for Controlled and Extended Release of Ranibizumab. Transl. Vis. Sci. Technol. 2019, 8, 12.
- Narayana, S.; Ahmed, M.G.; Gowda, J.B.H.; Shetty, P.K.; Nasrine, A.; Thriveni, M.; Noushida, N.; Sanjana, A. Recent advances in ocular drug delivery systems and targeting VEGF receptors for management of ocular angiogenesis: A comprehensive review. Future J. Pharm. Sci. 2021, 7, 186.
- Chen, W.; Yung, B.C.; Qian, Z.; Chen, X. Improving Long-Term Subcutaneous Drug Delivery by Regulating Material-Bioenvironment Interaction. Adv. Drug Deliv. Rev. 2018, 127, 20–34.
- Renukuntla, J.; Vadlapudi, A.D.; Patel, A.; Boddu, S.H.S.; Mitra, A.K. Approaches for Enhancing Oral Bioavailability of Peptides and Proteins. Int. J. Pharm. 2013, 447, 75–93.
- Faulds, D.; Goa, K.L.; Benfield, P. Cyclosporin. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic use in immunoregulatory disorders. Drugs 1993, 45, 953–1040.
- Brown, L.R. Commercial Challenges of Protein Drug Delivery. Expert Opin. Drug Deliv. 2005, 2, 29–42.
- Bhattacharya, M.; Sadeghi, A.; Sarkhel, S.; Hagström, M.; Bahrpeyma, S.; Toropainen, E.; Auriola, S.; Urtti, A. Release of functional dexamethasone by intracellular enzymes: A modular peptide-based strategy for ocular drug delivery. J. Control. Release 2020, 327, 584–594.
- Haddadzadegan, S.; Dorkoosh, F.; Bernkop-Schnürch, A. Oral delivery of therapeutic peptides and proteins: Technology landscape of lipid-based nanocarriers. Adv. Drug Deliv. Rev. 2022, 182, 114097.
- Lin, J. Pharmacokinetics of Biotech Drugs: Peptides, Proteins and Monoclonal Antibodies. Curr. Drug Metab. 2009, 10, 661–691.
- Ahmed, I.; Patton, T.F. Disposition of Timolol and Inulin in the Rabbit Eye Following Corneal versus Non-Corneal Absorption. Int. J. Pharm. 1987, 38, 9–21.
- Donovan, M.D.; Flynn, G.L.; Amidon, G.L. Absorption of Polyethylene Glycols 600 Through 2000: The Molecular Weight Dependence of Gastrointestinal and Nasal Absorption. Pharm. Res. Off. J. Am. Assoc. Pharm. Sci. 1990, 7, 863–868.
- Shen, W.; Matsui, T. Intestinal Absorption of Small Peptides: A Review. Int. J. Food Sci. Technol. 2019, 54, 1942–1948.
- Xu, Q.; Boylan, N.J.; Suk, J.S.; Wang, Y.Y.; Nance, E.A.; Yang, J.C.; McDonnell, P.J.; Cone, R.A.; Duh, E.J.; Hanes, J. Nanoparticle Diffusion in, and Microrheology of, the Bovine Vitreous Ex Vivo. J. Control. Release 2013, 167, 76–84.
- Xu, J.; Heys, J.J.; Barocas, V.H.; Randolph, T.W. Permeability and Diffusion in Vitreous Humor: Implications for Drug Delivery. Pharm. Res. 2000, 17, 664–669.
- Balachandran, R.K.; Barocas, V.H. Contribution of Saccadic Motion to Intravitreal Drug Transport: Theoretical Analysis. Pharm. Res. 2011, 28, 1049–1064.
- Käsdorf, B.T.; Arends, F.; Lieleg, O. Diffusion Regulation in the Vitreous Humor. Biophys. J. 2015, 109, 2171–2181.
- Nakano, M.; Lockhart, C.M.; Kelly, E.J.; Rettie, A.E. Ocular Cytochrome P450s and Transporters: Roles in Disease and Endobiotic and Xenobiotic Disposition. Drug Metab. Biophys. J. Rev. 2014, 46, 247–260.
- Urtti, A. Nanostructures Overcoming the Ocular Barrier: Drug Delivery Strategies; Chapter 4.2.; Royal Society of Chemistry: London, UK, 2012; pp. 190–204.
- DiCarlo, J.E.; Mahajan, V.B.; Tsang, S.H. Gene therapy and genome surgery in the retina. J. Clin. Investig. 2018, 128, 2177–2188.
- Sørensen, N.B. Subretinal Surgery: Functional and Histological Consequences of Entry into the Subretinal Space. Acta Ophthalmol. 2019, 97, 1–23.
- Subrizi, A.; del Amo, E.M.; Korzhikov-Vlakh, V.; Tennikova, T.; Ruponen, M.; Urtti, A. Design Principles of Ocular Drug Delivery Systems: Importance of Drug Payload, Release Rate, and Material Properties. Drug Discov. Today. 2019, 24, 1446–1457.
- Bachu, R.D.; Chowdhury, P.; Al-Saedi, Z.H.F.; Karla, P.K.; Boddu, S.H.S. Ocular Drug Delivery Barriers-Role of Nanocarriers in the Treatment of Anterior Segment Ocular Diseases. Pharmaceutics 2018, 10, 28.
- Muheem, A.; Shakeel, F.; Jahangir, M.A.; Anwar, M.; Mallick, N.; Jain, G.K.; Warsi, M.H.; Ahmad, F.J. A review on the strategies for oral delivery of proteins and peptides and their clinical perspectives. Saudi Pharm. J. 2016, 24, 413–428.
- Leclercq, B.; Mejlachowicz, D.; Behar-Cohen, F. Ocular Barriers and Their Influence on Gene Therapy Products Delivery. Pharmaceutics 2022, 14, 998.
- Tao, Y.; Li, X.X.; Jiang, Y.R.; Bai, X.B.; Wu, B.D.; Dong, J.Q. Diffusion of macromolecule through retina after experimental branch retinal vein occlusion and estimate of intraretinal barrier. Curr. Drug Metab. 2007, 8, 151–156.
- Jackson, T.L.; Antcliff, R.J.; Hillenkamp, J.; Marshall, J. Human retinal molecular weight exclusion limit and estimate of species variation. Investig. Ophthalmol. Vis. Sci. 2003, 44, 2141–2146.
- Blessing, C.I.; Charis, R.; Roel, F.M.; Mio, T.; Mei, C.; Wim, E.H. Hyaluronic Acid-PEG-Based Diels–Alder In Situ Forming Hydrogels for Sustained Intraocular Delivery of Bevacizumab. Biomacromolecules 2022, 23, 1525–7797.
- Burgalassi, S.; Monti, D.; Nicosia, N.; Tampucci, S.; Terreni, E.; Vento, A.; Chetoni, P. Freeze-dried matrices for ocular administration of bevacizumab: A comparison between subconjunctival and intravitreal administration in rabbits. Drug Deliv. Transl. Res. 2018, 8, 461–472.
- Urtti, A. Challenges and obstacles of ocular pharmacokinetics and drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1131–1135.
- Levison, M.E.; Levison, J.H. Pharmacokinetics and pharmacodynamics of antibacterial agents. Infect. Dis. Clini. N. Am. 2009, 23, 791–815.
- Del Amo, E.M.; Urtti, A. Rabbit as an animal model for intravitreal pharmacokinetics: Clinical predictability and quality of the published data. Exp. Eye. Res. 2015, 137, 111–124.
- Sidman, R.L.; Li, J.; Lawrence, M.; Hu, W.; Musso, G.F.; Giordano, R.J.; Cardo-Vila, M.; Pasqualini, R.; Arap, W. The peptidomimetic Vasotide targets two retinal VEGF receptors and reduces pathological angiogenesis in murine and nonhuman primate models of retinal disease. Sci. Transl. Med. 2015, 7, 309.
- Pescina, S.; Ferrari, G.; Govoni, P.; Macaluso, C.; Padula, C.; Santi, P.; Nicoli, S. In-vitro permeation of bevacizumab through human sclera: Effect of iontophoresis application. J. Pharm. Pharmacol. 2010, 62, 1189–1194.
- Swami, R.; Shahiwala, A. Impact of physiochemical properties on pharmacokinetics of protein therapeutics. Eur. J. Drug Metab. Pharmacokinetics. 2013, 38, 231–239.
- Kuo, T.T.; Baker, K.; Yoshida, M.; Qiao, S.W.; Aveson, V.G.; Lencer, W.I.; Blumberg, R.S. Neonatal Fc receptor: From immunity to therapeutics. J. Clin. Immunol. 2010, 30, 777–789.
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular Drug Delivery. AAPS J. 2010, 12, 348–360.
- Edelhauser, H.F.; Rowe-Rendleman, C.L.; Robinson, M.R.; Dawson, D.G.; Chader, G.J.; Grossniklaus, H.E. Ophthalmic drug delivery systems for the treatment of retinal diseases: Basic research to clinical applications. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5403–5420.
- Shen, J.; Durairaj, C.; Lin, T.; Liu, Y.; Burke, J. Ocular pharmacokinetics of intravitreally administered brimonidine and dexamethasone in animal models with and without blood-retinal barrier breakdown. Investig. Ophthalmol. Vis. Sci. 2014, 55, 1056–1066.
- Kim, Y.C.; Chiang, B.; Wu, X.; Prausnitz, M.R. Ocular delivery of macromolecules. J. Con. Rel. 2014, 190, 172–181.
- Joseph, R.R.; Venkatraman, S.S. Drug delivery to the eye: What benefits do nanocarriers offer? Nanomedicine 2017, 12, 683–702.
- Raghava, S.; Hammond, M.; Ub, K. Periocular routes for retinal drug delivery. Expert Opin. Drug Deliv. 2004, 1, 99–114.
- Puddu, A.; Sanguineti, R.; Montecucco, F.; Viviani, G.L. Retinal pigment epithelial cells express a functional receptor for glucagon-like peptide-1 (GLP-1). Mediat. Inflamm. 2013, 2013, 975032.
- Zelikin, A.N.; Ehrhardt, C.; Healy, A.M. Materials and methods for delivery of biological drugs. Nat. Chem. 2016, 8, 997–1007.
- Chang, J.H.; Garg, N.K.; Lunde, E.; Han, K.Y.; Jain, S.; Azar, D.T. Corneal neovascularization: An anti-VEGF therapy review. Surv. Ophthalmol. 2012, 57, 415–429.
- Vinores, S.A. Pegaptanib in the treatment of wet, age-related macular degeneration. Int. J. Nanomed. 2006, 1, 263–268.
- Joseph, M.; Trinh, H.M.; Cholkar, K.; Pal, D.; Mitra, A.K. Recent perspectives on the delivery of biologics to back of the eye. Expert Opin. Drug Deliv. 2016, 14, 631–645.
- Xu, L.; Lu, T.; Tuomi, L.; Jumbe, N.; Lu, J.; Eppler, S.; Kuebler, P.; Damico-Beyer, L.A.; Joshi, A. Pharmacokinetics of ranibizumab in patients with neovascular age-related macular degeneration: A population approach. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1616–1624.
- Vaishya, R.D.; Khurana, V.; Patel, S.; Mitra, A.K. Controlled ocular drug delivery with nanomicelles, Wiley interdisciplinary reviews. Nanomed. Nanobiotechnol. 2014, 6, 422–437.
- Moisseiev, E.; Waisbourd, M.; Ben-Artsi, E.; Levinger, E.; Barak, A.; Daniels, T.; Csaky, K.; Loewenstein, A.; Barequet, I.S. Pharmacokinetics of bevacizumab after topical and intravitreal administration in human eyes. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 331–337.
- Sharma, Y.R.; Venkatesh, P.; Gogia, V. Aflibercept—How does it compare with other Anti-VEGF Drugs? Aust. J. Clin. Ophthalmol. 2014, 1, 1–8.
- Neri, P.; Lettieri, M.; Fortuna, C.; Zucchi, M.; Manoni, M.; Celani, S.A. Giovannini, Adalimumab (humira) in ophthalmology: A review of the literature. Middle East Afr. J. Ophthalmol. 2010, 17, 290–296.
- Rodrigues, E.B.; Farah, M.E.; Maia, M.; Penha, F.M.; Regatieri, C.; Melo, G.B.; Pinheiro, M.M.; Zanetti, C.R. Therapeutic monoclonal antibodies in ophthalmology. Prog. Ret. Eye Res. 2009, 28, 117–144.
- Khawli, L.A.; Goswami, S.; Hutchinson, R.; Kwong, Z.W.; Yang, J.; Wang, X.; Yao, Z.; Sreedhara, A.; Cano, T.; Tesar, D. Charge variants in IgG1: Isolation, characterization, In vitro binding properties and pharma-cokinetics in rats. MAbs 2010, 2, 613–624.
- Maurice, D.M.; Watson, P.G. The distribution and movement of serum albumin in the cornea. Exp. Eye Res. 1965, 4, 355–363.
- Kim, J.H.; Green, K.; Martinez, M.; Paton, D. Solute permeability of the corneal endothelium and Descemet’s membrane. Exp. Eye Res. 1971, 12, 231–238.
- Olsen, T.W.; Edelhauser, H.F.; Lim, J.I.; Geroski, D.H. Human scleral permeability. Effects of age, cryotherapy, transscleral diode laser, and surgical thinning. Investig. Ophthalmol. Vis. Sci. 1995, 36, 1893–1903.
- Mitragotri, S.; Burke, P.A.; Langer, R. Overcoming the challenges in administering biopharmaceuticals: Formulation and delivery strategies. Nat. Rev. Drug Discov. 2014, 13, 655–672.
- Duvvuri, S.; Majumdar, S.; Mitra, A.K. Drug delivery to the retina: Challenges and opportunities. Expert Opin. Biol. Ther. 2003, 3, 45–56.
- Manning, M.C.; Chou, D.K.; Murphy, B.M.; Payne, R.W.; Katayama, D.S. Stability of protein pharmaceuticals: An update. Pharm. Res. 2010, 27, 544–575.
- Li, S.K.; Liddell, M.R.; Wen, H. Effective electrophoretic mobilities and charges of anti-VEGF proteins determined by capillary zone electrophoresis. J. Pharm. Biomed. Anal. 2011, 55, 603–607.
- Kaja, S.; Hilgenberg, J.D.; Everett, E.; Olitsky, S.E.; Gossage, J.; Koulen, P. Effects of dilution and prolonged storage with preservative in a polyethylene container on Bevacizumab (Avastin) for topical delivery as a nasal spray in anti-hereditary hemorrhagic telangiectasia and related therapies. Hum. Antibodies 2011, 20, 95–101.
- Gregoritza, M.; Messmann, V.; Abstiens, K.; Brandl, F.P.; Goepferich, A.M. Controlled antibody release from degradable thermoresponsive hydrogels cross-linked by Diels-Alder chemistry. Biomacromolecules 2017, 18, 2410–2418.
- Jani, R.; Lang, J.; Rodeheaver, D.; Missel, P.; Roehrs, R.; Chowhan, M. Design and Evaluation of Ophthalmic Pharmaceutical Products, Modern Pharmaceutics, 4th ed.; CRC Press: Boca Raton, FL, USA, 2002.
- Ali, Y.; Lehmussaari, K. Industrial perspective in ocular drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1258–1268.
- Subrizi, A.; Toropainen, E.; Ramsay, E.; Airaksinen, A.J.; Kaarniranta, K.; Urtti, A. Oxidative stress protection by exogenous delivery of rhHsp70 chaperone to the retinal pigment epithelium (RPE), a possible therapeutic strategy against RPE degeneration. Pharm. Res. 2015, 32, 211–221.
- Schymkowitz, J.; Rousseau, F. Protein aggregation: A rescue by chaperones. Nat. Chem. Biol. 2016, 12, 58–59.
- Angi, M.; Kalirai, H.; Coupland, S.E.; Damato, B.E.; Semeraro, F.; Romano, M.R. Proteomic Analyses of the Vitreous Humour. Mediat. Inflamm. 2012, 2012, 148039.
- Murthy, K.R.; Goel, R.; Subbannayya, Y.; Jacob, H.K.C.; Murthy, P.R.; Manda, S.S.; Patil, A.H.; Sharma, R.; Sahasrabuddhe, N.A.; Parashar, A.; et al. Proteomic Analysis of Human Vitreous Humor. Clin. Proteom. 2014, 11, 29.
- Babizhayev, M.A.; Burke, L.; Micans, P.; Richer, S.P. N-Acetylcarnosine Sustained Drug Delivery Eye Drops to Control the Signs of Ageless Vision: Glare Sensitivity, Cataract Amelioration and Quality of Vision Currently Available Treatment for the Challenging 50,000-Patient Population. Clin. Interv. Aging 2009, 4, 31–50.
- Peynshaert, K.; Devoldere, J.; Minnaert, A.K.; De Smedt, S.C.; Remaut, K. Morphology and Composition of the Inner Limiting Membrane: Species-Specific Variations and Relevance toward Drug Delivery Research. Curr. Eye Res. 2019, 44, 465–475.
- Boye, S.L.; Bennett, A.; Scalabrino, M.L.; McCullough, K.T.; Van Vliet, K.; Choudhury, S.; Ruan, Q.; Peterson, J.; Agbandje-McKenna, M.; Boye, S.E. Impact of Heparan Sulfate Binding on Transduction of Retina by Recombinant Adeno-Associated Virus Vectors. J. Virol. 2016, 90, 4215–4231.
- Bisht, R.; Rupenthal, I.D.; Sreebhavan, S.; Jaiswal, J.K. Development of a Novel Stability Indicating RP-HPLC Method for Quantification of Connexin43 Mimetic Peptide and Determination of Its Degradation Kinetics in Biological Fluids. J. Pharm. Anal. 2017, 7, 365–373.
- Stampfli, H.F.; Quon, C.Y. Polymorphic metabolism of flestolol and other ester containing compounds by a carboxylesterase in New Zealand white rabbit blood and cornea. Res. Commun. Mol. Pathol. Pharmacol. 1995, 88, 87–97.
- Fosgerau, K.; Hoffmann, T. Peptide Therapeutics: Current Status and Future Directions. Drug Discov. Today 2015, 20, 122–128.
- Ambati, J.; Atkinson, J.P.; Gelfand, B.D. Immunology of age-related macular degeneration. Nat. Rev. Immunol. 2013, 13, 438–451.
- Radhakrishnan, K.; Sonali, N.; Moreno, M.; Nirmal, J.; Fernandez, A.A.; Venkatraman, S.; Agrawal, R. Protein delivery to the back of the eye: Barriers, carriers and stability of anti-VEGF proteins. Drug Discov. Today. 2017, 22, 416–423.
- Vaughan-Thomas, A.; Gilbert, S.J.; Duance, V.C. Elevated levels of proteolytic enzymes in the aging human vitreous. Investig. Ophthalmol. Vis. Sci. 2000, 41, 3299–3304.
- Pescosolido, N.; Barbato, A.; Pascarella, A.; Giannotti, R.; Genzano, M.; Nebbioso, M. Role of Protease-Inhibitors in Ocular Diseases. Molecules 2014, 19, 20557–20569.
- Jwala, J.; Boddu, S.H.S.; Shah, S.; Sirimulla, S.; Pal, D.; Mitra, A.K. Ocular Sustained Release Nanoparticles Containing Stereoiso-meric Dipeptide Prodrugs of Acyclovir. J. Ocul. Pharmacol. Ther. 2011, 27, 163–172.
- Brinckerhoff, L.H.; Kalashnikov, V.V.; Thompson, L.W.; Yamshchikov, G.V.; Pierce, R.A.; Galavotti, H.S.; Engelhard, V.H.; Slingluff, C.L. Terminal Modifications Inhibit Proteolytic Degradation of an Immunogenic MART-127-35 Peptide: Implications for Peptide Vaccines. Int. J. Cancer 1999, 83, 326–334.
- Werle, M.; Bernkop-Schnürch, A. Strategies to Improve Plasma Half Life Time of Peptide and Protein Drugs. Amino Acids 2006, 30, 351–367.
- Attar, M.; Shen, J.; Ling, K.H.J.; Tang-Liu, D. Ophthalmic Drug Delivery Considerations at the Cellular Level: Drug-Metabolising Enzymes and Transporters. Expert Opin. Drug Deliv. 2005, 2, 891–908.
- Schwartzman, M.L.; Masferrer, J.; Dunn, M.W.; Mcgiff, J.C.; Abraham, N.G. Cytochrome P450, Drug Metabolizing Enzymes and Arachidonic Acid Metabolism in Bovine Ocular Tissues. Curr. Eye Res. 1987, 6, 623–630.
- Hayasaka, S. Lysosomal Enzymes in Ocular Tissues and Diseases. Surv. Ophthalmol. 1983, 27, 245–258.
- Vandervoort, J.; Ludwig, A. Ocular Drug Delivery: Nanomedicine Applications. Nanomedicine 2007, 2, 11–21.
- Ferrara, N.; Adamis, A. Ten years of anti-vascular endothelial growth factor therapy. Nat. Rev. Drug. Discov. 2016, 15, 385–403.
- Traynor, K. Aflibercept approved for macular degeneration. Am. J. Health Sys. Pharm. 2012, 69, 6.
- Ng, E.W.; Shima, D.T.; Calias, P.; Cunningham, E.T.; Guyer, D.R.; Adamis, A.P. Pegaptanib, a targeted anti-VEGF aptamer for ocular vascular disease. Nat. Rev. Drug Discov. 2006, 5, 123–132.
- Theodossiadis, P.G.; Markomichelakis, N.N.; Sfikakis, P.P. Tumor necrosis factor antagonists: Preliminary evidence for an emerging approach in the treatment of ocular inflammation. Retina 2007, 27, 399–413.
- Harooni, M.; Freilich, J.M.; Abelson, M.; Refojo, M. Efficacy of hyaluronidase in reducing increases in intraocular pressure related to the use of viscoelastic substances. Arch. Ophthalmol. 1998, 116, 1218–1221.
- Stern, R.; Jedrzejas, M.J. Hyaluronidases: Their genomics, structures, and mechanisms of action. Chem. Rev. 2006, 106, 818–839.